Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- 551.2r 15 Design Guide For Tilt Up Concrete PanelsDocument76 pages551.2r 15 Design Guide For Tilt Up Concrete PanelsKvrd PrasadNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- A Materialist Theory of The Mind by D. M. ArmstrongDocument8 pagesA Materialist Theory of The Mind by D. M. ArmstrongDon ArthurNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Euthenics PTDocument2 pagesEuthenics PTMwen Pelostratos100% (1)
- Reflection PaperDocument6 pagesReflection PapermarkNo ratings yet
- A2 Sitxwhs001 Activity Part1 Ver October 2019Document12 pagesA2 Sitxwhs001 Activity Part1 Ver October 2019jyoti singhNo ratings yet
- SECTION 1: Identification of The Substance/mixture and of The Company/undertakingDocument7 pagesSECTION 1: Identification of The Substance/mixture and of The Company/undertakingNaishal PatelNo ratings yet
- Health Policy: Alex Jingwei He, Vivien F.Y. TangDocument12 pagesHealth Policy: Alex Jingwei He, Vivien F.Y. TangNurul pattyNo ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument13 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsNurul pattyNo ratings yet
- En V12n1a05Document7 pagesEn V12n1a05Nurul pattyNo ratings yet
- A Health Policy and Systems Research Reader On: Human Resources For HealthDocument14 pagesA Health Policy and Systems Research Reader On: Human Resources For HealthNurul pattyNo ratings yet
- Hope Is An Optimistic State of Mind That Is Based On An Expectation of Positive Outcomes With Respect To EventsDocument10 pagesHope Is An Optimistic State of Mind That Is Based On An Expectation of Positive Outcomes With Respect To EventsNurul pattyNo ratings yet
- 13190-Article Text-25193-1-10-20201127Document5 pages13190-Article Text-25193-1-10-20201127Nurul pattyNo ratings yet
- Hope Life Satisfaction and MotivationDocument19 pagesHope Life Satisfaction and MotivationNurul pattyNo ratings yet
- Gerontology in India: International SpotlightDocument7 pagesGerontology in India: International SpotlightNurul pattyNo ratings yet
- FactSheet SeniorCentersDocument2 pagesFactSheet SeniorCentersNurul pattyNo ratings yet
- 1989 VallerandOConnor CPDocument13 pages1989 VallerandOConnor CPNurul pattyNo ratings yet
- Cki 116Document7 pagesCki 116Nurul pattyNo ratings yet
- Community Health Workers Caring For Dependent Elderly PeopleDocument10 pagesCommunity Health Workers Caring For Dependent Elderly PeopleNurul pattyNo ratings yet
- Sources of Community Health Worker Motivation: A Qualitative Study in Morogoro Region, TanzaniaDocument12 pagesSources of Community Health Worker Motivation: A Qualitative Study in Morogoro Region, TanzaniaNurul pattyNo ratings yet
- 15 Expectations Satisfaction ElderlyDocument7 pages15 Expectations Satisfaction ElderlyNurul pattyNo ratings yet
- 33 Pages 163 177Document15 pages33 Pages 163 177Nurul pattyNo ratings yet
- Critical Thinking Clinical Judgment and Nursing Process - Nurse KeyDocument21 pagesCritical Thinking Clinical Judgment and Nursing Process - Nurse KeyNurul pattyNo ratings yet
- The ECHI Project: Health Indicators For The European CommunityDocument6 pagesThe ECHI Project: Health Indicators For The European CommunityNurul pattyNo ratings yet
- Ethnicity & Health: To Cite This Article: KRISTIINA HEIKKILÄ & SIRKKA-LIISA EKMAN (2003) Elderly Care For EthnicDocument13 pagesEthnicity & Health: To Cite This Article: KRISTIINA HEIKKILÄ & SIRKKA-LIISA EKMAN (2003) Elderly Care For EthnicNurul pattyNo ratings yet
- A C R C C D D L A: Utomated Ardiothoracic Atio Alculation and Ardiomegaly Etection Using EEP Earning PproachDocument11 pagesA C R C C D D L A: Utomated Ardiothoracic Atio Alculation and Ardiomegaly Etection Using EEP Earning PproachNurul pattyNo ratings yet
- Patients' Knowledge of Diabetes Complications and S Elf-Management Practices in GhanaDocument18 pagesPatients' Knowledge of Diabetes Complications and S Elf-Management Practices in GhanaNurul pattyNo ratings yet
- Jurnal Covid VDocument4 pagesJurnal Covid VNurul pattyNo ratings yet
