
Diagnosis and Treatment Planning Part 1
Diagnosis and Treatment Planning Part 1
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5835)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (350)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Washington State CNA Skills BookletDocument60 pagesWashington State CNA Skills BookletJames Pallant100% (1)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
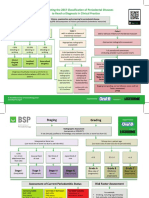
- BSP FlowchartDocument2 pagesBSP FlowchartShahrukh ali khan100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Evaluationand Comparisonofthe Effectof Different Border Molding Materialson 0 AComplete Denture Retention Aniinvivoi StudyDocument7 pagesEvaluationand Comparisonofthe Effectof Different Border Molding Materialson 0 AComplete Denture Retention Aniinvivoi StudyShahrukh ali khanNo ratings yet
- Comparison of Complete Denture Fabricated by Two Different Border Molding Materials, in Terms of Patients' SatisfactionDocument4 pagesComparison of Complete Denture Fabricated by Two Different Border Molding Materials, in Terms of Patients' SatisfactionShahrukh ali khanNo ratings yet
- Complete Denture IntroductionDocument3 pagesComplete Denture IntroductionShahrukh ali khanNo ratings yet
- Staging and GradingDocument4 pagesStaging and GradingShahrukh ali khanNo ratings yet
- Diagnosis and Treatment Planning Part 1Document12 pagesDiagnosis and Treatment Planning Part 1Shahrukh ali khanNo ratings yet
- Effects of Ageing On Edentulous Mouth: BoneDocument6 pagesEffects of Ageing On Edentulous Mouth: BoneShahrukh ali khanNo ratings yet
- Dental Bleaching: Presenter: DR Shahrukh Ali Khan Resident R1 Prosthodontics Aga Khan University, HospitalDocument47 pagesDental Bleaching: Presenter: DR Shahrukh Ali Khan Resident R1 Prosthodontics Aga Khan University, HospitalShahrukh ali khanNo ratings yet
- Research ArticleDocument7 pagesResearch ArticleShahrukh ali khanNo ratings yet
- Clinics in SurgeryDocument5 pagesClinics in SurgeryShahrukh ali khanNo ratings yet
- Common Mistakes in Clinical ResearchDocument6 pagesCommon Mistakes in Clinical ResearchShahrukh ali khanNo ratings yet
- FDS Amp 2020Document140 pagesFDS Amp 2020Shahrukh ali khan100% (1)
- Evaluation of Signs, Symptoms, and Occlusal Factors Among Patients With Temporomandibular Disorders According To Helkimo IndexDocument8 pagesEvaluation of Signs, Symptoms, and Occlusal Factors Among Patients With Temporomandibular Disorders According To Helkimo IndexShahrukh ali khanNo ratings yet
- Bloodborne Pathogens Learner Course Guide: Florida Department of HealthDocument30 pagesBloodborne Pathogens Learner Course Guide: Florida Department of HealthShahrukh ali khanNo ratings yet
- Infection Control in DentistryDocument69 pagesInfection Control in DentistryShahrukh ali khanNo ratings yet
- CeramicsDocument93 pagesCeramicsMooly ZakiNo ratings yet
- Long Span Ridge With Precision AttachmentDocument6 pagesLong Span Ridge With Precision AttachmentSHAILJA KATIYARNo ratings yet
- DR - Firas Mahmoud Abu Samra: Curriculum Vitae ofDocument16 pagesDR - Firas Mahmoud Abu Samra: Curriculum Vitae offerasallanNo ratings yet
- A Hollow Bulb ObturatorDocument6 pagesA Hollow Bulb ObturatorrekabiNo ratings yet
- Review Article: Occlusal Schemes For Complete Dentures - A Review ArticleDocument6 pagesReview Article: Occlusal Schemes For Complete Dentures - A Review ArticleoktikikiNo ratings yet
- Occlusion in Edentulous PatientDocument87 pagesOcclusion in Edentulous PatientMithun UpadhyaNo ratings yet
- Single Denture - II-Combination SyndromeDocument30 pagesSingle Denture - II-Combination SyndromeIsmail HamadaNo ratings yet
- RX Dentist BiotempsDocument2 pagesRX Dentist BiotempsdamingeniusNo ratings yet
- Prostho 3 Anatomic LandmarkDocument3 pagesProstho 3 Anatomic LandmarkLeigh Belmonte67% (3)
- New Questions 1Document2 pagesNew Questions 1ShobhitNo ratings yet
- PowerpointDocument33 pagesPowerpointZain HashmiNo ratings yet
- Prometric 2015 DR - Kadeeb Vol1.0. Jan2015 SolvedDocument54 pagesPrometric 2015 DR - Kadeeb Vol1.0. Jan2015 SolvedSubhajit Saha0% (1)
