
4.3 Peritonitis (Lecture-Based)
4.3 Peritonitis (Lecture-Based)
You might also like
- 4.4 Acute AbdomenDocument6 pages4.4 Acute AbdomenMiguel C. Dolot100% (1)
- A Grinchmas CarolDocument5 pagesA Grinchmas CarolMikey VultaggioNo ratings yet
- Peritonitis: Update On Pathophysiology, Clinical Manifestations, and ManagementDocument11 pagesPeritonitis: Update On Pathophysiology, Clinical Manifestations, and ManagementMuhamad Chairul SyahNo ratings yet
- Peritonitis: Update On Pathophysiology, Clinical Manifestations, and ManagementDocument11 pagesPeritonitis: Update On Pathophysiology, Clinical Manifestations, and ManagementerikafebriyanarNo ratings yet
- Peritonitis Update On Pathophysiology, Clinical Manifestations, and PDFDocument11 pagesPeritonitis Update On Pathophysiology, Clinical Manifestations, and PDFAnonymous InJS6aYZ100% (1)
- Leture 7 Infection in IcuDocument93 pagesLeture 7 Infection in IcuVincent Jofette AventunaNo ratings yet
- PeritonitisDocument78 pagesPeritonitisTan Dan100% (1)
- 1.3 PeritonitisDocument14 pages1.3 PeritonitisΜατθαίος ΠαππάςNo ratings yet
- Intra-Abdominal and Pelvic EmergenciesDocument21 pagesIntra-Abdominal and Pelvic Emergenciesqhrn48psvwNo ratings yet
- Management of Intra-Abdominal InfectionDocument65 pagesManagement of Intra-Abdominal InfectionKamran SherazNo ratings yet
- Sonographic Detection of Enlarged Mesenteric Lymph Nodes in Children and Its SignificanceDocument15 pagesSonographic Detection of Enlarged Mesenteric Lymph Nodes in Children and Its SignificanceInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- L09 - Diseases of The PeritoneumDocument13 pagesL09 - Diseases of The PeritoneumS sNo ratings yet
- Session 6Document72 pagesSession 6Alliah Marie CababarosNo ratings yet
- La Fasciite Nécrosante Sur Site D InjectionDocument6 pagesLa Fasciite Nécrosante Sur Site D InjectionDr ZarhouniNo ratings yet
- Peritonitis PDFDocument4 pagesPeritonitis PDFAndreas TheoNo ratings yet
- Fistulas Enterocutaneas MaingotDocument20 pagesFistulas Enterocutaneas MaingotroyvillafrancaNo ratings yet
- RETROPERITONEALDocument3 pagesRETROPERITONEALmichelleNo ratings yet
- 06 Peritonitis. Acute General Purulent and Encapsulated PeritonitisesDocument45 pages06 Peritonitis. Acute General Purulent and Encapsulated PeritonitisesFikri HaqNo ratings yet
- Siu Empiric Antibiotics For Select InfectionsDocument30 pagesSiu Empiric Antibiotics For Select InfectionspasswordNo ratings yet
- Penanganan Sepsis PitDocument43 pagesPenanganan Sepsis PitElfa RiniNo ratings yet
- AppendicitisDocument17 pagesAppendicitisalwinNo ratings yet
- Lower Genital Tract InfectionsDocument70 pagesLower Genital Tract InfectionsAbegail IbañezNo ratings yet
- PeritonitissDocument46 pagesPeritonitissNinaNo ratings yet
- Patofisiologi, Manifestasi Klinik, Dan Manajemen PeritonitisDocument11 pagesPatofisiologi, Manifestasi Klinik, Dan Manajemen Peritonitistika tikaNo ratings yet
- PeritonitisDocument34 pagesPeritonitisabrar_zaidiNo ratings yet
- Journal PeritonitisDocument7 pagesJournal PeritonitisEudia SiagianNo ratings yet
- Rotar O.V. As - Prof. General Surgery, BSMUDocument63 pagesRotar O.V. As - Prof. General Surgery, BSMUOleksandr RotarNo ratings yet
- Necrotising Fascitis: Recent Advances in Surgery 39Th EditionDocument36 pagesNecrotising Fascitis: Recent Advances in Surgery 39Th EditionPraveen CpNo ratings yet
- SEPSIS Incomplete-NotesDocument4 pagesSEPSIS Incomplete-NotesbmiakhylaellaineNo ratings yet
- Lap Pelvic DrainageDocument9 pagesLap Pelvic DrainageMuneer KhalamNo ratings yet
- PERITONITISDocument4 pagesPERITONITISAmoroso, Marian Corneth D.No ratings yet
- Peritonitis: Dr. Mahmoud Al-AwayshehDocument35 pagesPeritonitis: Dr. Mahmoud Al-Awayshehraed faisalNo ratings yet
- Fournier'S Gangrene: Rajah Amina SuleimanDocument27 pagesFournier'S Gangrene: Rajah Amina SuleimanAmina RajahNo ratings yet
- Afecciones Anorrectales Benignas Absceso Perianal, Fístula Anal, Hemorroides, Fisuras y Seno PilonidalDocument7 pagesAfecciones Anorrectales Benignas Absceso Perianal, Fístula Anal, Hemorroides, Fisuras y Seno PilonidalJoshua MaciasNo ratings yet
- Circulatory System Infectious Diseases: Dengue Hemorrhagic Shock SyndromeDocument3 pagesCirculatory System Infectious Diseases: Dengue Hemorrhagic Shock Syndromegrazelantonette.calubNo ratings yet
- Abdominal Tuberculosi S: DR - Prateek Kumar Junior ResidentDocument68 pagesAbdominal Tuberculosi S: DR - Prateek Kumar Junior ResidentututelNo ratings yet
- Typhoid Enteric Fever From UiA Volume 32 Final WebDocument4 pagesTyphoid Enteric Fever From UiA Volume 32 Final WebJayesh KumarNo ratings yet
