Download as pdf or txt
You might also like
- Ebook Electromyography and Neuromuscular Disorders Clinical Electrophysiologic Ultrasound Correlations PDF Full Chapter PDFDocument68 pagesEbook Electromyography and Neuromuscular Disorders Clinical Electrophysiologic Ultrasound Correlations PDF Full Chapter PDFhelen.reid678100% (33)
- Examination QuestionsDocument5 pagesExamination QuestionsVishva Lalitbhai HirparaNo ratings yet
- Surgery OralDocument39 pagesSurgery OralVishva Lalitbhai HirparaNo ratings yet
- Auriculotherapy For Respiratory DisordersDocument3 pagesAuriculotherapy For Respiratory DisordersCarissa Nichols100% (3)
- Short Bowel SyndromeDocument50 pagesShort Bowel SyndromeAbdul QadirNo ratings yet
- Chapter 43 Drugs Affecting Blood PressureDocument43 pagesChapter 43 Drugs Affecting Blood PressureHannah Lorraine GamayonNo ratings yet
- Blood Collection TubesDocument4 pagesBlood Collection TubesJilajeet Goswami100% (2)
- Asthma: A. DefinitionDocument6 pagesAsthma: A. DefinitionElvando SimatupangNo ratings yet
- AsmaDocument34 pagesAsmaRiselena Alyssa AmaDheaNo ratings yet
- Management of Asthma Attacks in Childhood AsthmaDocument43 pagesManagement of Asthma Attacks in Childhood AsthmaGilankNo ratings yet
- Asthma Management: Abdul Moeloek General HospitalDocument37 pagesAsthma Management: Abdul Moeloek General Hospitalkarina azlia amandaNo ratings yet
- Supplementary Material 1a Acute AsthmaDocument3 pagesSupplementary Material 1a Acute AsthmaANGELIE CRISTINE POMADONo ratings yet
- Asthma Management: Abdul Moeloek General HospitalDocument37 pagesAsthma Management: Abdul Moeloek General HospitalCaesarioNo ratings yet
- Kuliah AsmaattackDocument43 pagesKuliah AsmaattacksusnariahmadNo ratings yet
- AsthmaDocument44 pagesAsthmaEmmaNo ratings yet
- Lecture 06. Bronchial AsthmaDocument30 pagesLecture 06. Bronchial AsthmaJavier SaadNo ratings yet
- Obstructive Airway and Pulmonary Disease - Dr. Ahmad RasyidDocument95 pagesObstructive Airway and Pulmonary Disease - Dr. Ahmad Rasyidanisia ayundaNo ratings yet
- Asthma: Presentation By: Dr. Zunaira Nawaz Dr. Nida ShafiqueDocument47 pagesAsthma: Presentation By: Dr. Zunaira Nawaz Dr. Nida ShafiqueMohammad AliNo ratings yet
- ASTHMADocument26 pagesASTHMALe RobertNo ratings yet
- Bab Ii Tinjauan Pustaka: 2.1. Serangan Asma Akut 2.1.1. DefinisiDocument25 pagesBab Ii Tinjauan Pustaka: 2.1. Serangan Asma Akut 2.1.1. DefinisiOnes PizzahutNo ratings yet
- Two in One Disease: Asthma: Respiratory Disease That Can Have AttackDocument50 pagesTwo in One Disease: Asthma: Respiratory Disease That Can Have AttackkeiylumbantoruanNo ratings yet
- Bronchial Asthma: Mariam Lwasa Naluwugge Afrah 215-083011-07387Document25 pagesBronchial Asthma: Mariam Lwasa Naluwugge Afrah 215-083011-07387NinaNo ratings yet
- G IN A: Lobal Itiative For SthmaDocument66 pagesG IN A: Lobal Itiative For SthmaNerissaArvianaShintaraNo ratings yet
- Pharmacotherapy of AsthmaDocument53 pagesPharmacotherapy of AsthmaStella Aprilia NurNo ratings yet
- Supplementary Material 1a Acute AsthmaDocument3 pagesSupplementary Material 1a Acute AsthmaJanela Chriselle B. TICARNo ratings yet
- Asma Current Family MedicineDocument7 pagesAsma Current Family MedicineRay Erick RamosNo ratings yet
- 4 AsthmaDocument32 pages4 AsthmaSalman KhanNo ratings yet
- Asthma & UpdatesDocument74 pagesAsthma & Updatesnowrin05273815No ratings yet
- Asthma Bronchiale: Dr. Ramelan Navy Hospital SurabayaDocument53 pagesAsthma Bronchiale: Dr. Ramelan Navy Hospital SurabayaCornelia CindyNo ratings yet
- Obstructive Pulmonary DiseasesDocument50 pagesObstructive Pulmonary DiseasesGopala HariNo ratings yet
