Download as docx, pdf, or txt
You might also like
- Patophy of PudDocument4 pagesPatophy of PudClarence BravioNo ratings yet
- NCP Multiple SclerosisDocument2 pagesNCP Multiple SclerosisJaylord Verazon100% (2)
- Qtsoi Concept MapDocument5 pagesQtsoi Concept MapGenella BabantoNo ratings yet
- Acute Renal Failure DiagramDocument3 pagesAcute Renal Failure DiagramMichelle BarojaNo ratings yet
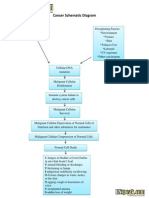
- Cancer Schematic DiagramDocument1 pageCancer Schematic DiagramCyrus De Asis100% (4)
- Nursing DepartmentDocument15 pagesNursing DepartmentJaylord VerazonNo ratings yet
- Semi Final Examination (Ips 1) : EsculentaDocument8 pagesSemi Final Examination (Ips 1) : EsculentaKenny TuanNo ratings yet
- Course Plan ON Bio-Chemistry: Bhopal (M.P.)Document6 pagesCourse Plan ON Bio-Chemistry: Bhopal (M.P.)amitNo ratings yet
- Hyperglycemic Hyperosmolar State - A Diabetic EmergencyDocument2 pagesHyperglycemic Hyperosmolar State - A Diabetic EmergencyNiken AninditaNo ratings yet
- Hyperosmolar Hyperglycemic StateDocument10 pagesHyperosmolar Hyperglycemic StateMirko S. León RguezNo ratings yet
- Esophagea L Cancer: By: Krizzia S. Bunagan-Legasi, RNDocument20 pagesEsophagea L Cancer: By: Krizzia S. Bunagan-Legasi, RNAnn SalvatierraNo ratings yet
- Pathophysiology of Multiple Myeloma OkDocument3 pagesPathophysiology of Multiple Myeloma OkRifa'atul MahmudahNo ratings yet
- Cerebrovascular Disease (Bleed)Document25 pagesCerebrovascular Disease (Bleed)Margaret Jenaw JenawNo ratings yet
- Systemic Lupus Erythematous: Precipitating Factors: Environmental Drug-Induced InfectionDocument10 pagesSystemic Lupus Erythematous: Precipitating Factors: Environmental Drug-Induced Infectioninah krizia lagueNo ratings yet
- Schistosomiasis (From Anatomy To Pathophysiology)Document10 pagesSchistosomiasis (From Anatomy To Pathophysiology)Tiger Knee100% (1)
- Example Case StudyDocument7 pagesExample Case StudyTerrena Lyn BlackmanNo ratings yet
- Cefadroxil: Antibiotic ClassDocument2 pagesCefadroxil: Antibiotic ClassTariNo ratings yet
- Vincristine (OncovinDocument4 pagesVincristine (Oncovin9959101161No ratings yet
- Ulcerative ColitisDocument9 pagesUlcerative Colitiskint manlangitNo ratings yet
- Vii. Pathophysiology A. AlgorithmDocument2 pagesVii. Pathophysiology A. AlgorithmJonna Mae TurquezaNo ratings yet
- Pathophy - Nephrotic SyndromeedDocument1 pagePathophy - Nephrotic Syndromeedianecunar100% (1)
- Pathophysiology of OsteomyelitisDocument2 pagesPathophysiology of Osteomyelitissorryandreosayanisalreadytaken100% (1)
- Liver Case StudyDocument6 pagesLiver Case StudyGhulam MustafaNo ratings yet
- PATHOPHYSIOLOGYDocument1 pagePATHOPHYSIOLOGYJeroham CoNo ratings yet
- Pathophysiology Precipitsting Factors: Predisposing FactorsDocument2 pagesPathophysiology Precipitsting Factors: Predisposing FactorsGeofrey MaglalangNo ratings yet
- Pa Tho Physiology Sle, CompDocument5 pagesPa Tho Physiology Sle, CompHassan Bj MarabongNo ratings yet
- HIV and Its TreatmentDocument24 pagesHIV and Its Treatmentaathira_kNo ratings yet
- ESRD PathophysiologyDocument2 pagesESRD Pathophysiologynursing concept mapsNo ratings yet
- CVDDocument67 pagesCVDRachel PerandoNo ratings yet
- Pathophysiology of OsteoarthritisDocument1 pagePathophysiology of OsteoarthritisGLADYS GARCIANo ratings yet