- 72 Ventilator Associated Pneumonia PDFDocument5 pages72 Ventilator Associated Pneumonia PDFV RakeshreddyNo ratings yet
- Peritonitis and AppendicitisDocument35 pagesPeritonitis and AppendicitisRose Anne AbivaNo ratings yet
- Pleural EffusionDocument3 pagesPleural EffusionAubrey PerezNo ratings yet
- Metritis With Pelvic CellulitisDocument2 pagesMetritis With Pelvic CellulitisCleoGomezNo ratings yet
- SECTION I Inflammatory, Infective, and Congenital: Pyogenic Liver AbscessDocument12 pagesSECTION I Inflammatory, Infective, and Congenital: Pyogenic Liver AbscessandresNo ratings yet
- Surgical Infection 1Document120 pagesSurgical Infection 1Liezel Dejumo BartolataNo ratings yet
- Peritonitis 1Document6 pagesPeritonitis 1m.rizoniakmalNo ratings yet
- F01ddiabrtes and InfectionDocument82 pagesF01ddiabrtes and InfectionAbdel-razek ElmelegiNo ratings yet
- Aspects of Nursing in The Control and Prevention of Peritoneal Dialysis InfectionsDocument27 pagesAspects of Nursing in The Control and Prevention of Peritoneal Dialysis InfectionsNanang AdhoniNo ratings yet
- Urinary Tract and Male Genital SystemDocument5 pagesUrinary Tract and Male Genital SystemMonicaNo ratings yet
- Empyema - Rol of SurgeonDocument5 pagesEmpyema - Rol of Surgeondantheman123No ratings yet
- (Surg2-Trans) 4.01 AppendixDocument7 pages(Surg2-Trans) 4.01 AppendixJake Brandon M. Andal, RNDNo ratings yet
- PeritonitisDocument15 pagesPeritonitiscgqphqdrytNo ratings yet
- Disorders of The Pleura: Pleural EffusionDocument42 pagesDisorders of The Pleura: Pleural EffusionIrma NurainiNo ratings yet
- Block 3.3 Sesi 3 Pathology of Urinary Tract: by Asdos 2011: Vetta Awe Eric Lily Fiko Ghana Ikal Linda May FahmiDocument96 pagesBlock 3.3 Sesi 3 Pathology of Urinary Tract: by Asdos 2011: Vetta Awe Eric Lily Fiko Ghana Ikal Linda May Fahmimail junkNo ratings yet
- Jurnal 8Document24 pagesJurnal 8agus indrawanNo ratings yet
- MPDFDocument11 pagesMPDFKeljang MoktanNo ratings yet
- 338 Typhoid Enteric FeverDocument6 pages338 Typhoid Enteric FeverSurbhi ThakurNo ratings yet
- Pneumonia PresentationDocument23 pagesPneumonia Presentationapi-546694141No ratings yet
- Acutel AppendicitisDocument8 pagesAcutel Appendicitislogamarquell17No ratings yet
- ASOMDocument41 pagesASOMArunkumar S KumarNo ratings yet
- Absceso Hepatico HarrisonDocument2 pagesAbsceso Hepatico HarrisonZafiss ChaconNo ratings yet
- Fast Facts: Complex Perianal Fistulas in Crohn's Disease: A multidisciplinary approach to a clinical challengeFrom EverandFast Facts: Complex Perianal Fistulas in Crohn's Disease: A multidisciplinary approach to a clinical challengeNo ratings yet
- Urinary Tract Infection in Children - Classification, Diagnosis and TreatmentFrom EverandUrinary Tract Infection in Children - Classification, Diagnosis and TreatmentNo ratings yet
- Nucleotide MetabolismDocument17 pagesNucleotide MetabolismMiguel C. DolotNo ratings yet
- 4.2 Abdominal Wall Hernia (Jerome Villacorta's Conflicted Copy 2014-03-22)Document7 pages4.2 Abdominal Wall Hernia (Jerome Villacorta's Conflicted Copy 2014-03-22)Miguel C. DolotNo ratings yet
- Shoulder Dystocia: Ina S. Irabon, MD, Fpogs, FPSRM, FpsgeDocument25 pagesShoulder Dystocia: Ina S. Irabon, MD, Fpogs, FPSRM, FpsgeMiguel C. DolotNo ratings yet
- 02.03-03 CNS II - Skeletal Muscle RelaxantsDocument7 pages02.03-03 CNS II - Skeletal Muscle RelaxantsMiguel C. DolotNo ratings yet
- Diabetes Mellitus 1Document47 pagesDiabetes Mellitus 1Miguel C. DolotNo ratings yet
- Basic Neuro-Ophthalmology: Common Problems SeenDocument6 pagesBasic Neuro-Ophthalmology: Common Problems SeenMiguel C. DolotNo ratings yet
- Cornea and External DiseasesDocument18 pagesCornea and External DiseasesMiguel C. DolotNo ratings yet
- Basic Ocular Surgeries: Fatima Medical Center Dr. Vicente O. Santos JR., MDDocument53 pagesBasic Ocular Surgeries: Fatima Medical Center Dr. Vicente O. Santos JR., MDMiguel C. DolotNo ratings yet
- 02.01-04 CNS I - AntiepilepticsDocument10 pages02.01-04 CNS I - AntiepilepticsMiguel C. DolotNo ratings yet
- Angeline D. Alabastro, M.D.: CNS Pharmacology I: AntiepilepticsDocument10 pagesAngeline D. Alabastro, M.D.: CNS Pharmacology I: AntiepilepticsMiguel C. DolotNo ratings yet
- 02.03-02 CNS II - Local AnesthesiaDocument5 pages02.03-02 CNS II - Local AnesthesiaMiguel C. DolotNo ratings yet
- 02.03-01 CNS II - General AnesthesiaDocument9 pages02.03-01 CNS II - General AnesthesiaMiguel C. DolotNo ratings yet
- 02.01-03 CNS I - AlcoholsDocument5 pages02.01-03 CNS I - AlcoholsMiguel C. DolotNo ratings yet
- 02.05. Patient-Doctor Relationship and Interviewing TechniquesDocument10 pages02.05. Patient-Doctor Relationship and Interviewing TechniquesMiguel C. DolotNo ratings yet
