Download as pdf or txt
You might also like
- Fear and Loathing in FaerûnDocument84 pagesFear and Loathing in FaerûnDavide Gobbi100% (1)
- Sailing Full Sail ChecklistDocument100 pagesSailing Full Sail ChecklistJoshua Welbaum100% (4)
- DM7000 Plus User - Manual - Menu - 20220314 - en - ReleaseDocument122 pagesDM7000 Plus User - Manual - Menu - 20220314 - en - ReleaseKamil ÖzpamukçuNo ratings yet
- Analysis of VAERS Data at The State LevelDocument18 pagesAnalysis of VAERS Data at The State LevelDIANI GAMARRANo ratings yet
- Spinalvolfor LSCSDocument5 pagesSpinalvolfor LSCSmaurice falzonNo ratings yet
- Kelly 1996Document3 pagesKelly 1996Agustin CuryNo ratings yet
- X 9702500504Document6 pagesX 9702500504Anonymous ORleRrNo ratings yet
- PDF Bilateral Transverse Abdominal Plane Block Ropi and Bupivacaine in Cs PatinetDocument3 pagesPDF Bilateral Transverse Abdominal Plane Block Ropi and Bupivacaine in Cs PatinetdrbkhiraniNo ratings yet
- Ref 192Document4 pagesRef 192Carlos CulquichicónNo ratings yet
- ComparisonDocument6 pagesComparisonYvon ChrétienNo ratings yet
- Jurnal Fentanil Dan BucainDocument7 pagesJurnal Fentanil Dan BucainAdhiny IslamNo ratings yet
- Role of Pain Placebo Analgesia: Gordont, Fields FDocument4 pagesRole of Pain Placebo Analgesia: Gordont, Fields Fmaurina rizkiNo ratings yet
- Role of Pain Placebo Analgesia: Gordont, Fields FDocument4 pagesRole of Pain Placebo Analgesia: Gordont, Fields Fmaurina rizkiNo ratings yet
- PCA Con Tramadol o RemiDocument5 pagesPCA Con Tramadol o RemiChurrunchaNo ratings yet
- Postoperative Analgesia in Modified Radical Mastectomy Patients After Instillation of Bupivacaine Through Surgical Drains-1.en - IdDocument23 pagesPostoperative Analgesia in Modified Radical Mastectomy Patients After Instillation of Bupivacaine Through Surgical Drains-1.en - Idsatria divaNo ratings yet
- Analgesic Efficacity of Pfannenstiel Incision Infiltration With Ropivacaine 7.5Mg/Ml For Caesarean SectionDocument17 pagesAnalgesic Efficacity of Pfannenstiel Incision Infiltration With Ropivacaine 7.5Mg/Ml For Caesarean SectionboblenazeNo ratings yet
- Low Dose Levobupivacaıne 0.5% With Fentanyl in Spinal Anaesthesia For Transurethral Resection of Prostate SurgeryDocument6 pagesLow Dose Levobupivacaıne 0.5% With Fentanyl in Spinal Anaesthesia For Transurethral Resection of Prostate Surgeryblabarry1109No ratings yet
- Cont Infusion Vs Mand Bolus W PCEADocument6 pagesCont Infusion Vs Mand Bolus W PCEAk3 rschNo ratings yet
- Comparison of Epidural Anaesthesia With Ropiva-Caine 0.5% and Bupiva - Caine 0.5% For Caesarean SectionDocument6 pagesComparison of Epidural Anaesthesia With Ropiva-Caine 0.5% and Bupiva - Caine 0.5% For Caesarean SectionSantiago ValeroNo ratings yet
- SivevskiDocument12 pagesSivevskiPalwasha MalikNo ratings yet
- Walking Epidural: An Effective Method of Labour Pain ReliefDocument3 pagesWalking Epidural: An Effective Method of Labour Pain ReliefrahmaNo ratings yet
- JPNR 2022 S01 216+ (1815 1822)Document8 pagesJPNR 2022 S01 216+ (1815 1822)prabaNo ratings yet