- Pre-Extraction Records in Edentulous Patients - A Literature ReviewDocument6 pagesPre-Extraction Records in Edentulous Patients - A Literature ReviewMaywiNo ratings yet
- Management of Flabby Ridge Case Report.20150524060252Document7 pagesManagement of Flabby Ridge Case Report.20150524060252Rico AnasNo ratings yet
- Prosthetics in DentistryDocument1 pageProsthetics in DentistryAmar BhochhibhoyaNo ratings yet
- Kaldenbach Carina Articol EPI Engleza PDFDocument9 pagesKaldenbach Carina Articol EPI Engleza PDFFlorin UngureanuNo ratings yet
- Implant Consent Form1Document2 pagesImplant Consent Form1Jitender ReddyNo ratings yet
- Managing The Unstable CDDocument8 pagesManaging The Unstable CDNajeeb UllahNo ratings yet
- Destiny and DevilDocument177 pagesDestiny and DevilSrinivasan NarasimhanNo ratings yet
- Form WHO Dewasa PDFDocument2 pagesForm WHO Dewasa PDFAbizar Agung WibawaNo ratings yet
- Procedure ListDocument20 pagesProcedure ListsoyrolandoNo ratings yet
- Gothic Arch Tracing PDFDocument5 pagesGothic Arch Tracing PDFSimran SahniNo ratings yet
- Requirements of A Direct RetainerDocument10 pagesRequirements of A Direct RetainerAnnika Siti ResdyantiNo ratings yet
- Asian Green Mussel Shells Perna Veridis As Base Ingredient and Strengthener For Partial DenturesDocument25 pagesAsian Green Mussel Shells Perna Veridis As Base Ingredient and Strengthener For Partial DenturesashleyNo ratings yet
- 2 - Diagnosis and Treatment PlanningDocument55 pages2 - Diagnosis and Treatment Planningamoon almNo ratings yet
- Residual Ridge Resorption Seminar PART 2Document144 pagesResidual Ridge Resorption Seminar PART 2ksowmyasreeNo ratings yet
- Book Reviews: Fundamentals For Maxillofacial ProstheticsDocument2 pagesBook Reviews: Fundamentals For Maxillofacial ProstheticsIbrahim SahibzadaNo ratings yet
- JShotwell Week6Document50 pagesJShotwell Week6Priyanka GandhiNo ratings yet
- Alzheimers Disease and Dental ManagementDocument5 pagesAlzheimers Disease and Dental ManagementMalu OliveiraNo ratings yet



















































































Download as docx, pdf, or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5835)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (350)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Washington State CNA Skills BookletDocument60 pagesWashington State CNA Skills BookletJames Pallant100% (1)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- BSP FlowchartDocument2 pagesBSP FlowchartShahrukh ali khan100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Evaluationand Comparisonofthe Effectof Different Border Molding Materialson 0 AComplete Denture Retention Aniinvivoi StudyDocument7 pagesEvaluationand Comparisonofthe Effectof Different Border Molding Materialson 0 AComplete Denture Retention Aniinvivoi StudyShahrukh ali khanNo ratings yet
- Comparison of Complete Denture Fabricated by Two Different Border Molding Materials, in Terms of Patients' SatisfactionDocument4 pagesComparison of Complete Denture Fabricated by Two Different Border Molding Materials, in Terms of Patients' SatisfactionShahrukh ali khanNo ratings yet
- Complete Denture IntroductionDocument3 pagesComplete Denture IntroductionShahrukh ali khanNo ratings yet
- Staging and GradingDocument4 pagesStaging and GradingShahrukh ali khanNo ratings yet
- Diagnosis and Treatment Planning Part 1Document12 pagesDiagnosis and Treatment Planning Part 1Shahrukh ali khanNo ratings yet
- Effects of Ageing On Edentulous Mouth: BoneDocument6 pagesEffects of Ageing On Edentulous Mouth: BoneShahrukh ali khanNo ratings yet
- Dental Bleaching: Presenter: DR Shahrukh Ali Khan Resident R1 Prosthodontics Aga Khan University, HospitalDocument47 pagesDental Bleaching: Presenter: DR Shahrukh Ali Khan Resident R1 Prosthodontics Aga Khan University, HospitalShahrukh ali khanNo ratings yet
- Research ArticleDocument7 pagesResearch ArticleShahrukh ali khanNo ratings yet
- Clinics in SurgeryDocument5 pagesClinics in SurgeryShahrukh ali khanNo ratings yet