- Angeline D. Alabastro, M.D. Angeline D. Alabastro, M.D. Angeline D. Alabastro, M.DDocument7 pagesAngeline D. Alabastro, M.D. Angeline D. Alabastro, M.D. Angeline D. Alabastro, M.DMiguel C. DolotNo ratings yet
- 02.04. Physical Examination and Laboratory Tests in PsychiatryDocument12 pages02.04. Physical Examination and Laboratory Tests in PsychiatryMiguel C. DolotNo ratings yet
- 02.01-01 CNS I - Central NeurotransmittersDocument3 pages02.01-01 CNS I - Central NeurotransmittersMiguel C. DolotNo ratings yet
- Psychiatric History: Doc Los BañosDocument6 pagesPsychiatric History: Doc Los BañosMiguel C. DolotNo ratings yet
- Los Baños: Mental Status ExamDocument5 pagesLos Baños: Mental Status ExamMiguel C. DolotNo ratings yet
- Aminoglycoside Dosing GuidelinesDocument3 pagesAminoglycoside Dosing GuidelinesaeromintNo ratings yet
- PE (General and Head Neck)Document14 pagesPE (General and Head Neck)antomiolam1218No ratings yet
- Patient Medication ProfileDocument4 pagesPatient Medication ProfileLaura HernandezNo ratings yet
- מצגת קרדיולוגיה מעודכנת עם שאלות 1Document289 pagesמצגת קרדיולוגיה מעודכנת עם שאלות 1adnan shwNo ratings yet
- Mensajes Del Buen Pastor, RemediesDocument28 pagesMensajes Del Buen Pastor, RemediesSusan DeeNo ratings yet
- JURY Updated To 2020 FebDocument29 pagesJURY Updated To 2020 FebjcNo ratings yet
- CCRN-PCCN Review GastrointestinalDocument23 pagesCCRN-PCCN Review GastrointestinalGiovanni MictilNo ratings yet
- Apidra Solostar Subq: Uses and How To UseDocument16 pagesApidra Solostar Subq: Uses and How To Use-Aiyxh Ramirez Perez-No ratings yet
- Fever Chart PDFDocument1 pageFever Chart PDFThe OrthogirlNo ratings yet
- PDF Infectious Diseases and Antimicrobial Stewardship in Critical Care Medicine 4Th Edition Cheston B Cunha Editor Ebook Full ChapterDocument40 pagesPDF Infectious Diseases and Antimicrobial Stewardship in Critical Care Medicine 4Th Edition Cheston B Cunha Editor Ebook Full Chapterdonna.martinez586100% (4)
- Nasm Essentials Workshop Presentation - (pdf-2mb) PDFDocument57 pagesNasm Essentials Workshop Presentation - (pdf-2mb) PDFJean Freitas Lima100% (3)
- Ativan (Lorazepam) Drug StudyDocument3 pagesAtivan (Lorazepam) Drug StudyCHERISE CORDOVA100% (2)
- Amalgam: Its History and PerilsDocument15 pagesAmalgam: Its History and PerilsMercuryfree100% (1)
- Consumer Knowledge, Attitude and Practice Towards The Use of Monosodium Glutamate and Food Grade Bullion Cubes As Dietary ConstituentsDocument5 pagesConsumer Knowledge, Attitude and Practice Towards The Use of Monosodium Glutamate and Food Grade Bullion Cubes As Dietary ConstituentsDeEpaa ManohanNo ratings yet
- Schizophrenia and Offending: Area of Residence and The Impact of Social Disorganisation and UrbanicityDocument17 pagesSchizophrenia and Offending: Area of Residence and The Impact of Social Disorganisation and UrbanicityMustafa ŠuvalijaNo ratings yet
- Spironolactone-Induced Rash: A Case Report and ReviewDocument2 pagesSpironolactone-Induced Rash: A Case Report and ReviewasclepiuspdfsNo ratings yet
- FC MS3 (SC)Document8 pagesFC MS3 (SC)madlahuddindayangNo ratings yet
- Oncologic NursingDocument16 pagesOncologic Nursinglushxene84No ratings yet
- Snap 4dx Plus Sensitivity Specificity PDFDocument1 pageSnap 4dx Plus Sensitivity Specificity PDFDesriwanAnggaMedicaNo ratings yet
- Pathology For The Health Professions 4Th Edition Damjanov Test Bank Full Chapter PDFDocument20 pagesPathology For The Health Professions 4Th Edition Damjanov Test Bank Full Chapter PDFcrastzfeiej100% (12)
- Fermented Foods and Food Safety: ArticleDocument9 pagesFermented Foods and Food Safety: ArticlesimurabiyeNo ratings yet
- Vastu and HealthDocument9 pagesVastu and HealthShashank VeerkarNo ratings yet
- Hematologic Disorders Intensive For Brilliant Post Test Answer KeyDocument4 pagesHematologic Disorders Intensive For Brilliant Post Test Answer Keymarlou agananNo ratings yet
- Acute and Chronic PancreatitisDocument8 pagesAcute and Chronic PancreatitisIsabel CastilloNo ratings yet
- Fleas ParasitologyDocument54 pagesFleas Parasitologyhuyenthanh1807No ratings yet
- Out of Step by Arnold LeeseDocument50 pagesOut of Step by Arnold Leesealfred rosenbergNo ratings yet
- The Effects of The Great Depression On American Women in I Stand Here Ironing by Tillie OlsenDocument5 pagesThe Effects of The Great Depression On American Women in I Stand Here Ironing by Tillie OlsenMihaela TomaNo ratings yet
- Lower Respiratory Tract DiseasesDocument4 pagesLower Respiratory Tract DiseasesJulia ManaloNo ratings yet











































































































4.
