
COVID-19 Vaccination Consent Form: Adults
COVID-19 Vaccination Consent Form: Adults
You might also like
- NCP. Decreased Cardiac OutputDocument5 pagesNCP. Decreased Cardiac OutputJillian AmponinNo ratings yet
- House Calls 101: The Complete Clinician's Guide To In-Home Health Care, Telemedicine Services, and Long-Distance Treatment For a Post-Pandemic WorldFrom EverandHouse Calls 101: The Complete Clinician's Guide To In-Home Health Care, Telemedicine Services, and Long-Distance Treatment For a Post-Pandemic WorldNo ratings yet
- COVID Immunization Record Correction RequestDocument1 pageCOVID Immunization Record Correction RequestNBC 10 WJAR50% (2)
- Your Covid-19 Survival Manual: A Physician's Guide to Keep You and Your Family Healthy During the Pandemic and BeyondFrom EverandYour Covid-19 Survival Manual: A Physician's Guide to Keep You and Your Family Healthy During the Pandemic and BeyondNo ratings yet
- PHE 11920 Covid-19 Consent Form Frontline SCSDocument1 pagePHE 11920 Covid-19 Consent Form Frontline SCSCormac QuinnNo ratings yet
- Imm102 Covid19 Pfizer New Consent Form 18121Document2 pagesImm102 Covid19 Pfizer New Consent Form 18121micleanNo ratings yet
- UKHSA COVID 19 Consent Form CYPDocument1 pageUKHSA COVID 19 Consent Form CYPPaula BurogNo ratings yet
- Personal Data of The Person To Be Vaccinated - COVID-19 mRNA VaccinesDocument2 pagesPersonal Data of The Person To Be Vaccinated - COVID-19 mRNA VaccinessdfasdweNo ratings yet
- COVID Safe PlanDocument9 pagesCOVID Safe PlanskubalaspamNo ratings yet
- COVID-19 Vax Consent FormDocument3 pagesCOVID-19 Vax Consent FormCj CCNo ratings yet
- Covid-19 Vaccine Screening and Consent Form Pfizer-Biontech Covid-19 VaccineDocument2 pagesCovid-19 Vaccine Screening and Consent Form Pfizer-Biontech Covid-19 Vaccinesiriamma wiliamsNo ratings yet
- Formular Za Pristanak Na Cijepljenje Na FloridiDocument2 pagesFormular Za Pristanak Na Cijepljenje Na FloridiIndex.hrNo ratings yet
- COVID-19 Vaccination Pre-Registration Form - 1 Dose: 1. BiodataDocument2 pagesCOVID-19 Vaccination Pre-Registration Form - 1 Dose: 1. BiodataMaimoon AliNo ratings yet
- Declaration of Good Health Form - With Covid QDocument2 pagesDeclaration of Good Health Form - With Covid QRajnish YadavNo ratings yet
- Medical Application Form PDFDocument3 pagesMedical Application Form PDFHumanNo ratings yet
- FINAL COVID-19 Vaccine Consent Form Inc. FDA Eua and ACIP 12.13.2020Document2 pagesFINAL COVID-19 Vaccine Consent Form Inc. FDA Eua and ACIP 12.13.2020Natasa PrelevicNo ratings yet
- OutptInfoConsenttoTreat-NH_900133Document1 pageOutptInfoConsenttoTreat-NH_900133brooklynlowe24No ratings yet
- BivalentConsent MichaelBelen HAG322426Document2 pagesBivalentConsent MichaelBelen HAG322426michaeljohnbelen14No ratings yet
- Fillable PDA COVID Form and Informed ConsentDocument1 pageFillable PDA COVID Form and Informed ConsentShane Marie ClitarNo ratings yet
- Health Form TDocument7 pagesHealth Form TcannistramoralescsjNo ratings yet
- Consent Form - Pfizer-Biontech Covid-19 VaccineDocument2 pagesConsent Form - Pfizer-Biontech Covid-19 VaccineRommel Bucasas GarciaNo ratings yet
- BivalentConsent LucianaPedrosopessoa 559154Document2 pagesBivalentConsent LucianaPedrosopessoa 559154Tatah SouzaNo ratings yet