- Pathophysiology of PihDocument3 pagesPathophysiology of PihMargueretti Delos ReyesNo ratings yet
- Case Presentation NCM 102Document30 pagesCase Presentation NCM 102Jubille FerrarenNo ratings yet
- Influenza PATHOPHYSIOLOGYDocument3 pagesInfluenza PATHOPHYSIOLOGYElle RosalesNo ratings yet
- Cva Concept MapDocument1 pageCva Concept MapAnn Justine OrbetaNo ratings yet
- Pathophysiology of Inflammatory ResponseDocument1 pagePathophysiology of Inflammatory ResponseDeo FactuarNo ratings yet
- Pa Tho Physiology of RaDocument7 pagesPa Tho Physiology of Ralisalmar2008No ratings yet
- Epidemiology, Pathogenesis, and Pathology of NeuroblastomaDocument21 pagesEpidemiology, Pathogenesis, and Pathology of NeuroblastomaHandre PutraNo ratings yet
- End Stage Renal Disease: A. Pathophysiology A. Schematic DiagramDocument2 pagesEnd Stage Renal Disease: A. Pathophysiology A. Schematic DiagramSharmaine Camille de LeonNo ratings yet
- BPHDocument81 pagesBPHFlo Neri BerondoNo ratings yet
- Age Greater Than 60 Y/o Hereditary Precipitating Factors: Hypertension Increase Protein and Fat IntakeDocument3 pagesAge Greater Than 60 Y/o Hereditary Precipitating Factors: Hypertension Increase Protein and Fat Intakenursing concept mapsNo ratings yet
- Pathophysiology AppendicitisDocument3 pagesPathophysiology AppendicitisIra Krystel ReyesNo ratings yet
- Case Pres A1-RhdDocument11 pagesCase Pres A1-RhdCharm TanyaNo ratings yet
- Anatomy and Physiology For Bacterial MeningitisDocument4 pagesAnatomy and Physiology For Bacterial MeningitisynecesityNo ratings yet
- CKD - For Concept MappingDocument7 pagesCKD - For Concept MappingKennette Lim0% (1)
- "Acute Coronary Syndrome Non ST Elevation Myocardial Infarction, Hypertensive Cardiovascular Disease, Diabetes Mellitus Type 2, and Community Acquired Pneumonia" Client Centered PathophysiologyDocument3 pages"Acute Coronary Syndrome Non ST Elevation Myocardial Infarction, Hypertensive Cardiovascular Disease, Diabetes Mellitus Type 2, and Community Acquired Pneumonia" Client Centered PathophysiologyCarl Elexer Cuyugan Ano50% (2)
- Pathophysiology of Chronic Renal Failure: By: Jonnel Montoya Musngi BSN 4-BDocument1 pagePathophysiology of Chronic Renal Failure: By: Jonnel Montoya Musngi BSN 4-BKenrick Randell IbanaNo ratings yet
- Patho DengueDocument3 pagesPatho DengueLindy Shane BoncalesNo ratings yet
- Schematic Diag DMDocument1 pageSchematic Diag DMReynaKatNo ratings yet
- PathophysiologyDocument2 pagesPathophysiologyKarla Karina Dela CruzNo ratings yet
- Increased Serum Glucose Level (Hyperglycemia) 278.14 MG/DL (Normal: 70-100 MG/DL)Document3 pagesIncreased Serum Glucose Level (Hyperglycemia) 278.14 MG/DL (Normal: 70-100 MG/DL)Angel FiloteoNo ratings yet
- E000779 FullDocument19 pagesE000779 Fullmartina silalahiNo ratings yet
- V. Pathophysiology Modifiable: Non - ModifiableDocument2 pagesV. Pathophysiology Modifiable: Non - ModifiableMary Grace BanezNo ratings yet
- Pathophysiology of AllDocument1 pagePathophysiology of AllBGHMC PEDIAHONo ratings yet
- FINAL CASE-GOUT... PrintDocument69 pagesFINAL CASE-GOUT... PrintVelz Noli100% (3)
- Anatomy and Phsyiology of MeningococcemiaDocument2 pagesAnatomy and Phsyiology of MeningococcemiaKevin Comahig100% (1)
