Download as pdf or txt
You might also like
- Bruce Ecker, Laurel Hulley - Depth Oriented Brief Therapy - How To Be Brief When You Were Trained To Be Deep and Vice Versa-Jossey-Bass (1995)Document306 pagesBruce Ecker, Laurel Hulley - Depth Oriented Brief Therapy - How To Be Brief When You Were Trained To Be Deep and Vice Versa-Jossey-Bass (1995)John Smith85% (13)
- PE11 - MELC 4 Module 4 - Week7 For Teacher PDFDocument24 pagesPE11 - MELC 4 Module 4 - Week7 For Teacher PDFRommel Cando80% (5)
- Pasi CalculatorDocument4 pagesPasi CalculatorBimo Aryo TejoNo ratings yet
- Protesis Fija Con Ataches. Rep Caso. 2020. Cureus. SivakumarDocument13 pagesProtesis Fija Con Ataches. Rep Caso. 2020. Cureus. SivakumarAngela AcostaNo ratings yet
- CASE REPORT Esthetic Prosthodontics: Case Reports: October 2019Document5 pagesCASE REPORT Esthetic Prosthodontics: Case Reports: October 2019Thio TiganaNo ratings yet
- Prosthodontic Rehabilitation of Residual Mandibular Defect With Fixed Removable Hybrid Prosthesis-A Case ReportDocument4 pagesProsthodontic Rehabilitation of Residual Mandibular Defect With Fixed Removable Hybrid Prosthesis-A Case ReportnastitiiNo ratings yet
- Jurnal ProsthoDocument5 pagesJurnal ProsthoFaiqotul KumalaNo ratings yet
- The Bio-Col TechniqueDocument9 pagesThe Bio-Col TechniquewnelsenNo ratings yet
- Tanpa Judul PDFDocument7 pagesTanpa Judul PDFnadyashintakasihNo ratings yet
- Fixed Prosthetic Implant Restoration of The Edentulous Maxilla A Systematic Pretreatment Evaluation Method - Jan - 2008Document11 pagesFixed Prosthetic Implant Restoration of The Edentulous Maxilla A Systematic Pretreatment Evaluation Method - Jan - 2008Nathawat PleumsamranNo ratings yet
- Management of A Subgingivally Fractured Central inDocument5 pagesManagement of A Subgingivally Fractured Central inayoubNo ratings yet
- 1 s2.0 S0278239107016424 MainDocument11 pages1 s2.0 S0278239107016424 MainDANTE DELEGUERYNo ratings yet
- Crown Lengthening in Mandibular Molars: A 5-Year Retrospective Radiographic AnalysisDocument7 pagesCrown Lengthening in Mandibular Molars: A 5-Year Retrospective Radiographic AnalysisbubuvulpeaNo ratings yet
- Avulsion and Replacement of The Tooth Element Fractured at The Level of The Middle A Case ReportDocument5 pagesAvulsion and Replacement of The Tooth Element Fractured at The Level of The Middle A Case ReportDr.O.R.GANESAMURTHINo ratings yet
- Successful Restoration of Severely Mutilated Primary Incisors Using A Novel Method To Retain Zirconia Crowns - Two Year ResultsDocument6 pagesSuccessful Restoration of Severely Mutilated Primary Incisors Using A Novel Method To Retain Zirconia Crowns - Two Year ResultsmartinfabyNo ratings yet
- Department of Pediatric & Preventive DentistryDocument3 pagesDepartment of Pediatric & Preventive DentistryRenieKumalaNo ratings yet
- IPIntJMedPaediatrOncol 9 2 77 82Document6 pagesIPIntJMedPaediatrOncol 9 2 77 82Laraduta AgustiniNo ratings yet
- Zona Neutra Maxilofacial PacienteDocument6 pagesZona Neutra Maxilofacial Pacientemargarita de montenegroNo ratings yet
- 2575 PDFDocument4 pages2575 PDFAkshayaa BalajiNo ratings yet
- Bone and Tissue LevelDocument3 pagesBone and Tissue LevelSaleh AlsadiNo ratings yet