- Bronchial Asthma 2.0Document53 pagesBronchial Asthma 2.0Minhajul AbedinNo ratings yet
- 10th Tutorial - Asthma Bronchiale WebDocument75 pages10th Tutorial - Asthma Bronchiale WebFety FatimahNo ratings yet
- EMD2 - K8 - Acute Severe Asthma AttackDocument34 pagesEMD2 - K8 - Acute Severe Asthma AttackJessica WijayaNo ratings yet
- Bronchial Asthma in ChildrenDocument19 pagesBronchial Asthma in ChildrenIvanNo ratings yet
- Bronchial AsthmaDocument46 pagesBronchial AsthmaKhor Kee GuanNo ratings yet
- Pharmacology 312: Assignment 3: Respiratory DiseasesDocument5 pagesPharmacology 312: Assignment 3: Respiratory DiseasesTerepe CrimsonNo ratings yet
- Integrated Therapeutics IiiDocument91 pagesIntegrated Therapeutics IiiSalahadinNo ratings yet
- Review Class Internal MedicineDocument216 pagesReview Class Internal MedicinekashifNo ratings yet
- Asthma: Treatment and ManagementDocument54 pagesAsthma: Treatment and ManagementEndah susantiNo ratings yet
- Asthma and COPDDocument79 pagesAsthma and COPDDawit g/kidanNo ratings yet
- Dr. Sak Indriyani, Spa, Mkes: Department of Child Health Rsu MataramDocument48 pagesDr. Sak Indriyani, Spa, Mkes: Department of Child Health Rsu MataramMuhammad Bilal Bin AmirNo ratings yet
- AsmaDocument39 pagesAsmaAndi ZultasyriqNo ratings yet
- Concept Map DraftsDocument9 pagesConcept Map DraftsFc CrisostomoNo ratings yet
- Family Medicine Case FilesDocument44 pagesFamily Medicine Case FilesTazan VoNo ratings yet
- Dr. Ediyono SP P Sub Dep Paru RSAL DR Ramelan: UHT September 2012Document50 pagesDr. Ediyono SP P Sub Dep Paru RSAL DR Ramelan: UHT September 2012gabyNo ratings yet
- Respiratory EmergenciesDocument34 pagesRespiratory EmergenciesRoshana MallawaarachchiNo ratings yet
- Presentado A:: Maria Carolina Aristizabal GomezDocument8 pagesPresentado A:: Maria Carolina Aristizabal GomezSami ArcosNo ratings yet
- Asthma in Children CMEDocument37 pagesAsthma in Children CMEGideon K. MutaiNo ratings yet
- Asthma in Children: April 2014Document35 pagesAsthma in Children: April 2014abdisalaan hassanNo ratings yet
- Class 8 (09.08.2022)Document75 pagesClass 8 (09.08.2022)Ãqûã FîggâNo ratings yet
- Asthma Diagnosis and Treatment GuidelineDocument20 pagesAsthma Diagnosis and Treatment GuidelineaanNo ratings yet
- БронхиальнаяDocument51 pagesБронхиальнаяDaniel FunkNo ratings yet
- Bronchial Asthma VERDEDocument83 pagesBronchial Asthma VERDEVanessa YunqueNo ratings yet
- Allergic RhinitisDocument20 pagesAllergic RhinitisAmit RainaNo ratings yet
- Faegh Aderangi Tarek HassounaDocument68 pagesFaegh Aderangi Tarek HassounasgolbariNo ratings yet
- Etiology & Triggers: AsthmaDocument6 pagesEtiology & Triggers: AsthmaNichole CollinsNo ratings yet
- Allergic RhinitisDocument55 pagesAllergic RhinitisZZNo ratings yet
- Asthma: Prepared By: DR - Habab AbdelrhmanDocument43 pagesAsthma: Prepared By: DR - Habab AbdelrhmanJdjshsbNo ratings yet
- Asthma: Dr. Bayu Sukresno, Sp. PDDocument15 pagesAsthma: Dr. Bayu Sukresno, Sp. PDAi Niech InoelNo ratings yet
- Asma Bronkiale: Muhsin Ppds Ilmu Penyakit Dalam FK Unsyiah Pembimbing: Dr. T. Mamfaluti, M.Kes, SP - PD, FinasimDocument33 pagesAsma Bronkiale: Muhsin Ppds Ilmu Penyakit Dalam FK Unsyiah Pembimbing: Dr. T. Mamfaluti, M.Kes, SP - PD, FinasimEvy LiesniawatiNo ratings yet
- Status Asthmaticus: Triwahju AstutiDocument41 pagesStatus Asthmaticus: Triwahju AstutirianiNo ratings yet
- Asthma ZENDocument57 pagesAsthma ZENKonjit MitikuNo ratings yet
- G IN A: Lobal Itiative For SthmaDocument55 pagesG IN A: Lobal Itiative For Sthmasamah sahakNo ratings yet