- Pfizer Consent Form - FillableDocument8 pagesPfizer Consent Form - FillableAbraham Baeza - Viajes PegüisNo ratings yet
- COVID-19 Self-Declaration Form - Atul ValsadDocument2 pagesCOVID-19 Self-Declaration Form - Atul Valsad8460272421No ratings yet
- Medical Application Form: Insured Name: Inception DateDocument3 pagesMedical Application Form: Insured Name: Inception DateDidier G PeñuelaNo ratings yet
- Family Medical Insurance Application PDFDocument6 pagesFamily Medical Insurance Application PDFScribdTranslationsNo ratings yet
- COVID 19 Consent FormDocument2 pagesCOVID 19 Consent FormfvdssfdNo ratings yet
- Form#1 - HDF - Consent Form For RT-PCRDocument1 pageForm#1 - HDF - Consent Form For RT-PCRdddzbdcmrkNo ratings yet
- Medical QuestionnaireDocument2 pagesMedical QuestionnaireKunal GuptaNo ratings yet
- Case Questionnaire COVID-19 (Novel Coronavirus) - Part A: InformationDocument11 pagesCase Questionnaire COVID-19 (Novel Coronavirus) - Part A: InformationHenrietta CookNo ratings yet
- Moderna Informed Consent Form Eng June 18 2021Document1 pageModerna Informed Consent Form Eng June 18 2021Bruce GonzalesNo ratings yet
- ParcfDocument8 pagesParcfGoogool YNo ratings yet
- Patient Consent Form (Hiv) : Treating Doctor'S DetailsDocument1 pagePatient Consent Form (Hiv) : Treating Doctor'S DetailsValentino KhojaNo ratings yet
- Vaccine Cluster - Health Screening FormDocument3 pagesVaccine Cluster - Health Screening FormArlene AngelesNo ratings yet
- Vaers: Information About The Facility Where Vaccine Was Given Information About The Person Completing This FormDocument4 pagesVaers: Information About The Facility Where Vaccine Was Given Information About The Person Completing This FormGarrick BarberNo ratings yet
- COVID-19 Vaccination Consent Form: Basic Info: First Tell Us Who You AreDocument2 pagesCOVID-19 Vaccination Consent Form: Basic Info: First Tell Us Who You AreVAS skytelNo ratings yet
- National Adverse Events Following Immunisation Aefi Reporting Form Feb 2021Document5 pagesNational Adverse Events Following Immunisation Aefi Reporting Form Feb 2021ernawatilebeNo ratings yet
- (ASTRAZENECA) Informed Consent Form - Eng March 5 2021Document1 page(ASTRAZENECA) Informed Consent Form - Eng March 5 2021Mara Ozoa VillaroyaNo ratings yet
- Informed Consent Form For The Astrazeneca Covid-19 VaccineDocument1 pageInformed Consent Form For The Astrazeneca Covid-19 VaccineJohn BNo ratings yet
- Informed Consent Form For The Astrazeneca Covid-19 VaccineDocument1 pageInformed Consent Form For The Astrazeneca Covid-19 VaccineBelle Alaba - RabiaNo ratings yet
- CONSENT FORM - COVID-19 VaccineDocument5 pagesCONSENT FORM - COVID-19 Vaccinebersabeh abayNo ratings yet
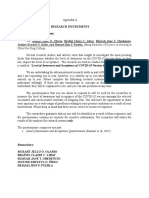
- Research Instruments Dear Sir/Ma'am RespondentDocument4 pagesResearch Instruments Dear Sir/Ma'am RespondentMozart OlarioNo ratings yet
- Informed Consent Form For The Astrazeneca Covid-19 VaccineDocument1 pageInformed Consent Form For The Astrazeneca Covid-19 VaccineGodfrey Loth Sales Alcansare Jr.No ratings yet
- DOH - Covid Vaccine Screening Consent FormDocument2 pagesDOH - Covid Vaccine Screening Consent FormCasey Feindt100% (1)