- 6.clinical Case ReportMultidisciplinary Approach For Rehabilitation of Debilitated Anterior ToothDocument6 pages6.clinical Case ReportMultidisciplinary Approach For Rehabilitation of Debilitated Anterior ToothSahana RangarajanNo ratings yet
- Management of Fracture Tooth Fragment Reattachment: Case ReportDocument7 pagesManagement of Fracture Tooth Fragment Reattachment: Case Reportwaleed MagidNo ratings yet
- Enhanced Retention of A Maxillofacial Prosthetic Obturator Using Precision Attachments: Two Case ReportsDocument6 pagesEnhanced Retention of A Maxillofacial Prosthetic Obturator Using Precision Attachments: Two Case ReportsAmalorNo ratings yet
- Conservative Mangement of Tilted AbutmentsDocument3 pagesConservative Mangement of Tilted Abutmentsrayavarapu sunilNo ratings yet
- Buzatu Teodor Valentin Art 1 EngDocument6 pagesBuzatu Teodor Valentin Art 1 EngStefana ReveiNo ratings yet
- Badami 2011Document5 pagesBadami 2011ayoubNo ratings yet
- Article WMC004708 PDFDocument5 pagesArticle WMC004708 PDFAnonymous 2r6nHhNo ratings yet
- Full Mouth Rehabilitation Using Hobo Twin-Stage TechniqueDocument5 pagesFull Mouth Rehabilitation Using Hobo Twin-Stage TechniqueswagataNo ratings yet
- Tooth TtriyionDocument5 pagesTooth TtriyionDhanasriNo ratings yet
- Non Familiar Characterization Using A Loop Connection in A Fixed Partial DentureDocument3 pagesNon Familiar Characterization Using A Loop Connection in A Fixed Partial DentureAzzam SaqrNo ratings yet
- Restoration of Congenitally Missing Lateral Incisors After Orthodontic TreatmentDocument4 pagesRestoration of Congenitally Missing Lateral Incisors After Orthodontic Treatmentmarianaduque82No ratings yet
- Prosthodontic Management of Dentate Maxillectomy Patient A Clinical Case ReportActa Marisiensis Seria MedicaDocument4 pagesProsthodontic Management of Dentate Maxillectomy Patient A Clinical Case ReportActa Marisiensis Seria MedicaSaniaNo ratings yet
- Tooth-Support Over Dentures: An Approach To Preventive ProsthodonticsDocument5 pagesTooth-Support Over Dentures: An Approach To Preventive ProsthodonticsAdvanced Research PublicationsNo ratings yet
- Apiko 2Document7 pagesApiko 2Asri DamayantiNo ratings yet
- Awais AssignmentDocument3 pagesAwais AssignmentMuhammad AwaisNo ratings yet
- Malo ArticleDocument6 pagesMalo Articleishita parekhNo ratings yet
- Chair-Side Fabrication of A FixedDocument7 pagesChair-Side Fabrication of A FixedKataryne Dos SantosNo ratings yet
- Full Mouth Rehabilitation of A Patient With Ra PDFDocument3 pagesFull Mouth Rehabilitation of A Patient With Ra PDFdehaaNo ratings yet
- Tecnica de HallDocument4 pagesTecnica de HallYalile TurkaNo ratings yet
- Adj 12563Document5 pagesAdj 12563anushiNo ratings yet
- Konser PDFDocument3 pagesKonser PDFSuciNo ratings yet
- Provisional RestorationsDocument4 pagesProvisional RestorationsMyri Gebert SchererNo ratings yet
- Prosthetic Rehabilitation of Maxillectomy Patient With Telescopic DenturesDocument6 pagesProsthetic Rehabilitation of Maxillectomy Patient With Telescopic DenturesVero AngelNo ratings yet