3
10 February 2014
Karlos Noel R. Aleta, MD
Lecture-based trans
Peritonitis
LEARNING OBJECTIVES CRITERIA FOR DIAGNOSIS
To know the different types, causes and manifestations of Two or more of following criteria are met:
peritonitis o Temp: >38°C (100.4°F) or <36°C (96.8°F)
To know the different types, causes and manifestations of o Heart rate >90 bpm
intra-abdominal abscesses o Respiratory rate >20 bpm or PaCO2 <32 mmHg or
To know the management of peritonitis and intra- mechanical ventilation
abdominal abscesses o WBC count >12,000/L or <4000/L or >10%
immature/band forms
INTRODUCTION
Intrabdominal Infections: one of the most common and CLINICAL SPECTRUM OF INFECTIONS AND SIRS
most important challenges on surgeon INFECTION Identifiable source of microbial insult
o Skills of surgeon- require repeated laparotomies SIRS refer to the table above
o STAR- Stage Abdominal Restoration SEPSIS Identifiable source of infection + SIRS
Despite ancillary diagnostics, diagnosis is still dependent on
SEVERE SEPSIS Sepsis + organ dysfunction
clinical criteria
Sepsis + cardiovascular collapse
A mutidisciplinary approach may be as important for SEPTIC SHOCK
(requiring vasopressor support)
survival as surgery
A critically ill patient may require intensive care support
Peritoneal cavity is three times that of the surface ROUTES OF ENTRY
area of the skin, thus, it is a huge area to be infected Bacteria may enter the cavity via 4 portals
Mortality from peritonitis is about 10% (even in good units) penetrating wound
EXTERIOR
infection at laparatomy, PD
PATHOPHYSIOLOGY gangrene of viscus
INTRA-ABDOMINAL
Inflammation of the peritoneal cavity evokes series of perforation of fluid
VISCERA
events. post op leak
An inflammatory response to peritoneal injury: BLOODSTREAM as part of septicemia
o Resulting in influx of protein-rich fluid FEMALE GENITAL acute salpingitis
Activation of complement cascade TRACT puerperal infection
Up-regulation of peritoneal mesothelial cell activity ADULTS:
Invasion of peritoneum with PMN’s, neutrophils and o 30% post-op complication
macrophages o 20% acute appendicitis
Stimulation of cytokine and chemokine production o 10% perforated peptic ulcer
Local Consequences CLASSIFICATION
o Transmigration of granulocytes from peritoneal Primary
capillaries to mesothelial surface Secondary
o Dilatation of peritoneal blood vessels Tertiary
o Enhanced permeability Peritonitis from peritoneal dialysis
o Peritoneal edema
o Formation of protein-rich exudate PRIMARY Monomicrobial
SECONDARY Polymicrobial
First line of defense: clearance of noxious agents via the TERTIARY Nosocomial (Gram (-), Staph, Fungi)
lymphatics of parietal peritoneum, diaphragm and
omentum
PRIMARY
Fibrin formation acts to wall off infection Infection of the peritoneal cavity not directly related to
o Associated with abscess formation other intra-abdominal abnormality
Majority are bacterial infections commonly known as
HOST RESPONSE – 5 key factors Spontaneous Bacterial Peritonitis (SBP)
1. Inoculum size Usually occurs in the presence of ascites from variety of
2. Virulence of contaminating organisms underlying conditions
3. Presence of adjuvants within peritoneal cavity In pre-antibiotic era, it accounted for ~10% of pediatric
4. Adequacy of local, regional, systemic host defenses abdominal emergencies
5. Adequacy of initial treatment Associated with post necrotic cirrhosis & nephrotic
syndrome
In adults, 25% from alcoholic cirrhosis
SIRS
o Post-necrotic cirrhosis, lymphedema, metastatic disease,
After a severe insult, accompanied by an inability to
SLE, CAH, CHF
regulate inflammatory response
WHY?
CIRRHOTIC PATIENTS
Proinflammatory cytokines
Hematogenous → most likely
o TNF-α
o IL-1, IL-6, IL-12 o Organisms removed by liver from circulation may
o IFN-γ contaminate hepatic lymph pass through permeable
lymphatic walls into ascetic fluid
Agatep, Dela Fuente, Detera, Leynes, Rodriguez, Tejano Page 1 of 5
Peritonitis
o Portosystemic shunting → greatly decrease hepatic o CHON concentration
clearance on bacteremia & increase opportunity for o Gram staining/Culture sensitivity anaerobic or aerobic
metastatic infection → susceptible sites ~ ascetic
collection DIAGNOSIS
o Importance of intrahepatic shunting in pathogenesis Patients with (+) cultures with few leukocytes and no s/sx
of disease emphasized by infrequency in non-liver bacterascites early colonization before host response
ascetic conditions Mortality of patients with low leukocyte response is same as
o Hepatic reticuloendothelial system important in patients with high leukocyte response
removal of bacteria from circulation Conversely (-) ascitic fluid culture ~ culture negative
↓ activity in cirrhotics neutrocytic ascites (+) blood culture in 1/3 of these
↓ in phagocytic activity in cirrhotics ~ severity of patients
disease Diagnostic if GS yield is positive; more commonly negative
Bacteremia ~ 75% with aerobic – may be negative in
TB PERITONITIS (TBP) anaerobic
Most likely hematogenous spread from Usually same organism isolated in peritoneal fluid is
remote focus/foci (mostly from lung) recovered in blood
ROUTE Direct entry of tubercle bacili into the
OF peritoneal cavity from lymph node, intestine, SECONDARY
SPREAD genital tract with active disease is possible Most common cause of peritonitis
TBP may become clinically evident after From perforation of a hollow viscus or other intra-
primary focus has healed abdominal pathology