- Covid19vaccineconsentform UpdatedDocument2 pagesCovid19vaccineconsentform UpdatedGlenn ReinhardtNo ratings yet
- ME In-G Ie: Claim FormDocument4 pagesME In-G Ie: Claim FormnithiananthiNo ratings yet
- BMS Patient Assistance FoundationDocument4 pagesBMS Patient Assistance FoundationJhoanna MonterolaNo ratings yet
- Registration and Consent Form For Covid 19 Vaccination 05.03.21Document4 pagesRegistration and Consent Form For Covid 19 Vaccination 05.03.21Yash HardowarNo ratings yet
- COVID Vaccination Packet SFODocument16 pagesCOVID Vaccination Packet SFOferNo ratings yet
- Medical Report and ReceiptDocument5 pagesMedical Report and Receiptkumarsam087No ratings yet
- Boosters Informed Consent Form ENGDocument1 pageBoosters Informed Consent Form ENGMoi ValdozNo ratings yet
- COVID 19 HEALTH DECLRATION AND LIABILITY WAIVER National Trainers Conference 2024Document2 pagesCOVID 19 HEALTH DECLRATION AND LIABILITY WAIVER National Trainers Conference 2024Randy JabatNo ratings yet
- Affidavit of Vaccine Adverse EffectDocument4 pagesAffidavit of Vaccine Adverse EffectRichard BalaisNo ratings yet
- Consent Form (Sinovac)Document1 pageConsent Form (Sinovac)Kresta BenignoNo ratings yet
- AUS Bupa Global Claim Form EN APR21 0028299Document8 pagesAUS Bupa Global Claim Form EN APR21 0028299ALJABERNo ratings yet
- COVID ConsentDocument3 pagesCOVID Consentakanksha.jain22No ratings yet
- PNC - A3-1Document5 pagesPNC - A3-1dabashgetNo ratings yet
- DIY How to Make Your Own Face Mask Anti Coronavirus. How to Make Your Own Desinfecting GelFrom EverandDIY How to Make Your Own Face Mask Anti Coronavirus. How to Make Your Own Desinfecting GelNo ratings yet
- Acute Raptured Appendicitis - VMCDocument6 pagesAcute Raptured Appendicitis - VMCMicahMananguitNo ratings yet
- Memo - COVID 19 Guidelines and Observance of Safety ProtocolsDocument1 pageMemo - COVID 19 Guidelines and Observance of Safety ProtocolsHav CatsNo ratings yet
- Ishii2020 Article CongenitalMultipleColonicAtresDocument5 pagesIshii2020 Article CongenitalMultipleColonicAtresAnisa GayatriNo ratings yet
- Nystagmus: Dr. Enny Lestari, M. Biomed, SP.SDocument39 pagesNystagmus: Dr. Enny Lestari, M. Biomed, SP.SPuji Yunisyah100% (1)
- Madison - Barfield MaximumHeartRate 04Document1 pageMadison - Barfield MaximumHeartRate 04maemaebarfieldNo ratings yet
- HEMMORRHOIDECTOMYDocument16 pagesHEMMORRHOIDECTOMYLily CentenoNo ratings yet
- Kinesiology Taping Redefined (PDFDrive)Document172 pagesKinesiology Taping Redefined (PDFDrive)Pahonțu Oana - ElenaNo ratings yet
- Discus Prolaps (HNP)Document22 pagesDiscus Prolaps (HNP)Fitriyani Rahma IINo ratings yet
- Learners' Activity Sheets: Health 8Document10 pagesLearners' Activity Sheets: Health 8Leode Joy TulangNo ratings yet
- (Week 10) Epidemiology and Disease TransmissionDocument1 page(Week 10) Epidemiology and Disease TransmissionDiana Leen Dela CruzNo ratings yet
- Drug StudyDocument14 pagesDrug StudyjackSNMMCNo ratings yet
- Question Paper 2023 AIAPGETDocument20 pagesQuestion Paper 2023 AIAPGETrohinibrajole123No ratings yet
- Hannah SchizopreniaDocument5 pagesHannah SchizopreniaEliezah RodriguezNo ratings yet
