Download as pdf or txt
You might also like
- Claims Management Policy TemplateDocument2 pagesClaims Management Policy TemplateSharif Fayiz AbushaikhaNo ratings yet
- Acute Effects of The Voodoo Flossing Band On Ankle Range of Motion - Philip Stevenson 2019Document10 pagesAcute Effects of The Voodoo Flossing Band On Ankle Range of Motion - Philip Stevenson 2019YngaMarquezJairNo ratings yet
- C-88 - An Additional Amendment To My Basis of Claim FormDocument19 pagesC-88 - An Additional Amendment To My Basis of Claim FormVéronique BellamyNo ratings yet
- DBT Visual Review Flash CardDocument14 pagesDBT Visual Review Flash CardBeyza Gül89% (9)
- Physical Therapy in Sport: Seth O'Neill, Simon Barry, Paul WatsonDocument8 pagesPhysical Therapy in Sport: Seth O'Neill, Simon Barry, Paul WatsonmorbreirNo ratings yet
- Alterations in Mechanical Properties of The Patellar Tendon Is Associated With Pain in Athletes With Patellar TendinopathyDocument7 pagesAlterations in Mechanical Properties of The Patellar Tendon Is Associated With Pain in Athletes With Patellar TendinopathyIsrael Oña CisnerosNo ratings yet
- Acta Orthopaedica: Please Scroll Down For ArticleDocument4 pagesActa Orthopaedica: Please Scroll Down For ArticleRicardo FerreiraNo ratings yet
- Ankle Stabilization With Arthroscopic Versus Open With Suture Tape Augmentation Techniques X1D XJ. George DeVries PDFDocument5 pagesAnkle Stabilization With Arthroscopic Versus Open With Suture Tape Augmentation Techniques X1D XJ. George DeVries PDFcrpcsxfdkgNo ratings yet
- Effects of Distally Fixated Versus Nondistally Fixated Leg Extensor Resistance Training On Knee Pain in The Early Period After Anterior Cruciate Ligament ReconstructionDocument9 pagesEffects of Distally Fixated Versus Nondistally Fixated Leg Extensor Resistance Training On Knee Pain in The Early Period After Anterior Cruciate Ligament ReconstructionMirna Vasquez MacayaNo ratings yet
- Evaluation Kinaesthetic Proprioceptive Deficit After Knee Anterior Cruciate Ligament (ACL) Reconstruction in AthletesDocument7 pagesEvaluation Kinaesthetic Proprioceptive Deficit After Knee Anterior Cruciate Ligament (ACL) Reconstruction in AthletesAndy Delos ReyesNo ratings yet
- FulltextDocument6 pagesFulltextdespNo ratings yet
- To Rry EffusionDocument14 pagesTo Rry EffusionLINANo ratings yet
- Evidence-Based Treatment Choices For Acute Lateral Ankle Sprain: A Comprehensive Systematic ReviewDocument9 pagesEvidence-Based Treatment Choices For Acute Lateral Ankle Sprain: A Comprehensive Systematic ReviewMilton RezzaNo ratings yet
- The Effect of Different Decline Angles On The Biomechanics of Double Limb Squats and The Implications To Clinical and Training PracticeDocument15 pagesThe Effect of Different Decline Angles On The Biomechanics of Double Limb Squats and The Implications To Clinical and Training Practicesebastian floresNo ratings yet
- 1 s2.0 S0929664619300567 MainDocument8 pages1 s2.0 S0929664619300567 Mainananta restyNo ratings yet
- 264 2013 Article 2112Document6 pages264 2013 Article 2112Anil KumarNo ratings yet
- The Modified Brostr M Gould Procedure - Early Results Usi - 2014 - Foot and AnklDocument5 pagesThe Modified Brostr M Gould Procedure - Early Results Usi - 2014 - Foot and AnklFyodorovich Makarov NikolaiNo ratings yet
- 45 Achilles Tendon Rupt 2018 Clinical Orthopaedic Rehabilitation A Team ADocument5 pages45 Achilles Tendon Rupt 2018 Clinical Orthopaedic Rehabilitation A Team AJessica HongNo ratings yet
- Jain 2013Document15 pagesJain 2013Mohan DesaiNo ratings yet