Gradual onset – fever, weight loss, malaise, Requires surgical intervention in virtually all cases
night sweats, abdominal distension Understanding of the anatomic spaces of the peritoneal
MANIFES- Abdomen “doughy”, may not be rigid cavity is crucial
TATIONS Surgery/Laparoscopy: Multiple nodules
scattered over peritoneal surface and
omentum
o Adhesions, variable amount of peritoneal
fluid
ROUTES OF ENTRANCE
Enteric bacteria
o Access into peritoneal cavity by directly traversing intact
intestinal wall
o Animal studies
o Multiplicity of species of anaerobic organisms in
peritoneal fluid with infrequent bacteremia
Pre-pubertal girls
o Ascending of genital origin
o Pneumococci in both vaginal secretions & peritoneal fluid
o Alkaline pH, vs acidic pH during post-pubertal, is less
inhibitory to bacterial growth
Transfallopian
o (+) IUD
o Spread of gonococcal or chlamydial peri-hepatitis (Fitz-
Hugh-Curtis syndrome)
o Presumably via fallopian tube and paracolic gutters to
subphrenic space
o May also be hematogenous
CLINICAL PRESENTATION
Pediatrics: acute febrile illness often confused with acute
appendicitis because of its s/sx
Adults – Cirrhotic patients: atypical, fever with or
without abdominal symptoms
Primary peritonitis: differential diagnosis for acute
decompensation of CLD especially with hepatic
encephalopathy
DIAGNOSIS
Laparotomy: diagnosis of primary peritonitis with certainty
to exclude intra-abdominal pathology
Examination of peritoneal fluid: surmise diagnosis of
peritonitis
o Cell CT / Diff CT
Agatep, Dela Fuente, Detera, Leynes, Rodriguez, Tejano Page 2 of 5
Peritonitis
PATHOLOGIC EFFECTS
Widespread absorption of toxins from large inflamed
surface
Associated paralytic ileus
o Loss of fluid
o Loss of electrolytes
o Loss of CHON
Gross abdominal distension- elevation of diaphragm
SPECIAL INVESTIGATION
CBC marked leukocytosis
SERUM AMYLASE acute pancreatitis
CHEST X-RAY (upright) pulmonary pathology
ABDOMINAL X-RAY free gas
free gas, pinpoint diagnosis,
CT SCAN
peritoneal fluid
ASPIRATION pus like, bile, urine, feces
MANAGEMENT
Recurring themes of treatment in peritonitis:
o Resuscitation- load with fluids and electrolytes
o Antibiotics- empiric treatment based on pathology
o Peritoneal lavage- culture fluid
TERTIARY o Source control- of pathology; liters of NSS: saline lavage
Defined as recurrent infection of the peritoneal cavity
after an episode of a primary or secondary peritonitis NON-OPERATIVE TREATMENT
Occurs when source control, antiBxTx or host immunity are INDICATIONS
inadequate o Acute Pancreatitis
o Some cases of typhoid peritonitis
MICROBIAL FLORA o Pelvic peritonitis
Feel an inflammatory mass, vaginal or rectal
E. coli
Confirm by aspiration
Streptococcus fecalis
FROM BOWEL- Drain pus vaginally/rectally
Pseudomonas
MIXED FECAL o Pus mainly under diaphragm
Klebsiella
FLORA o Peritonitis confirmed by aspiration; but patient too ill to
Proteus
withstand laparotomy. Delay operation until patient
Anaerobic: Clostridium, Bacteroides
improved
Chlamydial
GYNECOLOGIC
Gonococcal
PERITONITIS IN CAPD
Streptococcal
CAPD Continuous Ambulatory Peritoneal Dialysis
Streptococcal
Safe cost-effective treatment for ESRD (End Stage Renal
BLOODBORNE Pneumococcal
Disease)
Staphylococcal
Complication of Peritonitis
Tuberculous
Microbial Factors:
o Ability to grow in dialysis fluid
CLINICAL FEATURE o Production of extracellular (biofilm)
Depends on precipitating cause or History
Severe pain lie still
Irritation of the diaphragm shoulder tip
Vomiting
EARLY Temperature and pulse rate rises/elevated
Localized/generalized tenderness extent
Abdominal wall rigidrebound tenderness
Abdominal silenthear heart beat and respi
Direct Rectal Exam (DRE): tenderness on
Pouch of Douglas
Abdomen: distended, tympanitic, signs of free
fluid
ADVANCE Toxic: feeble rapid pulse
Vomiting feculent
Skin: moist, cold, cyanosed Peritoneal Dialysis
Agatep, Dela Fuente, Detera, Leynes, Rodriguez, Tejano Page 3 of 5
Peritonitis
o Complex interplay of opsonisation, phagocytosis and
intercellular killing by peritoneal macrophage,
mesothelials and neutrophils
BUT Dialyzed peritoneal cavity not a supportive milieu for
operations of cellular and immunologic cellular mechanisms
o Low pH, high osmolarity, IgG, complement
o Correlation between host immunity and incidence of
peritonitis not yet well-established
MICROBIOLOGY
Staph aureus
P. aeruginosa
CLINICAL PRESENTATION
Any 2 criterion to diagnose CAPD-related peritonitis
1. Sign and symptom of peritoneal irritation
Abdominal Pain
2. Cloudy dialysate effluent with WBC count > 100mm3
3. Positive culture of dialysate fluid
4. Turbid dialysate by abdominal pain and/or tenderness
DIFFERENTIAL DIAGNOSIS OF A CLOUDY EFFLUENT
Culture-positive infectious peritonitis
Infectious peritonitis with sterile cultures
Chemical peritonitis
Eosinophilia of the effluent
Hemoperitoneum
Malignancy (rare)
Chylous effluent (rare)
Specimen taken from “dry” abdomen
MANAGEMENT AND PREVENTION
AMBULATORY BASIS intraperitoneal antibiotics
HOSPITALIZATION severely ill
unable to manage administration
of antibiotics at home
INTRA-PERITONEAL permits high concentration and
ADMINISTRATION self-delivery by the patient 10-
OF ANTIBIOTICS 14days
PREFERRED
METHOD FOR Rx
DELIVERY
TERMINOLOGIES FOR PERITONITIS
an episode that occurs within 4 weeks of
2 MAIN ROUTES OF INFECTION RECURRENT completion of treatment of a prior episode
TRANSLUMINAL from break in sterile technique during but with a different organism