- Pediatric Respiratory DiseaseDocument90 pagesPediatric Respiratory DiseasePrashant MishraNo ratings yet
- Definition:: AsthmaDocument7 pagesDefinition:: AsthmaMIchele LeongNo ratings yet
- A Simple Guide to Dysphonia, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Dysphonia, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Exam Questions 4 CourseDocument4 pagesExam Questions 4 CourseVishva Lalitbhai HirparaNo ratings yet
- Neuro Oral AnswerDocument113 pagesNeuro Oral AnswerVishva Lalitbhai HirparaNo ratings yet
- JC Severe Scrub TyphusDocument27 pagesJC Severe Scrub TyphusAakarsh RastogiNo ratings yet
- Activity 6: Diagnostic Test and Procedures For Gastrointestinal SystemDocument29 pagesActivity 6: Diagnostic Test and Procedures For Gastrointestinal SystemRalp ManglicmotNo ratings yet
- Hyperkalemia - ICUDocument1 pageHyperkalemia - ICURithNo ratings yet
- Depression: Dr. John BergmanDocument54 pagesDepression: Dr. John Bergmanzeina32No ratings yet
- Terapi ToxoplasmosisDocument9 pagesTerapi Toxoplasmosissarah disaNo ratings yet
- Unit 11. Advocacy Programs Relevant To The Care of OlderDocument13 pagesUnit 11. Advocacy Programs Relevant To The Care of OlderRichmon Joseph SantosNo ratings yet
- Cold Chain System and Adverse Reaction Following Immunization (Aefi)Document46 pagesCold Chain System and Adverse Reaction Following Immunization (Aefi)Shikya AbnasNo ratings yet
- Blood Pressure in Early Autosomal Dominant Polycystic Kidney DiseaseDocument5 pagesBlood Pressure in Early Autosomal Dominant Polycystic Kidney DiseaseNancy MolinaNo ratings yet
- Blood CoagulationDocument8 pagesBlood CoagulationJaslir MendozaNo ratings yet
- Davao Doctors College Nursing Program Nursing Care PlanDocument6 pagesDavao Doctors College Nursing Program Nursing Care PlanSHINI0% (1)
- Enoxaparin - Prescribing, Administration and MonitoringDocument6 pagesEnoxaparin - Prescribing, Administration and MonitoringFaheem AlsabriaNo ratings yet
- Head GearDocument16 pagesHead GearHareemNo ratings yet
- Palatal Fistula: Dr. Amru Sungkar, SPB-SPBPDocument48 pagesPalatal Fistula: Dr. Amru Sungkar, SPB-SPBPlukhoriNo ratings yet
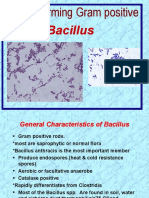
- Bacillus: Spore-Forming Gram PositiveDocument24 pagesBacillus: Spore-Forming Gram Positiveعلي عبد الكريم عاصيNo ratings yet
- Article Review ContohDocument15 pagesArticle Review ContohRadhi ShukriNo ratings yet
- Wongs Essentials of Pediatric Nursing 9th Edition Hockenberry Test BankDocument4 pagesWongs Essentials of Pediatric Nursing 9th Edition Hockenberry Test BankPeter Strange100% (30)
- Cphi Drug ListDocument11 pagesCphi Drug ListSanjay NavaleNo ratings yet
- Respiratory Disorder in PregnancyDocument52 pagesRespiratory Disorder in Pregnancyjhon heriansyahNo ratings yet
- Beta-Lactam Antibiotics & Other Cell Wall Synthesis InhibitorsDocument29 pagesBeta-Lactam Antibiotics & Other Cell Wall Synthesis InhibitorsRen PastelNo ratings yet
- Ignatavicius: Medical-Surgical Nursing, 9th EditionDocument5 pagesIgnatavicius: Medical-Surgical Nursing, 9th Editionfunky goodNo ratings yet
- Peripheral Neuropathy Clinical ApproachDocument19 pagesPeripheral Neuropathy Clinical ApproachNur Nadzifah Zainal AbidinNo ratings yet
- Gen Med Revision PDF 5Document107 pagesGen Med Revision PDF 5sharen100% (3)
- CH 21Document19 pagesCH 21Lisa Evitt CoxNo ratings yet
- Breast Cancer Content Concepts Map For Case Study1Document3 pagesBreast Cancer Content Concepts Map For Case Study1akankshaNo ratings yet
- Infanrix-Hexa SMPC 09 2020Document15 pagesInfanrix-Hexa SMPC 09 2020walkrogNo ratings yet