- Paper MAI FootDocument10 pagesPaper MAI Foothareem7bilalNo ratings yet
- McNeill & Pedersen 2016. Dynamic Tape. Is It All About Controlling LoadDocument10 pagesMcNeill & Pedersen 2016. Dynamic Tape. Is It All About Controlling Loaddaniel QuinteroNo ratings yet
- 53 - Changes in Arthroscopic Findings in The Anterior Cruciate Ligament Deficient Knee Prior To Reconstructive SurgeryDocument3 pages53 - Changes in Arthroscopic Findings in The Anterior Cruciate Ligament Deficient Knee Prior To Reconstructive SurgeryrandocalNo ratings yet
- BBRC Vol 14 No 04 2021-80Document5 pagesBBRC Vol 14 No 04 2021-80Dr Sharique AliNo ratings yet
- Art:10.1186/1756 0500 7 569Document6 pagesArt:10.1186/1756 0500 7 569Fuioaga Codrin-PaulNo ratings yet
- Graston TechniqueDocument8 pagesGraston TechniqueSvetlana PolyakovaNo ratings yet
- Volpin 2017Document8 pagesVolpin 2017Yogeshwar SinghNo ratings yet
- Eliasson 2018Document11 pagesEliasson 2018seriesediversosNo ratings yet
- International Society For Technology in Arthroplasty - Indicação de ArtigosDocument77 pagesInternational Society For Technology in Arthroplasty - Indicação de ArtigosJosé santanaNo ratings yet
- Predictors of Chronic Ankle InstabilityDocument6 pagesPredictors of Chronic Ankle InstabilityLeydi LondoñoNo ratings yet
- Patelofemoral MedialDocument9 pagesPatelofemoral MedialRe DiazNo ratings yet
- Comparative Study of Posterior Stabilizing VS Cruciate Retaining Prosthesis in Total Knee ReplacementDocument15 pagesComparative Study of Posterior Stabilizing VS Cruciate Retaining Prosthesis in Total Knee ReplacementIJAR JOURNALNo ratings yet
- Esguince de Codo 2Document10 pagesEsguince de Codo 2ansantiago.mendezzNo ratings yet
- The Effect of Kinesio® Tape On Vertical Jump and Dynamic Postural ControlDocument14 pagesThe Effect of Kinesio® Tape On Vertical Jump and Dynamic Postural ControlFrancisco Javier Luza RamosNo ratings yet
- Balance Awareness and Kinesio Taping of The Ankle: David K. GarciaDocument4 pagesBalance Awareness and Kinesio Taping of The Ankle: David K. GarciaAna Lu LoboNo ratings yet
- Prior Knee ArthrosDocument5 pagesPrior Knee ArthrosMaría Fernanda LópezNo ratings yet
- Adductor Magnus An EMG Investigation Into Proximal and Disctal Portions and Direction Specific ActionDocument9 pagesAdductor Magnus An EMG Investigation Into Proximal and Disctal Portions and Direction Specific ActionElaine CspNo ratings yet
- Ankle Arthrodesis For Pilon FractureDocument12 pagesAnkle Arthrodesis For Pilon FracturestudmmaNo ratings yet
- Resection Arthroplasty of The Sternoclavicular Joint: J Bone Joint Surg AmDocument8 pagesResection Arthroplasty of The Sternoclavicular Joint: J Bone Joint Surg AmPersonil MonkthreeysNo ratings yet
- Slight Femoral Under-Correction Versus Neutral Alignment in Total Knee Arthroplasty With Preoperative Varus Knees: A Comparative StudyDocument8 pagesSlight Femoral Under-Correction Versus Neutral Alignment in Total Knee Arthroplasty With Preoperative Varus Knees: A Comparative Studyfebyan yohanesNo ratings yet
- Elbow Joint Loads During Simulated Activities of DDocument11 pagesElbow Joint Loads During Simulated Activities of DJoe ANo ratings yet
- Bulut 2018Document5 pagesBulut 2018José Luis Velasquez UrregoNo ratings yet
- Schuh 2011Document8 pagesSchuh 2011Francisco Castillo VázquezNo ratings yet
- The Study To Assess The Effect of Prehabilitation On Postoperative Outcome of The Patients On Total Knee Arthroplasty at Selected HospitalDocument4 pagesThe Study To Assess The Effect of Prehabilitation On Postoperative Outcome of The Patients On Total Knee Arthroplasty at Selected HospitalEditor IJTSRDNo ratings yet
