Download as pdf or txt
You might also like
- Cellular and Molecular Immunology 9th Edition Abbas Test BankDocument4 pagesCellular and Molecular Immunology 9th Edition Abbas Test Bankdrkevinlee03071984jki100% (32)
- The European Trauma Course Manual: Edition 4.0Document10 pagesThe European Trauma Course Manual: Edition 4.0Ghenea Catalin-StefanNo ratings yet
- Prefrontal Lobotomy: January 2015Document7 pagesPrefrontal Lobotomy: January 2015duaNo ratings yet
- The Double Chin Posture: Posterior Sagittal Shift in Cervical DystoniaDocument3 pagesThe Double Chin Posture: Posterior Sagittal Shift in Cervical DystoniaDr-Asit Kumar ParidaNo ratings yet
- Annals of Neurology - 2008 - HamaniDocument5 pagesAnnals of Neurology - 2008 - HamaniEccoNo ratings yet
- Vlaeyen 2021 Low Back PainDocument16 pagesVlaeyen 2021 Low Back PainThawanny de CarvalhoNo ratings yet
- (Douglas W. Zochodne) Neurobiology of Peripheral NDocument318 pages(Douglas W. Zochodne) Neurobiology of Peripheral NImmer Armendáriz BetancourtNo ratings yet
- Low Back PainDocument15 pagesLow Back PainwidiaNo ratings yet
- Nijs Et Al 2021 LANCET RheumatologyDocument10 pagesNijs Et Al 2021 LANCET RheumatologyVicaroNo ratings yet
- Spine: Essential Neurosurgery For Medical StudentsDocument29 pagesSpine: Essential Neurosurgery For Medical StudentsAndreea IduNo ratings yet
- Oral Orthopedic Splint For The Treatment of Cervical DystoniaDocument8 pagesOral Orthopedic Splint For The Treatment of Cervical DystoniaCatalina Soler LioiNo ratings yet
- Volume: 03 Issue: 03 - May-Jun 2022Document4 pagesVolume: 03 Issue: 03 - May-Jun 2022Central Asian StudiesNo ratings yet
- Intertrochanteric FractureDocument43 pagesIntertrochanteric FractureZed P. EstalillaNo ratings yet
- The Treatment of Neck and Upper Back Pain With AcuDocument6 pagesThe Treatment of Neck and Upper Back Pain With AcuMohmmad Hossein NazariNo ratings yet
- Luxacion FacetariaDocument4 pagesLuxacion FacetariaBruno HazlebyNo ratings yet
- Sensibiliza o Central Nas Dores CR Nicas REVIEW LANCET 2021 - Open AccessDocument10 pagesSensibiliza o Central Nas Dores CR Nicas REVIEW LANCET 2021 - Open AccessRichard Mezadri ViebrantzNo ratings yet
- Draft 1Document13 pagesDraft 1api-581925910No ratings yet
- Ultrasound-Guided Nerve Blocks in The Head and Neck For Chronic Pain Management - The Anatomy, Sonoanatomy, and ProcedureDocument16 pagesUltrasound-Guided Nerve Blocks in The Head and Neck For Chronic Pain Management - The Anatomy, Sonoanatomy, and Proceduremarcus moraisNo ratings yet
- Myfirst 13724Document4 pagesMyfirst 13724simonyanNo ratings yet
- JCM 11 04184Document18 pagesJCM 11 04184Sky LarNo ratings yet
- Diagnosis of Space Occupying Lesions of BrainDocument3 pagesDiagnosis of Space Occupying Lesions of BrainsarahNo ratings yet
- Acu Accident LumbarDocument2 pagesAcu Accident Lumbarrswongym449No ratings yet
- BellsPalsy JNNP 2015Document8 pagesBellsPalsy JNNP 2015Marsya Yulinesia LoppiesNo ratings yet
- Post Lumbar Puncture Vertebral Collapse: Discitis andDocument3 pagesPost Lumbar Puncture Vertebral Collapse: Discitis andRohit GowdaNo ratings yet
- Case 1-2022: A 67-Year-Old Man With Motor Neuron Disease and Odd Behaviors During SleepDocument8 pagesCase 1-2022: A 67-Year-Old Man With Motor Neuron Disease and Odd Behaviors During Sleeppogesil46No ratings yet
- MusculoskeletalDocument8 pagesMusculoskeletalAbigailNo ratings yet