- Functional and Aesthetic Full Mouth Rehabilitation of A Severely Worn Dentition To Restore Vertical Dimension: A Case ReportDocument5 pagesFunctional and Aesthetic Full Mouth Rehabilitation of A Severely Worn Dentition To Restore Vertical Dimension: A Case ReportammarkochiNo ratings yet
- Clinical Management of A Fractured Anterior Tooth With Reattachment Technique A Case Report With An 8-Year Follow UpDocument5 pagesClinical Management of A Fractured Anterior Tooth With Reattachment Technique A Case Report With An 8-Year Follow UpABDUSSALAMNo ratings yet
- Prosthetic Rehabilitation of Mandibular Defects With Fixed-Removable Partial Denture Prosthesis Using Precision Attachment - A Twin Case ReportDocument17 pagesProsthetic Rehabilitation of Mandibular Defects With Fixed-Removable Partial Denture Prosthesis Using Precision Attachment - A Twin Case ReportIvy MedNo ratings yet
- Idjsr 5 (1) 25-28Document4 pagesIdjsr 5 (1) 25-28Krupali JainNo ratings yet
- Recurrent Diastema Closure After Orthodontic Treatment With CeramicDocument4 pagesRecurrent Diastema Closure After Orthodontic Treatment With Ceramicyuana dnsNo ratings yet
- Rehabilitation of Sieberts Class III Defect Using Fixed Removable Prosthesis (Andrew's Bridge)Document5 pagesRehabilitation of Sieberts Class III Defect Using Fixed Removable Prosthesis (Andrew's Bridge)drgunNo ratings yet
- 1994 1524551201 PDFDocument4 pages1994 1524551201 PDFRizki AmeliaNo ratings yet
- Mermigos 11 01Document4 pagesMermigos 11 01Sankurnia HariwijayadiNo ratings yet
- Dramit007, Journal Manager, 13Document3 pagesDramit007, Journal Manager, 13KAREN VIVIANA ALVARADO HERNANDEZNo ratings yet
- Cantor and Curtis ClassificationDocument4 pagesCantor and Curtis ClassificationMuhammad AwaisNo ratings yet
- Full Mouth Rehabilitation With Implant-Supported Fixed Dental Prosthesis - 'An All-On-6 Clinical Report'Document6 pagesFull Mouth Rehabilitation With Implant-Supported Fixed Dental Prosthesis - 'An All-On-6 Clinical Report'sapnaNo ratings yet
- TMP 371 BDocument4 pagesTMP 371 BFrontiersNo ratings yet
- Rehabilitation of Hemimandibulectomy PatientDocument3 pagesRehabilitation of Hemimandibulectomy PatientAB MISHRANo ratings yet
- Masking Conventional Metallic Cast Post For Enhancing EstheticsDocument5 pagesMasking Conventional Metallic Cast Post For Enhancing EstheticsleilyanisariNo ratings yet
- Restoration in Gingival Recession PDFDocument4 pagesRestoration in Gingival Recession PDFannysaNo ratings yet
- AsdfaDocument4 pagesAsdfaFree PizzaNo ratings yet
- Aumento de Reborde 1Document4 pagesAumento de Reborde 1valeriaNo ratings yet
- Article 1Document7 pagesArticle 1Sabrina CHNo ratings yet
- Intaglio JPDDocument7 pagesIntaglio JPDEddie Ojeda HoffmannNo ratings yet
- 20 Years of Guided Bone Regeneration in Implant Dentistry: Second EditionFrom Everand20 Years of Guided Bone Regeneration in Implant Dentistry: Second EditionNo ratings yet
- Mandibular MovementDocument56 pagesMandibular MovementSahana RangarajanNo ratings yet
- Factors Affecting Shade of All Ceramic Restorations - A Literature ReviewDocument8 pagesFactors Affecting Shade of All Ceramic Restorations - A Literature ReviewSahana RangarajanNo ratings yet