- Acute PancreatitisDocument2 pagesAcute PancreatitisPrincess Aliha M. JIMENEZNo ratings yet
- NeonatologyDocument47 pagesNeonatologySoumya K SNo ratings yet
- Emergency First Aid Orientation Creating A Plan ISU Youth ProgramsDocument34 pagesEmergency First Aid Orientation Creating A Plan ISU Youth ProgramsKaloy KamaoNo ratings yet
- Acute Otitis Media in AdultsDocument15 pagesAcute Otitis Media in AdultschristineNo ratings yet
- Post Test NUR 219 17Document3 pagesPost Test NUR 219 17Naomi VirtudazoNo ratings yet
- Ajinomoto 11 Horrible Side EffectsDocument7 pagesAjinomoto 11 Horrible Side EffectsYassir ButtNo ratings yet
- Soppi 2018Document5 pagesSoppi 2018dr_joe23No ratings yet
- Urinarytract Infection: Chief ComplaintDocument5 pagesUrinarytract Infection: Chief Complaintrahaf AlNo ratings yet
- Cancer PDFDocument18 pagesCancer PDFAhmed goldenNo ratings yet
- Acute Vs Chronic Renal FailureDocument7 pagesAcute Vs Chronic Renal FailurePellan Rhey CapuyanNo ratings yet
- PyelonephritisDocument24 pagesPyelonephritisfatihahannisahumairaNo ratings yet
- Radiography Technique - Exposure FactorsDocument36 pagesRadiography Technique - Exposure Factorshanghouse8244No ratings yet
- Presentation On Postpartum ComplicationsDocument24 pagesPresentation On Postpartum ComplicationsBeulah DasariNo ratings yet
- Kode Icd 10 Tersering Di Poliklinik Obstetri Dan Ginekologi - EditDocument5 pagesKode Icd 10 Tersering Di Poliklinik Obstetri Dan Ginekologi - EditNur Rohmah Arsyad100% (1)
- ChildDocument17 pagesChildReyna Glorian HilarioNo ratings yet
- Thyroid SwellingDocument8 pagesThyroid SwellingDn Ezrinah Dn Esham50% (2)























































































Download as docx, pdf, or txt
You might also like
- NCP. Decreased Cardiac OutputDocument5 pagesNCP. Decreased Cardiac OutputJillian AmponinNo ratings yet
- House Calls 101: The Complete Clinician's Guide To In-Home Health Care, Telemedicine Services, and Long-Distance Treatment For a Post-Pandemic WorldFrom EverandHouse Calls 101: The Complete Clinician's Guide To In-Home Health Care, Telemedicine Services, and Long-Distance Treatment For a Post-Pandemic WorldNo ratings yet
- COVID Immunization Record Correction RequestDocument1 pageCOVID Immunization Record Correction RequestNBC 10 WJAR50% (2)
- Your Covid-19 Survival Manual: A Physician's Guide to Keep You and Your Family Healthy During the Pandemic and BeyondFrom EverandYour Covid-19 Survival Manual: A Physician's Guide to Keep You and Your Family Healthy During the Pandemic and BeyondNo ratings yet
- PHE 11920 Covid-19 Consent Form Frontline SCSDocument1 pagePHE 11920 Covid-19 Consent Form Frontline SCSCormac QuinnNo ratings yet
- Imm102 Covid19 Pfizer New Consent Form 18121Document2 pagesImm102 Covid19 Pfizer New Consent Form 18121micleanNo ratings yet
- UKHSA COVID 19 Consent Form CYPDocument1 pageUKHSA COVID 19 Consent Form CYPPaula BurogNo ratings yet
- Personal Data of The Person To Be Vaccinated - COVID-19 mRNA VaccinesDocument2 pagesPersonal Data of The Person To Be Vaccinated - COVID-19 mRNA VaccinessdfasdweNo ratings yet
- COVID Safe PlanDocument9 pagesCOVID Safe PlanskubalaspamNo ratings yet