dialysate exchange an episode that occurs within 4 weeks of
CONTIGUOUS microorganisms access the completion of treatment of a prior episode
SPREAD peritoneum along tract of PD catheter RELAPSING
with the same organism or 1 sterile
LESSER ROUTES episode
HEMATOGENOUS from a known distant site of infection an episode that occurs > 4 weeks after
SPREAD REPEAT completion of treatment of a prior episode
DIRECT from GI tract with the same organism
CONTAMINATION failure of effluent to clear after 5 days of
REFRACTORY
appropriate antibiotics
HOST DEFENSE FACTORS CATHETER- peritonitis in conjuction with an exit-site
Microorganisms removed from dialysate cavity by RELATED or tunnel infection with the same
o Fibrin trapping and sequestration of microorganisms PERITONITIS organism or 1 sterile site
operate effectively despite dilution of fibrinogen and
coagulation proteins
o Removal of dialysate serves to or eliminate inoculum
of contaminating microorganisms
Agatep, Dela Fuente, Detera, Leynes, Rodriguez, Tejano Page 4 of 5
Peritonitis
INDICATIONS FOR CATHETER REMOVAL FOR PD- ABDOMINAL ABSCESS
RELATED INFECTIONS Observe
Refractory peritonitis Document
Relapsing peritonitis Intervene if deteriorating
Refractory exit site and tunnel infection o Surgical or percutaneous
Fungal peritonitis
Catheter removal may also be considered for:
o Repeat peritonitis
o Mycobactrial peritonitis
o Multiple enteric organisms
ABSCESS IN THE ABDOMEN
CLINICAL PRESENTATION
s/p (status post) laparotomy 14-21 days
o Temperature does not fall, or it falls & then rises in
spikey pattern w/c shows (+) pus somewhere within
o Patient not well, does not eat, loses weight
o ↑ WBC
o If loops of his gut pass through abscess → may become
obstructed acutely or sub-acutely
LOCALIZED ABSCESS
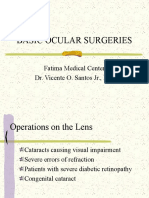
Can be a result from: Figure: Intra-abdominal abscess, CT scan (CT scan of the
o Generalized peritonitis – they are one of its major pelvis showing a large intra-abdominal mass)
complications
o Some primary focus of infection – e.g. appendicitis or
SUBPHRENIC ABSCESS
salpingitis (PID)
Peritonitis – either local or general
o An abdominal injury in which gut was perforated or
o PPU (Perforated Peptic Ulcer)
devitalized
o Typhoid ulcer
o Any laparotomy
o Appendicitis
o Infected CS (Caesarean Section)
o PID (Pelvic Inflammatory Disease)
Injury to ruptured viscus
s/p laparotomy with contamination
Ruptures amebic liver abscess
PELVIC ABSCESS
From:
o female genital tract
o appendicitis
o generalized peritonitis
Drainage:
o vaginally (2 routes for female)
o rectally
Agatep, Dela Fuente, Detera, Leynes, Rodriguez, Tejano Page 5 of 5
You might also like
- 4.4 Acute AbdomenDocument6 pages4.4 Acute AbdomenMiguel C. Dolot100% (1)
- A Grinchmas CarolDocument5 pagesA Grinchmas CarolMikey VultaggioNo ratings yet
- Peritonitis: Update On Pathophysiology, Clinical Manifestations, and ManagementDocument11 pagesPeritonitis: Update On Pathophysiology, Clinical Manifestations, and ManagementMuhamad Chairul SyahNo ratings yet
- Peritonitis: Update On Pathophysiology, Clinical Manifestations, and ManagementDocument11 pagesPeritonitis: Update On Pathophysiology, Clinical Manifestations, and ManagementerikafebriyanarNo ratings yet
- Peritonitis Update On Pathophysiology, Clinical Manifestations, and PDFDocument11 pagesPeritonitis Update On Pathophysiology, Clinical Manifestations, and PDFAnonymous InJS6aYZ100% (1)
- Leture 7 Infection in IcuDocument93 pagesLeture 7 Infection in IcuVincent Jofette AventunaNo ratings yet
- PeritonitisDocument78 pagesPeritonitisTan Dan100% (1)
- 1.3 PeritonitisDocument14 pages1.3 PeritonitisΜατθαίος ΠαππάςNo ratings yet
- Intra-Abdominal and Pelvic EmergenciesDocument21 pagesIntra-Abdominal and Pelvic Emergenciesqhrn48psvwNo ratings yet
- Management of Intra-Abdominal InfectionDocument65 pagesManagement of Intra-Abdominal InfectionKamran SherazNo ratings yet
- Sonographic Detection of Enlarged Mesenteric Lymph Nodes in Children and Its SignificanceDocument15 pagesSonographic Detection of Enlarged Mesenteric Lymph Nodes in Children and Its SignificanceInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- L09 - Diseases of The PeritoneumDocument13 pagesL09 - Diseases of The PeritoneumS sNo ratings yet
- Session 6Document72 pagesSession 6Alliah Marie CababarosNo ratings yet
- La Fasciite Nécrosante Sur Site D InjectionDocument6 pagesLa Fasciite Nécrosante Sur Site D InjectionDr ZarhouniNo ratings yet
- Peritonitis PDFDocument4 pagesPeritonitis PDFAndreas TheoNo ratings yet
- Fistulas Enterocutaneas MaingotDocument20 pagesFistulas Enterocutaneas MaingotroyvillafrancaNo ratings yet
- RETROPERITONEALDocument3 pagesRETROPERITONEALmichelleNo ratings yet
- 06 Peritonitis. Acute General Purulent and Encapsulated PeritonitisesDocument45 pages06 Peritonitis. Acute General Purulent and Encapsulated PeritonitisesFikri HaqNo ratings yet
- Siu Empiric Antibiotics For Select InfectionsDocument30 pagesSiu Empiric Antibiotics For Select InfectionspasswordNo ratings yet
- Penanganan Sepsis PitDocument43 pagesPenanganan Sepsis PitElfa RiniNo ratings yet
- AppendicitisDocument17 pagesAppendicitisalwinNo ratings yet
- Lower Genital Tract InfectionsDocument70 pagesLower Genital Tract InfectionsAbegail IbañezNo ratings yet
- PeritonitissDocument46 pagesPeritonitissNinaNo ratings yet
- Patofisiologi, Manifestasi Klinik, Dan Manajemen PeritonitisDocument11 pagesPatofisiologi, Manifestasi Klinik, Dan Manajemen Peritonitistika tikaNo ratings yet
