Download as xls, pdf, or txt
You might also like
- Mock Recall Traceability Summary ReportDocument2 pagesMock Recall Traceability Summary ReportCharles J Kunjumon100% (4)
- Mock Recall Traceability Summary ReportDocument2 pagesMock Recall Traceability Summary ReportCharles J Kunjumon100% (4)
- Recall TemplateDocument5 pagesRecall TemplateEGa Sharfina100% (2)
- 02.SOP of Retention Sample (Raw Material)Document5 pages02.SOP of Retention Sample (Raw Material)Bejoy Karim100% (4)
- ASEAN TMHS GMP Training Chapter 4 Annex 1 SOP On Personal HygieneDocument5 pagesASEAN TMHS GMP Training Chapter 4 Annex 1 SOP On Personal Hygienesunny mgxNo ratings yet
- BRC 3.9.2 Trace Exercise SampleDocument10 pagesBRC 3.9.2 Trace Exercise SampleAmine Simo Jackson100% (1)
- Recall 5Document2 pagesRecall 5stevierayo100% (1)
- Product Recall and Withdrawal ProcedureDocument5 pagesProduct Recall and Withdrawal ProcedureNaizil Kareem100% (6)
- SOP C03 Equipment MaintenanceDocument2 pagesSOP C03 Equipment Maintenancesampathdt100% (1)
- Mock Tracebility Exercise ASQDocument24 pagesMock Tracebility Exercise ASQspp100% (8)
- Raw Material SupplierDocument9 pagesRaw Material SuppliersutharitesshNo ratings yet
- SOP of Rejection of Packaging MaterialDocument3 pagesSOP of Rejection of Packaging MaterialYousif67% (3)
- Mock Call Record Sample SheetDocument1 pageMock Call Record Sample SheetSiddharth soniNo ratings yet
- Mock Recall FormDocument1 pageMock Recall FormGonzales Choque Christian Jhonatan50% (2)
- Quality Manual: Pt. Ani Mitra Jaya Frozen ChepalopodDocument1 pageQuality Manual: Pt. Ani Mitra Jaya Frozen ChepalopodMia AgustinNo ratings yet
- SOP For Monitoring of Compressed Air - GasesDocument2 pagesSOP For Monitoring of Compressed Air - GasesAnonymous FZs3yBHh70% (1)
- Form Product Recall FormDocument1 pageForm Product Recall Formfisherkidd100% (3)
- Batch Manufacturing Record Capsule FormatDocument2 pagesBatch Manufacturing Record Capsule FormatAkik Sasmal100% (1)
- Quality Food Safety Policy 08Document2 pagesQuality Food Safety Policy 08Mohit ShuklaNo ratings yet
- GMP StatementDocument2 pagesGMP StatementkaransinghraiNo ratings yet
- Stability Study Guidance ProtocolDocument10 pagesStability Study Guidance ProtocolManish shankarpure100% (2)
- Purpose & Scope: Procedure For Product Withdrawal & RecallDocument3 pagesPurpose & Scope: Procedure For Product Withdrawal & Recallsajid waqas100% (1)
- Personal Hygiene SOPDocument2 pagesPersonal Hygiene SOPbikash sen100% (1)
- Glass and Brittle Plastics RegisterDocument3 pagesGlass and Brittle Plastics RegisterNaizil Kareem100% (1)
- Mock RecallDocument14 pagesMock RecallQuality DeptNo ratings yet
- 11.2.0 Product Recall ProcedureDocument12 pages11.2.0 Product Recall ProcedureZed100% (2)
- QA 5.15 Allergens Materials Handling General ProcedureDocument3 pagesQA 5.15 Allergens Materials Handling General ProcedureangeldrandevNo ratings yet
- Allergen Policy ExampleDocument1 pageAllergen Policy ExampleJorge G. ManzaneroNo ratings yet
- SOP Personnel HygieneDocument4 pagesSOP Personnel HygieneBejoy Karim100% (3)
- Sop For in - Process Fill Weight DeterminationDocument1 pageSop For in - Process Fill Weight DeterminationPrince MoniNo ratings yet
- Product RecallDocument18 pagesProduct Recallmarkandey guptaNo ratings yet
- Risk-Management Assessment of Visible-Residue LimitsDocument4 pagesRisk-Management Assessment of Visible-Residue LimitsPrince Moni100% (1)
- Haccp PlanDocument1 pageHaccp Planjlordmercader100% (1)
- Annual Product Quality Review APQR FormatDocument9 pagesAnnual Product Quality Review APQR FormatDr.Sivakumar Selvaraj100% (1)
- ReprocessingDocument3 pagesReprocessingswanandkul86% (7)
- Standard Operating Procedure Somatec: TITLE: SOP FOR DM Plant SanitizationDocument3 pagesStandard Operating Procedure Somatec: TITLE: SOP FOR DM Plant SanitizationMajed HossainNo ratings yet
- SOP For Drug Product Recall & Mock Recall - Pharma BeginnersDocument13 pagesSOP For Drug Product Recall & Mock Recall - Pharma BeginnersFled Nguyen0% (1)
- CCP3.5 Supplier Approval Procedure8Document5 pagesCCP3.5 Supplier Approval Procedure8Dutch Charming100% (1)