- COVID-19 Vax Consent FormDocument3 pagesCOVID-19 Vax Consent FormCj CCNo ratings yet
- Covid-19 Vaccine Screening and Consent Form Pfizer-Biontech Covid-19 VaccineDocument2 pagesCovid-19 Vaccine Screening and Consent Form Pfizer-Biontech Covid-19 Vaccinesiriamma wiliamsNo ratings yet
- Formular Za Pristanak Na Cijepljenje Na FloridiDocument2 pagesFormular Za Pristanak Na Cijepljenje Na FloridiIndex.hrNo ratings yet
- COVID-19 Vaccination Pre-Registration Form - 1 Dose: 1. BiodataDocument2 pagesCOVID-19 Vaccination Pre-Registration Form - 1 Dose: 1. BiodataMaimoon AliNo ratings yet
- Declaration of Good Health Form - With Covid QDocument2 pagesDeclaration of Good Health Form - With Covid QRajnish YadavNo ratings yet
- Medical Application Form PDFDocument3 pagesMedical Application Form PDFHumanNo ratings yet
- FINAL COVID-19 Vaccine Consent Form Inc. FDA Eua and ACIP 12.13.2020Document2 pagesFINAL COVID-19 Vaccine Consent Form Inc. FDA Eua and ACIP 12.13.2020Natasa PrelevicNo ratings yet
- OutptInfoConsenttoTreat-NH_900133Document1 pageOutptInfoConsenttoTreat-NH_900133brooklynlowe24No ratings yet
- BivalentConsent MichaelBelen HAG322426Document2 pagesBivalentConsent MichaelBelen HAG322426michaeljohnbelen14No ratings yet
- Fillable PDA COVID Form and Informed ConsentDocument1 pageFillable PDA COVID Form and Informed ConsentShane Marie ClitarNo ratings yet
- Health Form TDocument7 pagesHealth Form TcannistramoralescsjNo ratings yet
- Consent Form - Pfizer-Biontech Covid-19 VaccineDocument2 pagesConsent Form - Pfizer-Biontech Covid-19 VaccineRommel Bucasas GarciaNo ratings yet
- BivalentConsent LucianaPedrosopessoa 559154Document2 pagesBivalentConsent LucianaPedrosopessoa 559154Tatah SouzaNo ratings yet
- Pfizer Consent Form - FillableDocument8 pagesPfizer Consent Form - FillableAbraham Baeza - Viajes PegüisNo ratings yet
- COVID-19 Self-Declaration Form - Atul ValsadDocument2 pagesCOVID-19 Self-Declaration Form - Atul Valsad8460272421No ratings yet
- Medical Application Form: Insured Name: Inception DateDocument3 pagesMedical Application Form: Insured Name: Inception DateDidier G PeñuelaNo ratings yet
- Family Medical Insurance Application PDFDocument6 pagesFamily Medical Insurance Application PDFScribdTranslationsNo ratings yet
- COVID 19 Consent FormDocument2 pagesCOVID 19 Consent FormfvdssfdNo ratings yet
- Form#1 - HDF - Consent Form For RT-PCRDocument1 pageForm#1 - HDF - Consent Form For RT-PCRdddzbdcmrkNo ratings yet
- Medical QuestionnaireDocument2 pagesMedical QuestionnaireKunal GuptaNo ratings yet
- Case Questionnaire COVID-19 (Novel Coronavirus) - Part A: InformationDocument11 pagesCase Questionnaire COVID-19 (Novel Coronavirus) - Part A: InformationHenrietta CookNo ratings yet
- Moderna Informed Consent Form Eng June 18 2021Document1 pageModerna Informed Consent Form Eng June 18 2021Bruce GonzalesNo ratings yet
- ParcfDocument8 pagesParcfGoogool YNo ratings yet
- Patient Consent Form (Hiv) : Treating Doctor'S DetailsDocument1 pagePatient Consent Form (Hiv) : Treating Doctor'S DetailsValentino KhojaNo ratings yet
- Vaccine Cluster - Health Screening FormDocument3 pagesVaccine Cluster - Health Screening FormArlene AngelesNo ratings yet