- Role of Patient Coping Strategies in Understanding The Effects of Early Palliative Care On Quality of Life and MoodDocument11 pagesRole of Patient Coping Strategies in Understanding The Effects of Early Palliative Care On Quality of Life and MoodNurul pattyNo ratings yet
- 14 - Rini Rachmawaty - Jurnalmankep - Coben-2008Document6 pages14 - Rini Rachmawaty - Jurnalmankep - Coben-2008Nurul pattyNo ratings yet
- The Correlation Between Happiness and Self-Transcendence in The Elderly of Khoshkrud, Zarandieh CityDocument16 pagesThe Correlation Between Happiness and Self-Transcendence in The Elderly of Khoshkrud, Zarandieh CityNurul pattyNo ratings yet
- MILLER, Nursing For Wellness in Older Adult - P61Document2 pagesMILLER, Nursing For Wellness in Older Adult - P61Nurul pattyNo ratings yet
- ESE ESNAT 2016 Adrenal IncidentalomaDocument34 pagesESE ESNAT 2016 Adrenal Incidentalomalim_kai_weiNo ratings yet
- Delirium, Dementia, PsychosisDocument1 pageDelirium, Dementia, PsychosisLana LocoNo ratings yet
- Edition 2 1Document3 pagesEdition 2 1api-549746046No ratings yet
- Central Council For: in HomoeopathyDocument18 pagesCentral Council For: in Homoeopathy9891233665No ratings yet
- Knowledge, Attitude, and Practice of Mothers On The First 1000 Days of LifeDocument8 pagesKnowledge, Attitude, and Practice of Mothers On The First 1000 Days of LifeSarah Ong SiuNo ratings yet
- Personalized Medicine - A Biological Approach To Patient Treatment - FDADocument5 pagesPersonalized Medicine - A Biological Approach To Patient Treatment - FDAAditya DebnathNo ratings yet
- Ipt-Ast Fact Sheet Interpersonal Therapy For AdolescentsDocument2 pagesIpt-Ast Fact Sheet Interpersonal Therapy For Adolescentsapi-507192289No ratings yet
- Periodontology Lec 2Document24 pagesPeriodontology Lec 2Ali MONo ratings yet
- Submaximal Fitness Tests in Team SportsDocument22 pagesSubmaximal Fitness Tests in Team SportsRoberto Portillo GarcíaNo ratings yet
- Answer All Questions. Each Questions Is Followed by Four Options, A, B, C, and D. For Each Question, Choose One Answer OnlyDocument4 pagesAnswer All Questions. Each Questions Is Followed by Four Options, A, B, C, and D. For Each Question, Choose One Answer OnlyFarid HajisNo ratings yet
- Eq and CQ Paragraph FormDocument18 pagesEq and CQ Paragraph FormmichaellanicpaculbzNo ratings yet
- Perceptions of Safety Management and Safety Culture in The Aviation Industry in New Zealand PDFDocument7 pagesPerceptions of Safety Management and Safety Culture in The Aviation Industry in New Zealand PDFrana abdulwasayNo ratings yet
- Appendix 5 Lean Six Sigma Interview Questionnaire For HospitalsDocument4 pagesAppendix 5 Lean Six Sigma Interview Questionnaire For HospitalsShibu SamuelNo ratings yet
- Test Questionnaires With Key Answer - Gabriel Aand BobisDocument6 pagesTest Questionnaires With Key Answer - Gabriel Aand BobisLeah BobisNo ratings yet
- New Flow Pasien Igd 11 November 2023 RinaDocument7 pagesNew Flow Pasien Igd 11 November 2023 RinasayaseorangdokterNo ratings yet
- Antenatal Care and Its Effect On Risk of PihDocument11 pagesAntenatal Care and Its Effect On Risk of PihNoraNo ratings yet
- Career Paths - Mediator (INFP) Personality - 16personalities Part06Document3 pagesCareer Paths - Mediator (INFP) Personality - 16personalities Part06CATIA VALERIA FERRAGENS E SELANTESNo ratings yet
- Hypertension in Hemodialysis PatientDocument54 pagesHypertension in Hemodialysis PatientIchtiar MahesaNo ratings yet
- Men S Fitness Uk October 2021Document100 pagesMen S Fitness Uk October 2021Ator DelNo ratings yet
- Lyle Mcdonald Womens BookDocument2 pagesLyle Mcdonald Womens BookAbdullah ZaidNo ratings yet
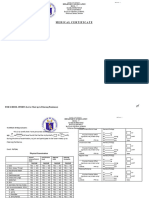
- Medical Certificate MC Form 1 All Sports EventsDocument2 pagesMedical Certificate MC Form 1 All Sports EventsKriston CabilesNo ratings yet
- Postnatal Care PlanDocument20 pagesPostnatal Care Planjinsi georgeNo ratings yet
- Common Induction Moot, 2019 Law Centre-Ii: ROLL NO. 188097Document24 pagesCommon Induction Moot, 2019 Law Centre-Ii: ROLL NO. 188097Nikita GuptaNo ratings yet
- Case Study For Round 1 of HCCB Case Challenge Season 1Document4 pagesCase Study For Round 1 of HCCB Case Challenge Season 1NitikaNo ratings yet