- Axillary Nerve Palsy and Deltoid Muscle AtonyDocument12 pagesAxillary Nerve Palsy and Deltoid Muscle AtonyLaura CandussiNo ratings yet
- The Basic Science of Pain ManagementDocument10 pagesThe Basic Science of Pain ManagementjacksonmpNo ratings yet
- Violence, Mental Illness and The BrainDocument13 pagesViolence, Mental Illness and The BrainAdriana Ornelas Aguirre100% (1)
- General Principles of NeurologyDocument8 pagesGeneral Principles of NeurologyCARZ 42No ratings yet
- Spinal Cord Detethering Without Laminectomy or LamDocument2 pagesSpinal Cord Detethering Without Laminectomy or LamLala CheeseNo ratings yet
- DBS, PerlmutterDocument32 pagesDBS, PerlmutterSebastiano Della CasaNo ratings yet
- Katz 2008Document8 pagesKatz 2008rulitoss_41739No ratings yet
- BJSM 1Document14 pagesBJSM 1MariaNo ratings yet
- Peroneal Nerve Palsy PDFDocument10 pagesPeroneal Nerve Palsy PDFChristian Reza WibowoNo ratings yet
- Post-Traumatic Neuroma After Hair Transplantation: LettersandcommunicationsDocument2 pagesPost-Traumatic Neuroma After Hair Transplantation: LettersandcommunicationsNishanthini AnnamalaiNo ratings yet
- Change in Psychiatric Symptoms in A Bipolar Patient Revealing Endocranial Extension of A Frontal MucoceleDocument3 pagesChange in Psychiatric Symptoms in A Bipolar Patient Revealing Endocranial Extension of A Frontal MucoceleIJAR JOURNALNo ratings yet
- Conversion Disorder and Spinal Cord Injury Case ReportDocument5 pagesConversion Disorder and Spinal Cord Injury Case ReportHerald Scholarly Open AccessNo ratings yet
- An Uncommon Disease With A Common Presentation Severe Back Pain and Diffuse Neuropathy in Two Cases of Hereditary Neuropathy With Liability To Pressure PalsyDocument3 pagesAn Uncommon Disease With A Common Presentation Severe Back Pain and Diffuse Neuropathy in Two Cases of Hereditary Neuropathy With Liability To Pressure PalsyAthenaeum Scientific PublishersNo ratings yet
- Enthesitis WeismanDocument1 pageEnthesitis WeismanDaniel AndryNo ratings yet
- The Associated Factors and Clinical Features Of.10Document7 pagesThe Associated Factors and Clinical Features Of.10Vinay VivekNo ratings yet
- General Principles in The Medical and Surgical Management of Spinal Infections A Multidisciplinary ApproachDocument16 pagesGeneral Principles in The Medical and Surgical Management of Spinal Infections A Multidisciplinary Approachdr.maulanahutabaratNo ratings yet
- PhysiotherapyDocument10 pagesPhysiotherapyHafizur RahmanNo ratings yet
- 2.5 NotesDocument7 pages2.5 NotesKenneth MelchorNo ratings yet
- Predicting Migraine ResponsivenessDocument5 pagesPredicting Migraine ResponsivenessfarmacialmoxcentralNo ratings yet
- Anosognosia, Denial, and Other Disorders of Phenomenological ExperienceDocument15 pagesAnosognosia, Denial, and Other Disorders of Phenomenological ExperienceAlan AlvídrezNo ratings yet
- Non Traumatic Skull FractureDocument2 pagesNon Traumatic Skull FractureBagus Andi PramonoNo ratings yet
- Psico CirugiaDocument24 pagesPsico CirugiaJuliana MartinezNo ratings yet
- Kwon World Neurosurgery 2016Document4 pagesKwon World Neurosurgery 2016Churl-Su KwonNo ratings yet
- Rehabilitation in Transverse MyelitisDocument16 pagesRehabilitation in Transverse MyelitisDaurian GarrandesNo ratings yet
- Cefalea Por Hipotension Complicada Con Herniacion Central Por Hematomas SubduralesDocument7 pagesCefalea Por Hipotension Complicada Con Herniacion Central Por Hematomas SubduralesFarid Santiago Abedrabbo LombeydaNo ratings yet