- PeritonitisDocument34 pagesPeritonitisabrar_zaidiNo ratings yet
- Journal PeritonitisDocument7 pagesJournal PeritonitisEudia SiagianNo ratings yet
- Rotar O.V. As - Prof. General Surgery, BSMUDocument63 pagesRotar O.V. As - Prof. General Surgery, BSMUOleksandr RotarNo ratings yet
- Necrotising Fascitis: Recent Advances in Surgery 39Th EditionDocument36 pagesNecrotising Fascitis: Recent Advances in Surgery 39Th EditionPraveen CpNo ratings yet
- SEPSIS Incomplete-NotesDocument4 pagesSEPSIS Incomplete-NotesbmiakhylaellaineNo ratings yet
- Lap Pelvic DrainageDocument9 pagesLap Pelvic DrainageMuneer KhalamNo ratings yet
- PERITONITISDocument4 pagesPERITONITISAmoroso, Marian Corneth D.No ratings yet
- Peritonitis: Dr. Mahmoud Al-AwayshehDocument35 pagesPeritonitis: Dr. Mahmoud Al-Awayshehraed faisalNo ratings yet
- Fournier'S Gangrene: Rajah Amina SuleimanDocument27 pagesFournier'S Gangrene: Rajah Amina SuleimanAmina RajahNo ratings yet
- Afecciones Anorrectales Benignas Absceso Perianal, Fístula Anal, Hemorroides, Fisuras y Seno PilonidalDocument7 pagesAfecciones Anorrectales Benignas Absceso Perianal, Fístula Anal, Hemorroides, Fisuras y Seno PilonidalJoshua MaciasNo ratings yet
- Circulatory System Infectious Diseases: Dengue Hemorrhagic Shock SyndromeDocument3 pagesCirculatory System Infectious Diseases: Dengue Hemorrhagic Shock Syndromegrazelantonette.calubNo ratings yet
- Abdominal Tuberculosi S: DR - Prateek Kumar Junior ResidentDocument68 pagesAbdominal Tuberculosi S: DR - Prateek Kumar Junior ResidentututelNo ratings yet
- Typhoid Enteric Fever From UiA Volume 32 Final WebDocument4 pagesTyphoid Enteric Fever From UiA Volume 32 Final WebJayesh KumarNo ratings yet
- 72 Ventilator Associated Pneumonia PDFDocument5 pages72 Ventilator Associated Pneumonia PDFV RakeshreddyNo ratings yet
- Peritonitis and AppendicitisDocument35 pagesPeritonitis and AppendicitisRose Anne AbivaNo ratings yet
- Pleural EffusionDocument3 pagesPleural EffusionAubrey PerezNo ratings yet
- Metritis With Pelvic CellulitisDocument2 pagesMetritis With Pelvic CellulitisCleoGomezNo ratings yet
- SECTION I Inflammatory, Infective, and Congenital: Pyogenic Liver AbscessDocument12 pagesSECTION I Inflammatory, Infective, and Congenital: Pyogenic Liver AbscessandresNo ratings yet
- Surgical Infection 1Document120 pagesSurgical Infection 1Liezel Dejumo BartolataNo ratings yet
- Peritonitis 1Document6 pagesPeritonitis 1m.rizoniakmalNo ratings yet
- F01ddiabrtes and InfectionDocument82 pagesF01ddiabrtes and InfectionAbdel-razek ElmelegiNo ratings yet
- Aspects of Nursing in The Control and Prevention of Peritoneal Dialysis InfectionsDocument27 pagesAspects of Nursing in The Control and Prevention of Peritoneal Dialysis InfectionsNanang AdhoniNo ratings yet
- Urinary Tract and Male Genital SystemDocument5 pagesUrinary Tract and Male Genital SystemMonicaNo ratings yet
- Empyema - Rol of SurgeonDocument5 pagesEmpyema - Rol of Surgeondantheman123No ratings yet
- (Surg2-Trans) 4.01 AppendixDocument7 pages(Surg2-Trans) 4.01 AppendixJake Brandon M. Andal, RNDNo ratings yet
- PeritonitisDocument15 pagesPeritonitiscgqphqdrytNo ratings yet
- Disorders of The Pleura: Pleural EffusionDocument42 pagesDisorders of The Pleura: Pleural EffusionIrma NurainiNo ratings yet
- Block 3.3 Sesi 3 Pathology of Urinary Tract: by Asdos 2011: Vetta Awe Eric Lily Fiko Ghana Ikal Linda May FahmiDocument96 pagesBlock 3.3 Sesi 3 Pathology of Urinary Tract: by Asdos 2011: Vetta Awe Eric Lily Fiko Ghana Ikal Linda May Fahmimail junkNo ratings yet
- Jurnal 8Document24 pagesJurnal 8agus indrawanNo ratings yet
- MPDFDocument11 pagesMPDFKeljang MoktanNo ratings yet
- 338 Typhoid Enteric FeverDocument6 pages338 Typhoid Enteric FeverSurbhi ThakurNo ratings yet
- Pneumonia PresentationDocument23 pagesPneumonia Presentationapi-546694141No ratings yet
- Acutel AppendicitisDocument8 pagesAcutel Appendicitislogamarquell17No ratings yet
- ASOMDocument41 pagesASOMArunkumar S KumarNo ratings yet
- Absceso Hepatico HarrisonDocument2 pagesAbsceso Hepatico HarrisonZafiss ChaconNo ratings yet
- Fast Facts: Complex Perianal Fistulas in Crohn's Disease: A multidisciplinary approach to a clinical challengeFrom EverandFast Facts: Complex Perianal Fistulas in Crohn's Disease: A multidisciplinary approach to a clinical challengeNo ratings yet
- Urinary Tract Infection in Children - Classification, Diagnosis and TreatmentFrom EverandUrinary Tract Infection in Children - Classification, Diagnosis and TreatmentNo ratings yet
- Nucleotide MetabolismDocument17 pagesNucleotide MetabolismMiguel C. DolotNo ratings yet
- 4.2 Abdominal Wall Hernia (Jerome Villacorta's Conflicted Copy 2014-03-22)Document7 pages4.2 Abdominal Wall Hernia (Jerome Villacorta's Conflicted Copy 2014-03-22)Miguel C. DolotNo ratings yet
- Shoulder Dystocia: Ina S. Irabon, MD, Fpogs, FPSRM, FpsgeDocument25 pagesShoulder Dystocia: Ina S. Irabon, MD, Fpogs, FPSRM, FpsgeMiguel C. DolotNo ratings yet
- 02.03-03 CNS II - Skeletal Muscle RelaxantsDocument7 pages02.03-03 CNS II - Skeletal Muscle RelaxantsMiguel C. DolotNo ratings yet
- Diabetes Mellitus 1Document47 pagesDiabetes Mellitus 1Miguel C. DolotNo ratings yet
- Basic Neuro-Ophthalmology: Common Problems SeenDocument6 pagesBasic Neuro-Ophthalmology: Common Problems SeenMiguel C. DolotNo ratings yet
- Cornea and External DiseasesDocument18 pagesCornea and External DiseasesMiguel C. DolotNo ratings yet