- Vaers: Information About The Facility Where Vaccine Was Given Information About The Person Completing This FormDocument4 pagesVaers: Information About The Facility Where Vaccine Was Given Information About The Person Completing This FormGarrick BarberNo ratings yet
- COVID-19 Vaccination Consent Form: Basic Info: First Tell Us Who You AreDocument2 pagesCOVID-19 Vaccination Consent Form: Basic Info: First Tell Us Who You AreVAS skytelNo ratings yet
- National Adverse Events Following Immunisation Aefi Reporting Form Feb 2021Document5 pagesNational Adverse Events Following Immunisation Aefi Reporting Form Feb 2021ernawatilebeNo ratings yet
- (ASTRAZENECA) Informed Consent Form - Eng March 5 2021Document1 page(ASTRAZENECA) Informed Consent Form - Eng March 5 2021Mara Ozoa VillaroyaNo ratings yet
- Informed Consent Form For The Astrazeneca Covid-19 VaccineDocument1 pageInformed Consent Form For The Astrazeneca Covid-19 VaccineJohn BNo ratings yet
- Informed Consent Form For The Astrazeneca Covid-19 VaccineDocument1 pageInformed Consent Form For The Astrazeneca Covid-19 VaccineBelle Alaba - RabiaNo ratings yet
- CONSENT FORM - COVID-19 VaccineDocument5 pagesCONSENT FORM - COVID-19 Vaccinebersabeh abayNo ratings yet
- Research Instruments Dear Sir/Ma'am RespondentDocument4 pagesResearch Instruments Dear Sir/Ma'am RespondentMozart OlarioNo ratings yet
- Informed Consent Form For The Astrazeneca Covid-19 VaccineDocument1 pageInformed Consent Form For The Astrazeneca Covid-19 VaccineGodfrey Loth Sales Alcansare Jr.No ratings yet
- DOH - Covid Vaccine Screening Consent FormDocument2 pagesDOH - Covid Vaccine Screening Consent FormCasey Feindt100% (1)
- Covid19vaccineconsentform UpdatedDocument2 pagesCovid19vaccineconsentform UpdatedGlenn ReinhardtNo ratings yet
- ME In-G Ie: Claim FormDocument4 pagesME In-G Ie: Claim FormnithiananthiNo ratings yet
- BMS Patient Assistance FoundationDocument4 pagesBMS Patient Assistance FoundationJhoanna MonterolaNo ratings yet
- Registration and Consent Form For Covid 19 Vaccination 05.03.21Document4 pagesRegistration and Consent Form For Covid 19 Vaccination 05.03.21Yash HardowarNo ratings yet
- COVID Vaccination Packet SFODocument16 pagesCOVID Vaccination Packet SFOferNo ratings yet
- Medical Report and ReceiptDocument5 pagesMedical Report and Receiptkumarsam087No ratings yet
- Boosters Informed Consent Form ENGDocument1 pageBoosters Informed Consent Form ENGMoi ValdozNo ratings yet
- COVID 19 HEALTH DECLRATION AND LIABILITY WAIVER National Trainers Conference 2024Document2 pagesCOVID 19 HEALTH DECLRATION AND LIABILITY WAIVER National Trainers Conference 2024Randy JabatNo ratings yet
- Affidavit of Vaccine Adverse EffectDocument4 pagesAffidavit of Vaccine Adverse EffectRichard BalaisNo ratings yet
- Consent Form (Sinovac)Document1 pageConsent Form (Sinovac)Kresta BenignoNo ratings yet
- AUS Bupa Global Claim Form EN APR21 0028299Document8 pagesAUS Bupa Global Claim Form EN APR21 0028299ALJABERNo ratings yet
- COVID ConsentDocument3 pagesCOVID Consentakanksha.jain22No ratings yet
- PNC - A3-1Document5 pagesPNC - A3-1dabashgetNo ratings yet
- DIY How to Make Your Own Face Mask Anti Coronavirus. How to Make Your Own Desinfecting GelFrom EverandDIY How to Make Your Own Face Mask Anti Coronavirus. How to Make Your Own Desinfecting GelNo ratings yet