- 6 PathophysiologyDocument2 pages6 PathophysiologyAJ SnowhiNo ratings yet
- Pathophysiology Cushing S SyndromeDocument4 pagesPathophysiology Cushing S SyndromeMaria Luisa VillalunaNo ratings yet
- Kaposi's SarcomaDocument6 pagesKaposi's SarcomaveremkovichNo ratings yet
- Anatomy and PhysiologyDocument5 pagesAnatomy and Physiologyjohnbech07No ratings yet
- Pa Add Mga Ito Kapag May KulangDocument5 pagesPa Add Mga Ito Kapag May KulangJaylord VerazonNo ratings yet
- Schematic Pathophy DkaDocument2 pagesSchematic Pathophy DkaMaria Francheska OsiNo ratings yet
- Diabetic KetoacidosisDocument11 pagesDiabetic KetoacidosisYoung brosNo ratings yet
- Homeostatis Principles and Regulation of Glucose in BloodDocument13 pagesHomeostatis Principles and Regulation of Glucose in Bloodk75544863No ratings yet
- AsncudDocument2 pagesAsncudJaylord VerazonNo ratings yet
- Nursing DepartmentDocument10 pagesNursing DepartmentJaylord VerazonNo ratings yet
- Activity 4 Paper Work The Influence of Cultural and Health Belief System On Health Care PracticesDocument4 pagesActivity 4 Paper Work The Influence of Cultural and Health Belief System On Health Care PracticesJaylord VerazonNo ratings yet
- In Partial Fulfillment: Small Study Group (SSG)Document9 pagesIn Partial Fulfillment: Small Study Group (SSG)Jaylord VerazonNo ratings yet
- JSVFDocument1 pageJSVFJaylord VerazonNo ratings yet
- Nursing DepartmentDocument29 pagesNursing DepartmentJaylord VerazonNo ratings yet
- Journal Making 2 CFE 106 2 Term: Title of The Journal Biblical Passage ContextDocument2 pagesJournal Making 2 CFE 106 2 Term: Title of The Journal Biblical Passage ContextJaylord VerazonNo ratings yet
- Nursing DepartmentDocument14 pagesNursing DepartmentJaylord VerazonNo ratings yet
- NCP SciDocument3 pagesNCP SciJaylord VerazonNo ratings yet
- NCP - Major Depressive DisorderDocument7 pagesNCP - Major Depressive DisorderJaylord Verazon100% (1)
- Impaired Physical Mobility Related To Application of Traction or Cast As Evidenced by AssessmentDocument13 pagesImpaired Physical Mobility Related To Application of Traction or Cast As Evidenced by AssessmentJaylord VerazonNo ratings yet
- NCP GbsDocument2 pagesNCP GbsJaylord VerazonNo ratings yet
- Assessment Nursing Diagnosis Pathophysiology/ Scientific Explanation Planning Intervention Rationale EvaluationDocument4 pagesAssessment Nursing Diagnosis Pathophysiology/ Scientific Explanation Planning Intervention Rationale EvaluationJaylord VerazonNo ratings yet
- Nursing Care Plan For Hip Fracture Assessment Diagnosis Rationale Goal & Objectives Interventions Rationale EvaluationDocument1 pageNursing Care Plan For Hip Fracture Assessment Diagnosis Rationale Goal & Objectives Interventions Rationale EvaluationJaylord Verazon100% (1)
- Comprehensive Nursing Care PlanDocument3 pagesComprehensive Nursing Care PlanJaylord VerazonNo ratings yet
- Diagnostic EvaluationDocument29 pagesDiagnostic EvaluationJaylord VerazonNo ratings yet
- Verazon, Bsn3a-Myastenia NCPDocument5 pagesVerazon, Bsn3a-Myastenia NCPJaylord VerazonNo ratings yet
- Ancheta Et Al Handwashing - Chap4Document53 pagesAncheta Et Al Handwashing - Chap4Jaylord VerazonNo ratings yet
- Chemotherapy PPTDocument58 pagesChemotherapy PPTJaylord Verazon100% (1)