- Basic Ocular Surgeries: Fatima Medical Center Dr. Vicente O. Santos JR., MDDocument53 pagesBasic Ocular Surgeries: Fatima Medical Center Dr. Vicente O. Santos JR., MDMiguel C. DolotNo ratings yet
- 02.01-04 CNS I - AntiepilepticsDocument10 pages02.01-04 CNS I - AntiepilepticsMiguel C. DolotNo ratings yet
- Angeline D. Alabastro, M.D.: CNS Pharmacology I: AntiepilepticsDocument10 pagesAngeline D. Alabastro, M.D.: CNS Pharmacology I: AntiepilepticsMiguel C. DolotNo ratings yet
- 02.03-02 CNS II - Local AnesthesiaDocument5 pages02.03-02 CNS II - Local AnesthesiaMiguel C. DolotNo ratings yet
- 02.03-01 CNS II - General AnesthesiaDocument9 pages02.03-01 CNS II - General AnesthesiaMiguel C. DolotNo ratings yet
- 02.01-03 CNS I - AlcoholsDocument5 pages02.01-03 CNS I - AlcoholsMiguel C. DolotNo ratings yet
- 02.05. Patient-Doctor Relationship and Interviewing TechniquesDocument10 pages02.05. Patient-Doctor Relationship and Interviewing TechniquesMiguel C. DolotNo ratings yet
- Angeline D. Alabastro, M.D. Angeline D. Alabastro, M.D. Angeline D. Alabastro, M.DDocument7 pagesAngeline D. Alabastro, M.D. Angeline D. Alabastro, M.D. Angeline D. Alabastro, M.DMiguel C. DolotNo ratings yet
- 02.04. Physical Examination and Laboratory Tests in PsychiatryDocument12 pages02.04. Physical Examination and Laboratory Tests in PsychiatryMiguel C. DolotNo ratings yet
- 02.01-01 CNS I - Central NeurotransmittersDocument3 pages02.01-01 CNS I - Central NeurotransmittersMiguel C. DolotNo ratings yet
- Psychiatric History: Doc Los BañosDocument6 pagesPsychiatric History: Doc Los BañosMiguel C. DolotNo ratings yet
- Los Baños: Mental Status ExamDocument5 pagesLos Baños: Mental Status ExamMiguel C. DolotNo ratings yet
- Aminoglycoside Dosing GuidelinesDocument3 pagesAminoglycoside Dosing GuidelinesaeromintNo ratings yet
- PE (General and Head Neck)Document14 pagesPE (General and Head Neck)antomiolam1218No ratings yet
- Patient Medication ProfileDocument4 pagesPatient Medication ProfileLaura HernandezNo ratings yet
- מצגת קרדיולוגיה מעודכנת עם שאלות 1Document289 pagesמצגת קרדיולוגיה מעודכנת עם שאלות 1adnan shwNo ratings yet
- Mensajes Del Buen Pastor, RemediesDocument28 pagesMensajes Del Buen Pastor, RemediesSusan DeeNo ratings yet
- JURY Updated To 2020 FebDocument29 pagesJURY Updated To 2020 FebjcNo ratings yet
- CCRN-PCCN Review GastrointestinalDocument23 pagesCCRN-PCCN Review GastrointestinalGiovanni MictilNo ratings yet
- Apidra Solostar Subq: Uses and How To UseDocument16 pagesApidra Solostar Subq: Uses and How To Use-Aiyxh Ramirez Perez-No ratings yet
- Fever Chart PDFDocument1 pageFever Chart PDFThe OrthogirlNo ratings yet
- PDF Infectious Diseases and Antimicrobial Stewardship in Critical Care Medicine 4Th Edition Cheston B Cunha Editor Ebook Full ChapterDocument40 pagesPDF Infectious Diseases and Antimicrobial Stewardship in Critical Care Medicine 4Th Edition Cheston B Cunha Editor Ebook Full Chapterdonna.martinez586100% (4)
- Nasm Essentials Workshop Presentation - (pdf-2mb) PDFDocument57 pagesNasm Essentials Workshop Presentation - (pdf-2mb) PDFJean Freitas Lima100% (3)
- Ativan (Lorazepam) Drug StudyDocument3 pagesAtivan (Lorazepam) Drug StudyCHERISE CORDOVA100% (2)
- Amalgam: Its History and PerilsDocument15 pagesAmalgam: Its History and PerilsMercuryfree100% (1)
- Consumer Knowledge, Attitude and Practice Towards The Use of Monosodium Glutamate and Food Grade Bullion Cubes As Dietary ConstituentsDocument5 pagesConsumer Knowledge, Attitude and Practice Towards The Use of Monosodium Glutamate and Food Grade Bullion Cubes As Dietary ConstituentsDeEpaa ManohanNo ratings yet
- Schizophrenia and Offending: Area of Residence and The Impact of Social Disorganisation and UrbanicityDocument17 pagesSchizophrenia and Offending: Area of Residence and The Impact of Social Disorganisation and UrbanicityMustafa ŠuvalijaNo ratings yet
- Spironolactone-Induced Rash: A Case Report and ReviewDocument2 pagesSpironolactone-Induced Rash: A Case Report and ReviewasclepiuspdfsNo ratings yet
- FC MS3 (SC)Document8 pagesFC MS3 (SC)madlahuddindayangNo ratings yet
- Oncologic NursingDocument16 pagesOncologic Nursinglushxene84No ratings yet
- Snap 4dx Plus Sensitivity Specificity PDFDocument1 pageSnap 4dx Plus Sensitivity Specificity PDFDesriwanAnggaMedicaNo ratings yet
- Pathology For The Health Professions 4Th Edition Damjanov Test Bank Full Chapter PDFDocument20 pagesPathology For The Health Professions 4Th Edition Damjanov Test Bank Full Chapter PDFcrastzfeiej100% (12)
- Fermented Foods and Food Safety: ArticleDocument9 pagesFermented Foods and Food Safety: ArticlesimurabiyeNo ratings yet
- Vastu and HealthDocument9 pagesVastu and HealthShashank VeerkarNo ratings yet
- Hematologic Disorders Intensive For Brilliant Post Test Answer KeyDocument4 pagesHematologic Disorders Intensive For Brilliant Post Test Answer Keymarlou agananNo ratings yet
- Acute and Chronic PancreatitisDocument8 pagesAcute and Chronic PancreatitisIsabel CastilloNo ratings yet
- Fleas ParasitologyDocument54 pagesFleas Parasitologyhuyenthanh1807No ratings yet
- Out of Step by Arnold LeeseDocument50 pagesOut of Step by Arnold Leesealfred rosenbergNo ratings yet
- The Effects of The Great Depression On American Women in I Stand Here Ironing by Tillie OlsenDocument5 pagesThe Effects of The Great Depression On American Women in I Stand Here Ironing by Tillie OlsenMihaela TomaNo ratings yet
- Lower Respiratory Tract DiseasesDocument4 pagesLower Respiratory Tract DiseasesJulia ManaloNo ratings yet