- 113 PerkinsDocument1 page113 PerkinssimonyanNo ratings yet
- Jurnal RMDocument4 pagesJurnal RMFandie PratamaNo ratings yet
- Cranial and Fascial Distortion Techniques Used As Complementary Treatments To Alleviate Migraine Headache: A Case ReportDocument4 pagesCranial and Fascial Distortion Techniques Used As Complementary Treatments To Alleviate Migraine Headache: A Case ReportLadykaNo ratings yet
- Duplication of The External Auditory Canal Two CasDocument5 pagesDuplication of The External Auditory Canal Two CasIvana SupitNo ratings yet
- Cefalea en Racimos Por DISECCION CAROTIDEADocument6 pagesCefalea en Racimos Por DISECCION CAROTIDEAFarid Santiago Abedrabbo LombeydaNo ratings yet
- Neurosurgical Treatment of PainDocument41 pagesNeurosurgical Treatment of PainAishwarya PoojaryNo ratings yet
- Conversion, Factitious Disorder and Malingering A Distinct Pattern or A ContinuumDocument10 pagesConversion, Factitious Disorder and Malingering A Distinct Pattern or A ContinuumPankhuri MishraNo ratings yet
- 39 Full-2Document5 pages39 Full-2ALEXIA CEDILLO LEZAMANo ratings yet
- Chaptar 30 Degenerative Spine DiseaseDocument9 pagesChaptar 30 Degenerative Spine DiseaseAbraham SaldañaNo ratings yet
- Spinal Segmental Sensitization As A Common OriginDocument8 pagesSpinal Segmental Sensitization As A Common OriginRossangel Huapaya RomeroNo ratings yet
- The Dislocated Brain: Innovation in Traumatic Brain Injury and IrrigationFrom EverandThe Dislocated Brain: Innovation in Traumatic Brain Injury and IrrigationRating: 5 out of 5 stars5/5 (2)
- Grafik Preterm FENTON 2013 Laki-LakiDocument1 pageGrafik Preterm FENTON 2013 Laki-LakiEmma FitrianaNo ratings yet
- Length-For-Age GIRLS: Birth To 6 Months (Z-Scores)Document15 pagesLength-For-Age GIRLS: Birth To 6 Months (Z-Scores)Emma FitrianaNo ratings yet
- Epidemiological Characteristics of Malassezia Folliculitis and Use of The May-Grunwald-Giwmsa Stain To Diagnose The InfectionDocument8 pagesEpidemiological Characteristics of Malassezia Folliculitis and Use of The May-Grunwald-Giwmsa Stain To Diagnose The InfectionEmma FitrianaNo ratings yet
- Follicular Contact Dermatitia Revisited A Review Emphasizing Neomycin Associated Follicular Contact DermatitisDocument8 pagesFollicular Contact Dermatitia Revisited A Review Emphasizing Neomycin Associated Follicular Contact DermatitisEmma FitrianaNo ratings yet
- Cue and Clue Problem List Idx PDX PTX Pmo PedDocument5 pagesCue and Clue Problem List Idx PDX PTX Pmo PedEmma FitrianaNo ratings yet
- Jurnal PDFDocument12 pagesJurnal PDFEmma FitrianaNo ratings yet
- Morning: MR Facilitator: Dr. Dikara Widyangga Sulfian Maulidy, Sp. PDDocument19 pagesMorning: MR Facilitator: Dr. Dikara Widyangga Sulfian Maulidy, Sp. PDEmma FitrianaNo ratings yet
- Clinical Practice Guideline (Update) : Adult SinusitisDocument39 pagesClinical Practice Guideline (Update) : Adult SinusitisEmma FitrianaNo ratings yet
- Medical and Surgical Management of Nasal PolypsDocument11 pagesMedical and Surgical Management of Nasal PolypsEmma FitrianaNo ratings yet
- TITLE: Pediatric Rhinosinusitis SOURCE: Grand Rounds Presentation, UTMB, Dept. of OtolaryngologyDocument10 pagesTITLE: Pediatric Rhinosinusitis SOURCE: Grand Rounds Presentation, UTMB, Dept. of OtolaryngologyEmma FitrianaNo ratings yet