- Dynamic Navigation in Dental Implantology: The Influence of Surgical Experience On Implant Placement Accuracy and Operating Time. An in Vitro StudyDocument9 pagesDynamic Navigation in Dental Implantology: The Influence of Surgical Experience On Implant Placement Accuracy and Operating Time. An in Vitro StudySahana RangarajanNo ratings yet
- Support in Complete DentureDocument16 pagesSupport in Complete DentureSahana RangarajanNo ratings yet
- Different Types of Tooth PreparationDocument56 pagesDifferent Types of Tooth PreparationSahana Rangarajan100% (1)
- Finishing and Polishing Agents: - Presented by DR Arpita DuttaDocument89 pagesFinishing and Polishing Agents: - Presented by DR Arpita DuttaSahana RangarajanNo ratings yet
- Support in Complete DentureDocument30 pagesSupport in Complete DentureSahana Rangarajan100% (2)
- Frankel Appliance Certified Fixed Orthodontic Courses by Indian Dental AcademyDocument76 pagesFrankel Appliance Certified Fixed Orthodontic Courses by Indian Dental AcademySahana RangarajanNo ratings yet
- Clinical Report Rehabilitation of Maxillary Surgical Defect With A Cast Partial Denture ObturatorDocument4 pagesClinical Report Rehabilitation of Maxillary Surgical Defect With A Cast Partial Denture ObturatorSahana RangarajanNo ratings yet
- A Hollow Bulb Obturator For Maxillary Resection in A Completely Edentulous PatientDocument6 pagesA Hollow Bulb Obturator For Maxillary Resection in A Completely Edentulous PatientSahana RangarajanNo ratings yet
- 6.clinical Case ReportMultidisciplinary Approach For Rehabilitation of Debilitated Anterior ToothDocument6 pages6.clinical Case ReportMultidisciplinary Approach For Rehabilitation of Debilitated Anterior ToothSahana RangarajanNo ratings yet
- 3D Printing Industry Roadmap - India (Aerospace) Summit DocumentDocument19 pages3D Printing Industry Roadmap - India (Aerospace) Summit DocumentSahana RangarajanNo ratings yet
- 7 Shreeprada Dash IJPHRDDecember 2018 IssueDocument7 pages7 Shreeprada Dash IJPHRDDecember 2018 IssueSahana RangarajanNo ratings yet
- Mouth Guards in Dentistry-A Review: September 2018Document6 pagesMouth Guards in Dentistry-A Review: September 2018Sahana RangarajanNo ratings yet
- Long-Term Follow-Up of Maxillary Fixed Retention: Survival Rate and Periodontal HealthDocument7 pagesLong-Term Follow-Up of Maxillary Fixed Retention: Survival Rate and Periodontal HealthSahana RangarajanNo ratings yet
- Review: Types of Finish Lines or Gingival Margins Intooth PreparationDocument6 pagesReview: Types of Finish Lines or Gingival Margins Intooth PreparationSahana RangarajanNo ratings yet
- 7 RetainerinorthodonticsDocument6 pages7 RetainerinorthodonticsSahana RangarajanNo ratings yet
- Elegant Galaxy Background Breakthrough by SlidesgoDocument48 pagesElegant Galaxy Background Breakthrough by SlidesgoSahana RangarajanNo ratings yet
- Significance of Facebow For Dental RestorationsDocument5 pagesSignificance of Facebow For Dental RestorationsSahana RangarajanNo ratings yet
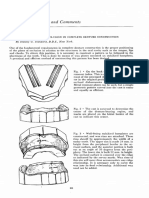
- Cases and Comments: by Stanley G. Standard, D.D.S., New YorkDocument3 pagesCases and Comments: by Stanley G. Standard, D.D.S., New YorkSahana RangarajanNo ratings yet
- Sauser 1957Document9 pagesSauser 1957Sahana RangarajanNo ratings yet