- Iridology and HypoglycemiaDocument15 pagesIridology and Hypoglycemiasohail_mashwnaiNo ratings yet
- Codex Stan 1-1985 Labelling of Prepackaged GoodsDocument7 pagesCodex Stan 1-1985 Labelling of Prepackaged GoodsvabimhahNo ratings yet
- Fortnightly Test Series: (For NEET/AIIMS-2019-2021)Document4 pagesFortnightly Test Series: (For NEET/AIIMS-2019-2021)Madhavkrishnan S100% (1)
- Lab 11 BIOCHEM REPORTDocument8 pagesLab 11 BIOCHEM REPORTAna LuisaNo ratings yet
- Basic Energy SystemDocument10 pagesBasic Energy SystemMozil Fadzil KamarudinNo ratings yet
- Rock Candy Lab ReportDocument3 pagesRock Candy Lab Reportapi-328384351100% (1)
- Jumping Jacks LabDocument4 pagesJumping Jacks Labapi-237677548100% (1)
- LWT - Food Science and Technology: A A B ADocument6 pagesLWT - Food Science and Technology: A A B ACarlos BispoNo ratings yet
- F3 - Bio - Final Exam - MCQs - WT Ans - Final - 110526Document14 pagesF3 - Bio - Final Exam - MCQs - WT Ans - Final - 110526jonas hoNo ratings yet
- Carbohydrates WorksheetDocument3 pagesCarbohydrates Worksheetaanyaverma267No ratings yet
- Rapoport 2012Document16 pagesRapoport 2012rehena mojammelNo ratings yet
- PAS I Exercise Discussion Compressed 231124 171104Document156 pagesPAS I Exercise Discussion Compressed 231124 171104Suryadi SuryadiNo ratings yet
- Biology Teachers' Manual PDFDocument72 pagesBiology Teachers' Manual PDFAndrewNo ratings yet
- Effect of Concentration of Sargassum Polycystum and Fermentation Time On Thickness and Yield of Nata de SargassumDocument5 pagesEffect of Concentration of Sargassum Polycystum and Fermentation Time On Thickness and Yield of Nata de SargassumMamta AgarwalNo ratings yet
- 1 - Photosynthesis and AssimilationDocument19 pages1 - Photosynthesis and AssimilationJasmine VS032689No ratings yet
- Module5 MARCHMIDTERMfinalmodule Biochemwithpages2021-22Document15 pagesModule5 MARCHMIDTERMfinalmodule Biochemwithpages2021-22Maden betoNo ratings yet
- Investigatory Project: Comparative Study ofDocument14 pagesInvestigatory Project: Comparative Study ofPradeep LenkaNo ratings yet
- Honey Its Characteristics Sensory Aspects and Applications-2Document18 pagesHoney Its Characteristics Sensory Aspects and Applications-2Zeina ZwayhedNo ratings yet
- Biochemistry - Reviewer (Carbohydrates)Document8 pagesBiochemistry - Reviewer (Carbohydrates)hi hoNo ratings yet
- CarbohydratesDocument17 pagesCarbohydratesNimkel L. SariqueNo ratings yet
- Bio Trial SPM 2007 Paper 3Document4 pagesBio Trial SPM 2007 Paper 3cmeeflyNo ratings yet
- Non-Digestible Oligosaccharides: A Review: Solange I. Mussatto, Ismael M. MancilhaDocument11 pagesNon-Digestible Oligosaccharides: A Review: Solange I. Mussatto, Ismael M. MancilhaPatrícia Felix ÁvilaNo ratings yet
- Sugar Term Project - 1Document4 pagesSugar Term Project - 1api-602532043No ratings yet
- Fdocuments - in Study The Rate of Fermentation of Fruits and Vegetables JuicesDocument9 pagesFdocuments - in Study The Rate of Fermentation of Fruits and Vegetables JuicesabinavNo ratings yet
- Respiration CHP 7 Biology Form 4Document24 pagesRespiration CHP 7 Biology Form 4Banu PriyaNo ratings yet
- Physical ScienceDocument117 pagesPhysical Sciencechi582552No ratings yet
- CarbsDocument40 pagesCarbsAnonymous eDD0YqzPMNo ratings yet
- Simp DoDocument2 pagesSimp DohealthyprettywiseNo ratings yet