- Aspirin: Action: Aspirin (But Not Other Salicylates) Powerfully Inhibits PlateletDocument4 pagesAspirin: Action: Aspirin (But Not Other Salicylates) Powerfully Inhibits PlateletAubrey Unique EvangelistaNo ratings yet
- Radiology NotesDocument24 pagesRadiology NotesAaron Raestas0% (1)
- DR Manavita Mahajan MD (PGI Chandigarh), FRCOG (London) SR Consultant Obstetrician & GynecologistDocument21 pagesDR Manavita Mahajan MD (PGI Chandigarh), FRCOG (London) SR Consultant Obstetrician & Gynecologistﻣﻠﻚ عيسىNo ratings yet
- Pharm Exam 4 ReviewDocument2 pagesPharm Exam 4 ReviewHwi GNDCNo ratings yet
- Developmental Disturbances of TeethDocument32 pagesDevelopmental Disturbances of TeethNada SaadNo ratings yet
- Preeklamsia Amp - dm18Document32 pagesPreeklamsia Amp - dm18Noni Minty BelantricNo ratings yet
- Form WHO Dewasa PDFDocument2 pagesForm WHO Dewasa PDFAbizar Agung WibawaNo ratings yet
- Biochemistry Reagents - ITA Kits - Promotional Tool 27th - August-2019-2Document23 pagesBiochemistry Reagents - ITA Kits - Promotional Tool 27th - August-2019-2Ajay DataniyaNo ratings yet
- Physical Examination FormatDocument7 pagesPhysical Examination FormatHiba V.ANo ratings yet
- Fluid, Electrolyte and Acid-Base Imbalance - Powerpoint - LectureDocument53 pagesFluid, Electrolyte and Acid-Base Imbalance - Powerpoint - Lecturezakaria hossainNo ratings yet
- Heart-Brain AxisDocument15 pagesHeart-Brain Axiscc vereNo ratings yet
- No. Nama Penyakit Kode Dan Nama Kode Diagnosa ICD 10Document20 pagesNo. Nama Penyakit Kode Dan Nama Kode Diagnosa ICD 10Yunia Indah Khumaira RNo ratings yet
- DocumentDocument128 pagesDocumentHardi OtoyNo ratings yet
- IsoxsuprineDocument1 pageIsoxsuprineAndrean EnriquezNo ratings yet
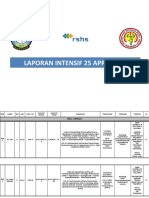
- Laporan Intensif 25 April 2021Document21 pagesLaporan Intensif 25 April 2021bosnia agusNo ratings yet
- Benign Lesion of The LarynxDocument17 pagesBenign Lesion of The Larynxadham bani younesNo ratings yet
- Part 2 HematologyDocument42 pagesPart 2 Hematology크리스찰이No ratings yet
- Sns vs. Ans: Somatic Nervous System (SNS)Document20 pagesSns vs. Ans: Somatic Nervous System (SNS)dave_1128No ratings yet
- Topic List Q&ADocument63 pagesTopic List Q&APop D. MadalinaNo ratings yet
- Name of Drug Action Indication Contraindication Side Effects Nursing Consideration AspirinDocument5 pagesName of Drug Action Indication Contraindication Side Effects Nursing Consideration AspirinPerpetual DaltaNo ratings yet
- 52 Q. Medicine 2nd Half PDFDocument15 pages52 Q. Medicine 2nd Half PDFFahad2036No ratings yet
- Lecture 3.5 Acute Abdomen in Gastrointenstinal-Dr. Adeodatus Yudha Handaya, SP.-KBD (2020)Document63 pagesLecture 3.5 Acute Abdomen in Gastrointenstinal-Dr. Adeodatus Yudha Handaya, SP.-KBD (2020)stefany huangNo ratings yet
- Nursing. Midwifery. Pharmacy. Medtech. CriminologyDocument5 pagesNursing. Midwifery. Pharmacy. Medtech. CriminologyJake CopradeNo ratings yet
- Sukoon New MAFDocument5 pagesSukoon New MAFJdNo ratings yet
- Radiology Case Report - Splenic AbscessDocument6 pagesRadiology Case Report - Splenic AbscessAbeebNo ratings yet
- How To Use Magic DeviceDocument11 pagesHow To Use Magic DeviceJavid QadirNo ratings yet
- Abdominal Wall, Omentum, Mesentery and RetroperitoneumDocument8 pagesAbdominal Wall, Omentum, Mesentery and RetroperitoneumRae Marie AquinoNo ratings yet
- Drug StudyDocument1 pageDrug StudyEdmarkmoises ValdezNo ratings yet