- Immobilization in External RotationDocument9 pagesImmobilization in External RotationSylvia DamayantiNo ratings yet
- Integrated Review WeeblyDocument10 pagesIntegrated Review Weeblyapi-401390929No ratings yet
- HombroDocument10 pagesHombroDr. AlonsoNo ratings yet
- Aspiration and Injection of The Knee Joint: Approach Portal: Review ArticleDocument6 pagesAspiration and Injection of The Knee Joint: Approach Portal: Review ArticleLindaespGarciaNo ratings yet
- Prosthet Orthot Int 2002 Sjödahl 101 12Document13 pagesProsthet Orthot Int 2002 Sjödahl 101 12Jorge Eduardo Jiménez SimpsonsNo ratings yet
- Journal of Orthopaedics: Dominic T. Mathis, Leif Lohrer, Felix Amsler, Michael T. HirschmannDocument7 pagesJournal of Orthopaedics: Dominic T. Mathis, Leif Lohrer, Felix Amsler, Michael T. HirschmannDita AldiniNo ratings yet
- N Lower Limb Amputation Following Trauma2011Document6 pagesN Lower Limb Amputation Following Trauma2011IMSS LomasverdesNo ratings yet
- Partial-Thickness Articular Surface Rotator Cuff Tears: An All-Inside Repair TechniqueDocument7 pagesPartial-Thickness Articular Surface Rotator Cuff Tears: An All-Inside Repair TechniqueCsiszar AporNo ratings yet
- Full TextDocument9 pagesFull TextdespNo ratings yet
- Heel Pain Plantar Fascitis Hard Vs Sorft Orthotics and Heels PadDocument11 pagesHeel Pain Plantar Fascitis Hard Vs Sorft Orthotics and Heels PadDik 40No ratings yet
- 1 s2.0 S1466853X16302139 MainDocument5 pages1 s2.0 S1466853X16302139 MainMiguel de Caso VillarroelNo ratings yet
- Flexion Contracture Following Primary TKA Risk Factors and OutcomesDocument5 pagesFlexion Contracture Following Primary TKA Risk Factors and OutcomesAdi WesnawaNo ratings yet
- Assessment of Postural Stability in Patients With A TranstibialDocument9 pagesAssessment of Postural Stability in Patients With A TranstibialTarushi TanwarNo ratings yet
- Effective Use of Viscosupplementation After Knee Arthroscopy: Experience From A Working GroupDocument10 pagesEffective Use of Viscosupplementation After Knee Arthroscopy: Experience From A Working GroupIJAR JOURNALNo ratings yet
- Manual Therapy: Original ArticleDocument5 pagesManual Therapy: Original ArticleCleber PimentaNo ratings yet
- Andrews Arthroplasty 06Document18 pagesAndrews Arthroplasty 06Sagar SharmaNo ratings yet
- Abat 2016Document8 pagesAbat 2016toaldoNo ratings yet
- Daigeler 2009Document8 pagesDaigeler 2009Javier JonesNo ratings yet
- Region Specific Patellar Tendon Hypertrophy in Humans Following Resistance TrainingDocument11 pagesRegion Specific Patellar Tendon Hypertrophy in Humans Following Resistance TrainingRosaneLacerdaNo ratings yet
- Cartilage Injury of the Knee: State-of-the-Art Treatment and ControversiesFrom EverandCartilage Injury of the Knee: State-of-the-Art Treatment and ControversiesAaron J. KrychNo ratings yet
- Chemistry ProjectDocument12 pagesChemistry ProjectShubham AgrawalNo ratings yet
- KanadDocument3 pagesKanadShubham AgrawalNo ratings yet
- SEARCH ENGINES-research PaperDocument2 pagesSEARCH ENGINES-research PaperShubham AgrawalNo ratings yet
- Name:-Lisa Bajaj Registration No.: - 11617461 Roll No.: - A21Document5 pagesName:-Lisa Bajaj Registration No.: - 11617461 Roll No.: - A21Shubham AgrawalNo ratings yet
- Reactive Power Problems and System: Submitted By:-Section: - Roll No: - SubjectDocument16 pagesReactive Power Problems and System: Submitted By:-Section: - Roll No: - SubjectShubham AgrawalNo ratings yet