- Prosthodontics Horizontal Jaw Relation: Dr. Firas AbdulameerDocument6 pagesProsthodontics Horizontal Jaw Relation: Dr. Firas AbdulameerSahana RangarajanNo ratings yet
- Gothic Arch TrachingDocument7 pagesGothic Arch TrachingSahana RangarajanNo ratings yet
- Alcohal DependenceDocument17 pagesAlcohal DependenceViky SinghNo ratings yet
- National Program For Rehabilitation of Polluted Site - A Case StudyDocument4 pagesNational Program For Rehabilitation of Polluted Site - A Case StudyijeteeditorNo ratings yet
- IELTS Cause-Problem and Effect-Solution Model EssayDocument17 pagesIELTS Cause-Problem and Effect-Solution Model EssaySayaf RashadNo ratings yet
- Tapentadol ThiocholchicosideDocument2 pagesTapentadol ThiocholchicosideMohammad Shahbaz Alam100% (1)
- 3340-Sds-Petromin Atf Dexron Ii e V#2Document6 pages3340-Sds-Petromin Atf Dexron Ii e V#2SICIM SAUDI ARABIANo ratings yet
- Main AmbaniDocument28 pagesMain AmbaniankursagarNo ratings yet
- ComplaintDocument52 pagesComplaintmarwaNo ratings yet
- A170566 Study Report BodyDocument79 pagesA170566 Study Report BodyAnonymous yqRB5cVMeNo ratings yet
- HypothermiaDocument5 pagesHypothermiaMRS CHAKRAPANINo ratings yet
- PREGNANCYDocument4 pagesPREGNANCYShaileeNo ratings yet
- One Health Concepts and Knowledge Presentation SlidesDocument48 pagesOne Health Concepts and Knowledge Presentation Slideskarunia nihaya100% (1)
- One Minute Push Up TestDocument5 pagesOne Minute Push Up Testayieeeee03No ratings yet
- Humanitarians in The Face of Atrocities: Case Studies: Syria and CARDocument19 pagesHumanitarians in The Face of Atrocities: Case Studies: Syria and CARMigs MontrealNo ratings yet
- Oxygen Therapy AdviceDocument38 pagesOxygen Therapy Advicenick_clayton_9No ratings yet
- Combination AntibioticsDocument36 pagesCombination AntibioticsAamir BugtiNo ratings yet
- Department of Labor: Bct-Fy01Document101 pagesDepartment of Labor: Bct-Fy01USA_DepartmentOfLabor100% (1)
- Omonigbehin Emmanuel AdedayoDocument12 pagesOmonigbehin Emmanuel AdedayoAriel GhieNo ratings yet
- The Effects of Trauma and How To Deal With It Jim BanksDocument5 pagesThe Effects of Trauma and How To Deal With It Jim Banks2bug2me2not2No ratings yet
- Rose Doe v. The City of New York, Et. Al.Document57 pagesRose Doe v. The City of New York, Et. Al.Daily Caller News FoundationNo ratings yet
- Passenger Locator Form: Non-Red ListDocument4 pagesPassenger Locator Form: Non-Red ListSamadrukNo ratings yet
- Clamoxin 156-25mg Suspension (Amoxicillin and Clavulanate Potassium)Document5 pagesClamoxin 156-25mg Suspension (Amoxicillin and Clavulanate Potassium)rizwan900No ratings yet
- PHENYLKETONURIADocument3 pagesPHENYLKETONURIAMiwa IshiiNo ratings yet
- Substance AbuseDocument54 pagesSubstance AbuseCharles CastilloNo ratings yet
- Post Partum Psychosis Nursing Diagnosis: Aurelio, Lyca Mae MDocument3 pagesPost Partum Psychosis Nursing Diagnosis: Aurelio, Lyca Mae MLyca Mae AurelioNo ratings yet
- Construction Site Management ChecklistDocument6 pagesConstruction Site Management ChecklistAbdulaziz IbrahimNo ratings yet
- Written Report Abnormal PsychologyDocument23 pagesWritten Report Abnormal PsychologyCy Esquibel LingaNo ratings yet
- Green Light Surgical GuideDocument88 pagesGreen Light Surgical GuidekbrinaldiNo ratings yet