- Comparison of Intrathecal Fentanyl and BuprenorphiDocument7 pagesComparison of Intrathecal Fentanyl and BuprenorphiAn JNo ratings yet
- Anaesthesia - January 1983 - NIGHTINGALE - Barbotage and Spinal AnaesthesiaDocument3 pagesAnaesthesia - January 1983 - NIGHTINGALE - Barbotage and Spinal AnaesthesiablackNo ratings yet
- Is Granisetron-Dexamethasone Combination Better ThanDocument8 pagesIs Granisetron-Dexamethasone Combination Better ThanGustomo PanantroNo ratings yet
- SynopsisDocument14 pagesSynopsisAqeel AhmadNo ratings yet
- Diamorfina SpinalDocument5 pagesDiamorfina SpinalAurora TrifaNo ratings yet
- Ref 6Document7 pagesRef 6Ferdi ArdiNo ratings yet
- 1085519Document5 pages1085519ABDUL WARIS BIN AYYUB BIN IMAM SAHEBNo ratings yet
- Synergistic Interaction Between Fentanyl and Bupivacaine Given Intrathecally For Labor AnalgesiaDocument11 pagesSynergistic Interaction Between Fentanyl and Bupivacaine Given Intrathecally For Labor AnalgesiaNurul Dwi LestariNo ratings yet
- Journal Homepage: - : IntroductionDocument8 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Pecs BlockDocument4 pagesPecs BlockSana AbbasNo ratings yet
- Comparative Study of Epidural 0.125% Bupivacaine With Butorphanol and Epidural 0.125% Bupivacaine With Nalbuphine For Postoperative Analgesia in Abdominal SurgeriesDocument7 pagesComparative Study of Epidural 0.125% Bupivacaine With Butorphanol and Epidural 0.125% Bupivacaine With Nalbuphine For Postoperative Analgesia in Abdominal SurgeriesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 1 s2.0 S0104001413001127 MainDocument8 pages1 s2.0 S0104001413001127 MainFrederica WiryawanNo ratings yet
- Comparative Study of Intrathecal Sufentanil Bupivacaine Versus Intrathecal Bupivacaine in Patients Undergoing Elective Cesarean SectionDocument5 pagesComparative Study of Intrathecal Sufentanil Bupivacaine Versus Intrathecal Bupivacaine in Patients Undergoing Elective Cesarean SectiontamiNo ratings yet
- 1 s2.0 S0007091217366175 MainDocument5 pages1 s2.0 S0007091217366175 MainMeutia LaksaniNo ratings yet
- Small-Dose Ketamine Infusion Improves Postoperative Analgesia and Rehabilitation After Total Knee ArthroplastyDocument6 pagesSmall-Dose Ketamine Infusion Improves Postoperative Analgesia and Rehabilitation After Total Knee ArthroplastyArturo AlcantaraNo ratings yet
- Transient Neurological Symptoms Following Spinal Anesthesia For Cesarean SectionDocument6 pagesTransient Neurological Symptoms Following Spinal Anesthesia For Cesarean SectionSuni AbrahamNo ratings yet
- Rba 40 5 331Document6 pagesRba 40 5 331Ana MariaNo ratings yet
- Arp2018 1486261Document5 pagesArp2018 1486261Sheren ElinNo ratings yet
- HindawiDocument6 pagesHindawiTaufiqo Nugraha SjachrilNo ratings yet
- AshrafDocument5 pagesAshrafJennifer GNo ratings yet
- GhimireDocument5 pagesGhimireJennifer GNo ratings yet
- Thesis Full PDFDocument144 pagesThesis Full PDFJayaprakash Kuppusamy80% (5)
- H. Aksoy, G. Gökahmeto ĞLU, M. Ak, Ü. Aksoy: European Review For Medical and Pharmacological SciencesDocument8 pagesH. Aksoy, G. Gökahmeto ĞLU, M. Ak, Ü. Aksoy: European Review For Medical and Pharmacological SciencesNadra SeptiadiNo ratings yet