- A1989472039 17688 4 2019 ProjectDocument1 pageA1989472039 17688 4 2019 ProjectShubham AgrawalNo ratings yet
- Purchage: Yes NoDocument1 pagePurchage: Yes NoShubham AgrawalNo ratings yet
- PARENT AWARENESS SEMINAR-hand OutsDocument2 pagesPARENT AWARENESS SEMINAR-hand OutsLADY ANN GRACE LAGASNo ratings yet
- Class 12 Physical Education Half-Yearly Paper 2021-22Document15 pagesClass 12 Physical Education Half-Yearly Paper 2021-22Gamer ZoneNo ratings yet
- 0610 - s17 - QP - 42 AnsweredDocument20 pages0610 - s17 - QP - 42 Answered-Bleh- WalkerNo ratings yet
- MindfulnessDocument30 pagesMindfulnessYetro ValentinoNo ratings yet
- DessyDocument5 pagesDessyYenita sariNo ratings yet
- Chapter 3 CaregiversDocument20 pagesChapter 3 CaregiversJuanNo ratings yet
- PB Nuflow REV03Document2 pagesPB Nuflow REV03metech8xNo ratings yet
- Sansulin R Suspensi Injeksi 100 IU, ML - Rekombinan Insulin Manusia - DKI0708100443A1 - 2016Document2 pagesSansulin R Suspensi Injeksi 100 IU, ML - Rekombinan Insulin Manusia - DKI0708100443A1 - 2016Yessi VirginiaNo ratings yet
- 2020 Tanzania in FiguresDocument110 pages2020 Tanzania in FiguresDaveNo ratings yet
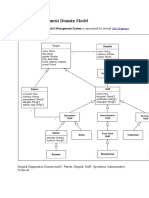
- Hospital Management Domain ModelDocument4 pagesHospital Management Domain Modelvinod kapateNo ratings yet
- Drug Book On EmergencyDocument21 pagesDrug Book On EmergencyDimpal Choudhary100% (4)
- ISMT 12 - Day 402 - Rita - Posterior Cervical Laminectomy and Fusion Surgery C3-C7Document21 pagesISMT 12 - Day 402 - Rita - Posterior Cervical Laminectomy and Fusion Surgery C3-C7Vito MasagusNo ratings yet
- 升降机说明书 (新式升降机)英文SC200200Document49 pages升降机说明书 (新式升降机)英文SC200200Victor LeãoNo ratings yet
- De Thi Thu THPT Quoc Gia 2022 Mon Tieng Anh Truong THPT Tran Phu Lan 1Document10 pagesDe Thi Thu THPT Quoc Gia 2022 Mon Tieng Anh Truong THPT Tran Phu Lan 1Ngọc TrầnNo ratings yet
- BDSM As Trauma PlayDocument17 pagesBDSM As Trauma Playaeiman zazNo ratings yet
- Shell Omala S2 G 320: Performance, Features & BenefitsDocument3 pagesShell Omala S2 G 320: Performance, Features & BenefitsVelibor KaranovicNo ratings yet
- $1-5 Donations Benefits - Medical Study ZoneDocument63 pages$1-5 Donations Benefits - Medical Study ZoneVishal KumarNo ratings yet
- Lace Flames The Kimberly Chronicles Book One Lainey Reese Full ChapterDocument51 pagesLace Flames The Kimberly Chronicles Book One Lainey Reese Full Chapterlinda.walsh847100% (10)
- AAOSub2017 - RET SyllabusDocument217 pagesAAOSub2017 - RET SyllabusYasminSolbergNo ratings yet
- Stress Management Case Study SubmissionDocument4 pagesStress Management Case Study Submissionapi-571240870No ratings yet
- Albert Lea Tribune 08172022 E-EditionDocument16 pagesAlbert Lea Tribune 08172022 E-EditionSarah StultzNo ratings yet
- Birthday Party - Character SketchesDocument2 pagesBirthday Party - Character SketchesDhivyaNo ratings yet
- Total Number of Prepators: Earthstar Geographics Sio, © 2022 Tomtom, © 2022 Microsoft CorporationDocument4 pagesTotal Number of Prepators: Earthstar Geographics Sio, © 2022 Tomtom, © 2022 Microsoft Corporationsushain koulNo ratings yet
- Product: A Product Is Anything That Can Be Offered To A Market To Satisfy A Want or NeedDocument12 pagesProduct: A Product Is Anything That Can Be Offered To A Market To Satisfy A Want or NeedSumon Das DasNo ratings yet
- Hospital: ServicesDocument60 pagesHospital: ServicesChanpreet SinghNo ratings yet
- Corrective Action Plan Template 01Document2 pagesCorrective Action Plan Template 01sarge18No ratings yet
- Edu 422 NotesDocument13 pagesEdu 422 NotesAbdulazeez AishatNo ratings yet