- Acute Raptured Appendicitis - VMCDocument6 pagesAcute Raptured Appendicitis - VMCMicahMananguitNo ratings yet
- Memo - COVID 19 Guidelines and Observance of Safety ProtocolsDocument1 pageMemo - COVID 19 Guidelines and Observance of Safety ProtocolsHav CatsNo ratings yet
- Ishii2020 Article CongenitalMultipleColonicAtresDocument5 pagesIshii2020 Article CongenitalMultipleColonicAtresAnisa GayatriNo ratings yet
- Nystagmus: Dr. Enny Lestari, M. Biomed, SP.SDocument39 pagesNystagmus: Dr. Enny Lestari, M. Biomed, SP.SPuji Yunisyah100% (1)
- Madison - Barfield MaximumHeartRate 04Document1 pageMadison - Barfield MaximumHeartRate 04maemaebarfieldNo ratings yet
- HEMMORRHOIDECTOMYDocument16 pagesHEMMORRHOIDECTOMYLily CentenoNo ratings yet
- Kinesiology Taping Redefined (PDFDrive)Document172 pagesKinesiology Taping Redefined (PDFDrive)Pahonțu Oana - ElenaNo ratings yet
- Discus Prolaps (HNP)Document22 pagesDiscus Prolaps (HNP)Fitriyani Rahma IINo ratings yet
- Learners' Activity Sheets: Health 8Document10 pagesLearners' Activity Sheets: Health 8Leode Joy TulangNo ratings yet
- (Week 10) Epidemiology and Disease TransmissionDocument1 page(Week 10) Epidemiology and Disease TransmissionDiana Leen Dela CruzNo ratings yet
- Drug StudyDocument14 pagesDrug StudyjackSNMMCNo ratings yet
- Question Paper 2023 AIAPGETDocument20 pagesQuestion Paper 2023 AIAPGETrohinibrajole123No ratings yet
- Hannah SchizopreniaDocument5 pagesHannah SchizopreniaEliezah RodriguezNo ratings yet
- Acute PancreatitisDocument2 pagesAcute PancreatitisPrincess Aliha M. JIMENEZNo ratings yet
- NeonatologyDocument47 pagesNeonatologySoumya K SNo ratings yet
- Emergency First Aid Orientation Creating A Plan ISU Youth ProgramsDocument34 pagesEmergency First Aid Orientation Creating A Plan ISU Youth ProgramsKaloy KamaoNo ratings yet
- Acute Otitis Media in AdultsDocument15 pagesAcute Otitis Media in AdultschristineNo ratings yet
- Post Test NUR 219 17Document3 pagesPost Test NUR 219 17Naomi VirtudazoNo ratings yet
- Ajinomoto 11 Horrible Side EffectsDocument7 pagesAjinomoto 11 Horrible Side EffectsYassir ButtNo ratings yet
- Soppi 2018Document5 pagesSoppi 2018dr_joe23No ratings yet
- Urinarytract Infection: Chief ComplaintDocument5 pagesUrinarytract Infection: Chief Complaintrahaf AlNo ratings yet
- Cancer PDFDocument18 pagesCancer PDFAhmed goldenNo ratings yet
- Acute Vs Chronic Renal FailureDocument7 pagesAcute Vs Chronic Renal FailurePellan Rhey CapuyanNo ratings yet
- PyelonephritisDocument24 pagesPyelonephritisfatihahannisahumairaNo ratings yet
- Radiography Technique - Exposure FactorsDocument36 pagesRadiography Technique - Exposure Factorshanghouse8244No ratings yet
- Presentation On Postpartum ComplicationsDocument24 pagesPresentation On Postpartum ComplicationsBeulah DasariNo ratings yet
- Kode Icd 10 Tersering Di Poliklinik Obstetri Dan Ginekologi - EditDocument5 pagesKode Icd 10 Tersering Di Poliklinik Obstetri Dan Ginekologi - EditNur Rohmah Arsyad100% (1)
- ChildDocument17 pagesChildReyna Glorian HilarioNo ratings yet
- Thyroid SwellingDocument8 pagesThyroid SwellingDn Ezrinah Dn Esham50% (2)