Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- DiareDocument4 pagesDiareDyerik LilingNo ratings yet
- Molecular Sciences. 2020Document4 pagesMolecular Sciences. 2020Dyerik LilingNo ratings yet
- Diagnosis Dan Tatalaksana Konjungtival Melanoma - Ericka Febriyanti Pratama PutriDocument14 pagesDiagnosis Dan Tatalaksana Konjungtival Melanoma - Ericka Febriyanti Pratama PutriDyerik LilingNo ratings yet
- Malignant Melanoma: A Case Report With Literature ReviewDocument6 pagesMalignant Melanoma: A Case Report With Literature ReviewDyerik LilingNo ratings yet
- Metastatic Malignant Melanoma: A Case StudyDocument3 pagesMetastatic Malignant Melanoma: A Case StudyDyerik LilingNo ratings yet
- Malignant Melanoma: Healthcare November 2013Document20 pagesMalignant Melanoma: Healthcare November 2013Dyerik LilingNo ratings yet
- Cutaneous Melanoma - Guidelines For Diagnostics and Therapy in 2016Document17 pagesCutaneous Melanoma - Guidelines For Diagnostics and Therapy in 2016Dyerik LilingNo ratings yet
- A 60-Year-Old Female With Metastatic Malignant Melanoma of The Scalp Responding To IpilimumabDocument4 pagesA 60-Year-Old Female With Metastatic Malignant Melanoma of The Scalp Responding To IpilimumabDyerik LilingNo ratings yet
- Case Report: A Case of Malignant Melanoma Arising in Mediastinal Malignant TeratomaDocument6 pagesCase Report: A Case of Malignant Melanoma Arising in Mediastinal Malignant TeratomaDyerik LilingNo ratings yet
- Gestational Trophoblastic Disease The Philippine ExperienceDocument5 pagesGestational Trophoblastic Disease The Philippine ExperienceksescletoNo ratings yet
- Biology Investigatory Project: Study On CancerDocument24 pagesBiology Investigatory Project: Study On CancerAthiya Zainab100% (1)
- Tumores Mucinosos Del Ovario Con Nodulo Mural Case Report 2020Document10 pagesTumores Mucinosos Del Ovario Con Nodulo Mural Case Report 2020Jairo Lino BNo ratings yet
- Pathophysiologi Laryngeal CancerDocument13 pagesPathophysiologi Laryngeal CancerIvan Kurniadi100% (4)
- CancerDocument4 pagesCancerJan Jamison ZuluetaNo ratings yet
- Algorithm ColonosDocument1 pageAlgorithm ColonosDavNo ratings yet
- Absite Questions MissedDocument11 pagesAbsite Questions MissedVikram Patel100% (1)
- Management of Breast DiseaseDocument111 pagesManagement of Breast DiseaseVikkineshwaran Siva SubramaniamNo ratings yet
- Ewing SarcomaDocument12 pagesEwing SarcomaVany MaksumNo ratings yet
- ESMO Preceptorship On Breast Cancer Lisbon SepteDocument73 pagesESMO Preceptorship On Breast Cancer Lisbon SepteStancaMihaiAlexandruNo ratings yet
- Dr. Burzynski Antinewoplastons Cancer TreatmentDocument13 pagesDr. Burzynski Antinewoplastons Cancer TreatmentJo RoNo ratings yet
- Cervical Cancer Screening - DOH Standard - May 2018Document14 pagesCervical Cancer Screening - DOH Standard - May 2018Basil al-hashaikehNo ratings yet
- Caderno de Questões - TwentyFour Dia 2Document2 pagesCaderno de Questões - TwentyFour Dia 2Guilherme MacedoNo ratings yet
- Salivary GlandsDocument43 pagesSalivary GlandsSuha ManaaNo ratings yet
- Breast ScreeningDocument87 pagesBreast ScreeningDira NidausshafaNo ratings yet
- Malignant Neoplasm (Ovarian Cancer)Document4 pagesMalignant Neoplasm (Ovarian Cancer)nursing concept mapsNo ratings yet
- S. G. Silverberg (Ed) : Principles and Practice of Surgical Pathology and Cytopathology. Churchill LivingstoneDocument1 pageS. G. Silverberg (Ed) : Principles and Practice of Surgical Pathology and Cytopathology. Churchill LivingstoneasadsNo ratings yet
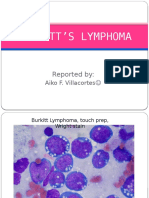
- Burkitt S LymphomaDocument12 pagesBurkitt S LymphomaAiko VillacortesNo ratings yet
- Lions Club International District 325 A 1 Nepal September NewsletterDocument28 pagesLions Club International District 325 A 1 Nepal September NewsletternittamNo ratings yet
- For Case 2Document2 pagesFor Case 2Nneka Andrea DatilesNo ratings yet
- K.S. Clifford Chao-Practical Essentials of Intensity Modulated Radiation Therapy-LWW (2013) (1) - 19-23Document5 pagesK.S. Clifford Chao-Practical Essentials of Intensity Modulated Radiation Therapy-LWW (2013) (1) - 19-23Roger Moreyra QuinchoNo ratings yet
- Cancer of The EsophagusDocument31 pagesCancer of The EsophagusBiway RegalaNo ratings yet
- MelanomaDocument162 pagesMelanomaximetorres31No ratings yet
- Brain Tumors: Jeselo Ouano GormeDocument13 pagesBrain Tumors: Jeselo Ouano GormeMaddox EdeyajNo ratings yet
- Journal Homepage: - : IntroductionDocument6 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- EdCaN Specialty Module 4Document23 pagesEdCaN Specialty Module 4cindy8127No ratings yet
- Testicular Cancer JUDocument10 pagesTesticular Cancer JUkarla QuinteroNo ratings yet
- Subungual MelanomaDocument50 pagesSubungual Melanomastefani83No ratings yet
- Adnexal Tumors of The SkinDocument6 pagesAdnexal Tumors of The SkinFaduahSalazarNo ratings yet
- Abnormal Pap Smear. K.C 2023Document71 pagesAbnormal Pap Smear. K.C 2023MLV AbayNo ratings yet