- Common Mistakes in Clinical ResearchDocument6 pagesCommon Mistakes in Clinical ResearchShahrukh ali khanNo ratings yet
- FDS Amp 2020Document140 pagesFDS Amp 2020Shahrukh ali khan100% (1)
- Evaluation of Signs, Symptoms, and Occlusal Factors Among Patients With Temporomandibular Disorders According To Helkimo IndexDocument8 pagesEvaluation of Signs, Symptoms, and Occlusal Factors Among Patients With Temporomandibular Disorders According To Helkimo IndexShahrukh ali khanNo ratings yet
- Bloodborne Pathogens Learner Course Guide: Florida Department of HealthDocument30 pagesBloodborne Pathogens Learner Course Guide: Florida Department of HealthShahrukh ali khanNo ratings yet
- Infection Control in DentistryDocument69 pagesInfection Control in DentistryShahrukh ali khanNo ratings yet
- CeramicsDocument93 pagesCeramicsMooly ZakiNo ratings yet
- Long Span Ridge With Precision AttachmentDocument6 pagesLong Span Ridge With Precision AttachmentSHAILJA KATIYARNo ratings yet
- DR - Firas Mahmoud Abu Samra: Curriculum Vitae ofDocument16 pagesDR - Firas Mahmoud Abu Samra: Curriculum Vitae offerasallanNo ratings yet
- A Hollow Bulb ObturatorDocument6 pagesA Hollow Bulb ObturatorrekabiNo ratings yet
- Review Article: Occlusal Schemes For Complete Dentures - A Review ArticleDocument6 pagesReview Article: Occlusal Schemes For Complete Dentures - A Review ArticleoktikikiNo ratings yet
- Occlusion in Edentulous PatientDocument87 pagesOcclusion in Edentulous PatientMithun UpadhyaNo ratings yet
- Single Denture - II-Combination SyndromeDocument30 pagesSingle Denture - II-Combination SyndromeIsmail HamadaNo ratings yet
- RX Dentist BiotempsDocument2 pagesRX Dentist BiotempsdamingeniusNo ratings yet
- Prostho 3 Anatomic LandmarkDocument3 pagesProstho 3 Anatomic LandmarkLeigh Belmonte67% (3)
- New Questions 1Document2 pagesNew Questions 1ShobhitNo ratings yet
- PowerpointDocument33 pagesPowerpointZain HashmiNo ratings yet
- Prometric 2015 DR - Kadeeb Vol1.0. Jan2015 SolvedDocument54 pagesPrometric 2015 DR - Kadeeb Vol1.0. Jan2015 SolvedSubhajit Saha0% (1)
- Pre-Extraction Records in Edentulous Patients - A Literature ReviewDocument6 pagesPre-Extraction Records in Edentulous Patients - A Literature ReviewMaywiNo ratings yet
- Management of Flabby Ridge Case Report.20150524060252Document7 pagesManagement of Flabby Ridge Case Report.20150524060252Rico AnasNo ratings yet
- Prosthetics in DentistryDocument1 pageProsthetics in DentistryAmar BhochhibhoyaNo ratings yet
- Kaldenbach Carina Articol EPI Engleza PDFDocument9 pagesKaldenbach Carina Articol EPI Engleza PDFFlorin UngureanuNo ratings yet
- Implant Consent Form1Document2 pagesImplant Consent Form1Jitender ReddyNo ratings yet
- Managing The Unstable CDDocument8 pagesManaging The Unstable CDNajeeb UllahNo ratings yet
- Destiny and DevilDocument177 pagesDestiny and DevilSrinivasan NarasimhanNo ratings yet
- Form WHO Dewasa PDFDocument2 pagesForm WHO Dewasa PDFAbizar Agung WibawaNo ratings yet
- Procedure ListDocument20 pagesProcedure ListsoyrolandoNo ratings yet
- Gothic Arch Tracing PDFDocument5 pagesGothic Arch Tracing PDFSimran SahniNo ratings yet
- Requirements of A Direct RetainerDocument10 pagesRequirements of A Direct RetainerAnnika Siti ResdyantiNo ratings yet
- Asian Green Mussel Shells Perna Veridis As Base Ingredient and Strengthener For Partial DenturesDocument25 pagesAsian Green Mussel Shells Perna Veridis As Base Ingredient and Strengthener For Partial DenturesashleyNo ratings yet
- 2 - Diagnosis and Treatment PlanningDocument55 pages2 - Diagnosis and Treatment Planningamoon almNo ratings yet
- Residual Ridge Resorption Seminar PART 2Document144 pagesResidual Ridge Resorption Seminar PART 2ksowmyasreeNo ratings yet
- Book Reviews: Fundamentals For Maxillofacial ProstheticsDocument2 pagesBook Reviews: Fundamentals For Maxillofacial ProstheticsIbrahim SahibzadaNo ratings yet
- JShotwell Week6Document50 pagesJShotwell Week6Priyanka GandhiNo ratings yet
- Alzheimers Disease and Dental ManagementDocument5 pagesAlzheimers Disease and Dental ManagementMalu OliveiraNo ratings yet