- TAP Vs QL CesareanDocument7 pagesTAP Vs QL CesareanEmmanuel FortalezaNo ratings yet
- Exilis StudieDocument36 pagesExilis StudiesdwNo ratings yet
- Ijhs 8383+12635 12654Document20 pagesIjhs 8383+12635 12654Muhammad Daniala SyuhadaNo ratings yet
- Obstetrics AnesthesiaDocument31 pagesObstetrics AnesthesiaNorfarhanah ZakariaNo ratings yet
- Abrams, 2015Document12 pagesAbrams, 2015choirin nurNo ratings yet
- Preoperative Paravertebral Block and Chronic Pain After Breast Cancer Surgery: A Double-Blind Randomized TrialDocument13 pagesPreoperative Paravertebral Block and Chronic Pain After Breast Cancer Surgery: A Double-Blind Randomized TrialRafly SuwandhiNo ratings yet
- Bolo Vs PerfusiónDocument6 pagesBolo Vs Perfusión1cucu0No ratings yet
- Intrathecal Fentanyl For Prevention of Shivering in Spinal Anesthesia in Cesarean SectionDocument5 pagesIntrathecal Fentanyl For Prevention of Shivering in Spinal Anesthesia in Cesarean SectionMuhammad Habibi NstNo ratings yet
- Manasi Abstract KDocument2 pagesManasi Abstract KjslgreenhomesNo ratings yet
- PRM2017 1721460 PDFDocument6 pagesPRM2017 1721460 PDFmikoNo ratings yet
- Lehmann 2005Document18 pagesLehmann 2005asdasdasdNo ratings yet
- Comparative Time Achieved VAS 3 On Oxycodone and Fentanyl Intravenous Continue As Post-Operative AnalgesiaDocument3 pagesComparative Time Achieved VAS 3 On Oxycodone and Fentanyl Intravenous Continue As Post-Operative AnalgesiaFranz Josef TariganNo ratings yet
- 1207-Article Text-3856-2-10-20210722Document4 pages1207-Article Text-3856-2-10-20210722GREESTYNo ratings yet
- Loane HDocument7 pagesLoane HVan DaoNo ratings yet
- International Journal of Obstetric AnesthesiaDocument6 pagesInternational Journal of Obstetric Anesthesiaanita pratiwiNo ratings yet
- Penentuan Dosis Efektif Bupivacaine Hiperbarik 0,5% Berdasarkan Tinggi Badan Untuk Bedah Sesar Dengan Blok SubarakhnoidDocument9 pagesPenentuan Dosis Efektif Bupivacaine Hiperbarik 0,5% Berdasarkan Tinggi Badan Untuk Bedah Sesar Dengan Blok SubarakhnoidChrist YanuarNo ratings yet
- EVALUATION OF THE INFLUENCE OF TWO DIFFERENT SYSTEMS OF ANALGESIA AND THE NASOGASTRIC TUBE ON THE INCIDENCE OF POSTOPERATIVE NAUSEA AND VOMITING IN CARDIAC SURGERYFrom EverandEVALUATION OF THE INFLUENCE OF TWO DIFFERENT SYSTEMS OF ANALGESIA AND THE NASOGASTRIC TUBE ON THE INCIDENCE OF POSTOPERATIVE NAUSEA AND VOMITING IN CARDIAC SURGERYNo ratings yet
- Absolute Obstetric Anesthesia Review: The Complete Study Guide for Certification and RecertificationFrom EverandAbsolute Obstetric Anesthesia Review: The Complete Study Guide for Certification and RecertificationNo ratings yet
- CSC Form No 211 (Medical-Blank)Document1 pageCSC Form No 211 (Medical-Blank)Anonymous qg3W2rsRcGNo ratings yet
- Master Rotation Plan-3Rd Year Basic-Bsc Nursing: Indira Gandhi College of NursingDocument5 pagesMaster Rotation Plan-3Rd Year Basic-Bsc Nursing: Indira Gandhi College of Nursingkuruvagadda sagarNo ratings yet