- Quality & Food Safety Manual: Wilverley Trading Estate 813/815 Bath Road Brislington Bristol Bs4 5NlDocument23 pagesQuality & Food Safety Manual: Wilverley Trading Estate 813/815 Bath Road Brislington Bristol Bs4 5NlMohamed100% (1)
- Food Repacking SOPDocument4 pagesFood Repacking SOPKayla OcampoNo ratings yet
- 38-SOP-Layout of Work Place and PremisesDocument4 pages38-SOP-Layout of Work Place and Premisesarun100% (3)
- 20.) SOP - Complaints, Recalls, & ReturnsDocument3 pages20.) SOP - Complaints, Recalls, & ReturnsMa. Angelica de GuzmanNo ratings yet
- Batch Packing RecordDocument1 pageBatch Packing RecordGBL 22100% (1)
- Protocol Jacketed MFG Tank LV02Document7 pagesProtocol Jacketed MFG Tank LV02pooja aswal100% (3)
- Transportation Validation ProtocolDocument2 pagesTransportation Validation ProtocolKhushboo Warhade100% (1)
- Activity 19 SOP On Pest ControlDocument2 pagesActivity 19 SOP On Pest ControlMarizel PormilosNo ratings yet
- HR001-00 Pest ControlDocument3 pagesHR001-00 Pest ControlBRIJENDRA KUMAR SINGHNo ratings yet
- Foreign Material Control PolicyDocument5 pagesForeign Material Control Policymonik manuel100% (1)
- FSSAI Food Recall Plan Sample Template Free PDF FileDocument4 pagesFSSAI Food Recall Plan Sample Template Free PDF FileAnees Alam0% (1)
- SOP For Cleaning of StirrerDocument2 pagesSOP For Cleaning of StirrerPrince Moni100% (1)
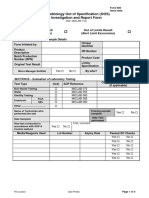
- Microbiology Out of Specification (OOS) Investigation and Report FormDocument3 pagesMicrobiology Out of Specification (OOS) Investigation and Report FormIra Nurjannah100% (1)
- 33-SOP-Measures For Prevention of Cross ContaminationDocument2 pages33-SOP-Measures For Prevention of Cross ContaminationarunNo ratings yet
- OOS InvestigationDocument5 pagesOOS Investigationmarkandey gupta100% (2)
- Personal Hygiene ProcedureDocument6 pagesPersonal Hygiene ProcedureSaad Zia100% (1)
- Finalized Draft of Intas Audit Compliance Report 05-12-20Document14 pagesFinalized Draft of Intas Audit Compliance Report 05-12-20DeepakNo ratings yet
- BMR - Reference - Moisturizing CreamDocument6 pagesBMR - Reference - Moisturizing CreamNIKHIL YEMUL100% (1)
- SOP For Operation of Bottle LabelingDocument4 pagesSOP For Operation of Bottle LabelingSolomonNo ratings yet
- G.2 Allergen Validation RecordDocument1 pageG.2 Allergen Validation RecordBibekNo ratings yet
- Consumer Complaint FormDocument4 pagesConsumer Complaint FormTiffany BvNo ratings yet
- Uc 304Document1 pageUc 304unseen worldNo ratings yet
- Personal Information: Application FormDocument3 pagesPersonal Information: Application Formmarklee torresNo ratings yet
- Guam Department of Labor Pandemic Unemployment Assistance Program Record of Contacts Made For WorkDocument2 pagesGuam Department of Labor Pandemic Unemployment Assistance Program Record of Contacts Made For WorkjjeonNo ratings yet
- British Bakels Limited Product Specification: Emergency ContactDocument13 pagesBritish Bakels Limited Product Specification: Emergency ContactCharles J KunjumonNo ratings yet
- Module 1 - Location, Layout, FacilitiesDocument45 pagesModule 1 - Location, Layout, FacilitiesCharles J KunjumonNo ratings yet
- Service Methodology For Halal: Certification of Products in Compliance With The Precepts of Islamic LawDocument5 pagesService Methodology For Halal: Certification of Products in Compliance With The Precepts of Islamic LawCharles J KunjumonNo ratings yet
- Food Traceability Template 2Document4 pagesFood Traceability Template 2Charles J KunjumonNo ratings yet
- Documents To Be Elaborated in Order To Meet ISO 22716 PDFDocument6 pagesDocuments To Be Elaborated in Order To Meet ISO 22716 PDFCharles J KunjumonNo ratings yet
- Checklist of ISO 9001 2015Document4 pagesChecklist of ISO 9001 2015Charles J KunjumonNo ratings yet
- Recalls: Mary Rait Craft Brew Alliance Manager of Regulatory ComplianceDocument11 pagesRecalls: Mary Rait Craft Brew Alliance Manager of Regulatory ComplianceCharles J KunjumonNo ratings yet
- Mock Recall Exercise DocumentationDocument3 pagesMock Recall Exercise DocumentationCharles J KunjumonNo ratings yet
- Quality Management PolicyDocument5 pagesQuality Management PolicyCharles J KunjumonNo ratings yet