- NICU Flow Chart KangarooDocument6 pagesNICU Flow Chart KangarooBasavarajNo ratings yet
- Lippincott S Anesthesia Review 1001 Questions And.20Document1 pageLippincott S Anesthesia Review 1001 Questions And.20Reem Salem0% (1)
- Es0345 Electrosurgical Unit PDFDocument16 pagesEs0345 Electrosurgical Unit PDFJairo Andrés Damelinez TorresNo ratings yet
- HOOKWORM TransDocument4 pagesHOOKWORM TransDavid Ryan MangawilNo ratings yet
- Workflow Jan 2021Document3 pagesWorkflow Jan 2021Kathrine Ann FavoritoNo ratings yet
- DGDA GVP Guideline Sep 2023Document70 pagesDGDA GVP Guideline Sep 2023Vandana ReddyNo ratings yet
- Revised OK Sa DepEd Forms 2019Document16 pagesRevised OK Sa DepEd Forms 2019Annielou OliveraNo ratings yet
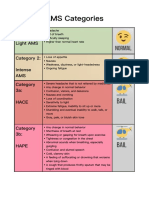
- AMS Categories: Category 1: Light AMS Category 2: Intense AMS Category 3a: HaceDocument1 pageAMS Categories: Category 1: Light AMS Category 2: Intense AMS Category 3a: HaceyyggvcNo ratings yet
- Phlebotomy - 2021Document36 pagesPhlebotomy - 2021Sumathi AkshayaNo ratings yet
- Press Information Bureau162645Document3 pagesPress Information Bureau162645Shrinivas A BNo ratings yet
- LMHL-MICRO-Examination of Cerebral Spinal Fluid-001Document5 pagesLMHL-MICRO-Examination of Cerebral Spinal Fluid-001Steve KabambeNo ratings yet
- MAPEH PE9 Q2 Modules 12Document14 pagesMAPEH PE9 Q2 Modules 12Jan Den Saul DalanNo ratings yet
- Beneview - t8 Operational ManualDocument290 pagesBeneview - t8 Operational ManualIrakli JibladzeNo ratings yet
- FROLIC Studio - Decontamination Box - HygCen Test Report PDFDocument8 pagesFROLIC Studio - Decontamination Box - HygCen Test Report PDFeduardo jesusNo ratings yet
- SC Auto Surg - LuaDocument5 pagesSC Auto Surg - Luanew kitsuenNo ratings yet
- Mountain Province Vaccination Monitoring: Data (As of October 24-30, 2021)Document14 pagesMountain Province Vaccination Monitoring: Data (As of October 24-30, 2021)Janice DinesNo ratings yet
- Ipcr-Samillano, John Vanne D. Samillano, Rmt-MaayonDocument3 pagesIpcr-Samillano, John Vanne D. Samillano, Rmt-MaayonGeline Joy D. SamillanoNo ratings yet
- Review Article: V. K. Agnihotri Et Al / Int. J. Res. Ayurveda Pharm. 6 (6), Nov - Dec 2015Document6 pagesReview Article: V. K. Agnihotri Et Al / Int. J. Res. Ayurveda Pharm. 6 (6), Nov - Dec 2015Pranoti ShettiNo ratings yet
- Catheterization ChecklistDocument5 pagesCatheterization ChecklistEmerald IsleNo ratings yet
- Suturing RemovalDocument16 pagesSuturing Removalandrie febriansyahNo ratings yet
- HSTP II HMIS Hospital Heath Centre and Health PostDocument367 pagesHSTP II HMIS Hospital Heath Centre and Health PostDagmawitNo ratings yet
- Nin/Pmjay Id Name of The Vaccination Site Category Type Latitude LongitudeDocument18 pagesNin/Pmjay Id Name of The Vaccination Site Category Type Latitude LongitudeRappadi LSFPNo ratings yet
- Instilling Nose DropsDocument4 pagesInstilling Nose DropsHarvey T. Dato-onNo ratings yet
- Guide To The Quality EDQM For Human ApplicationDocument462 pagesGuide To The Quality EDQM For Human ApplicationFREDY ALONSO MANTILLA CABALLERONo ratings yet