Download as pdf or txt
You might also like
- NCLEX-RN Q&A Flash Cards by Ray A. Hargrove-Huttel, Kathryn Cadenhead ColgroDocument793 pagesNCLEX-RN Q&A Flash Cards by Ray A. Hargrove-Huttel, Kathryn Cadenhead ColgroHeri Zalmes Dodge Tomahawk94% (53)
- Introduction To PediatricsDocument13 pagesIntroduction To PediatricsElvis100% (4)
- Bio Mechanical Analysis of FootballDocument54 pagesBio Mechanical Analysis of FootballMunesh kumar srivastava58% (12)
- London Med Student Neurology CasesDocument11 pagesLondon Med Student Neurology CasesAmmuNo ratings yet
- Ombregt Ludwig. A System of Orthopaedic Medicine. 3th Edition. Elesvier. 2013. B9780702031458000867 - Web Pemeriksaan FisikDocument6 pagesOmbregt Ludwig. A System of Orthopaedic Medicine. 3th Edition. Elesvier. 2013. B9780702031458000867 - Web Pemeriksaan FisikSonia RogersNo ratings yet
- Pectus Carinatum, (Pigeon Chest) A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandPectus Carinatum, (Pigeon Chest) A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
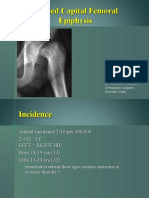
- Slipped Capital Femoral Epiphysis: Vivek PandeyDocument30 pagesSlipped Capital Femoral Epiphysis: Vivek PandeyvivpanNo ratings yet
- KYPHOSIS Con FinalDocument52 pagesKYPHOSIS Con FinalAbdul Ghaffar AbdullahNo ratings yet
- Slipped Capital Femoral EpiphysisDocument40 pagesSlipped Capital Femoral EpiphysisDrAshesh Desai100% (2)
- Surgery - Dychioco - Fractures of Pelvis & Lower ExtremityDocument87 pagesSurgery - Dychioco - Fractures of Pelvis & Lower Extremity3rd yrsNo ratings yet
- Fracture of Radius and Ulna 3Document38 pagesFracture of Radius and Ulna 3Noor Al Zahraa AliNo ratings yet
- 04 - Femur Neck and HeadDocument28 pages04 - Femur Neck and HeadammarNo ratings yet
- Cephalopelvic DisproportionDocument6 pagesCephalopelvic DisproportionBaljinder kaurNo ratings yet
- Developmental Dysplasia of The Hip (DDH) : Dr. Robert Miawa 14/02/2019Document67 pagesDevelopmental Dysplasia of The Hip (DDH) : Dr. Robert Miawa 14/02/2019Gladys MainaNo ratings yet
- Hip Dislocations and Femoral Head Fractures: John T. Gorczyca, MDDocument97 pagesHip Dislocations and Femoral Head Fractures: John T. Gorczyca, MDLassie LazyNo ratings yet
- Pelvic FracturesDocument39 pagesPelvic Fracturescromwellopoku42No ratings yet
- DDH ManagementDocument121 pagesDDH ManagementAnonymous 14fGB26QuNo ratings yet
- Hip ProblemsDocument24 pagesHip ProblemsOng Siaw YenNo ratings yet
- CLUBFOOT, Polydactily, Spina BividaDocument39 pagesCLUBFOOT, Polydactily, Spina BividaRobertus Dwi AtmokoNo ratings yet
- Should All Unstable Slipped Capital Femoral Epiphysis Be Treated OpenDocument7 pagesShould All Unstable Slipped Capital Femoral Epiphysis Be Treated Openyarimar hoyosNo ratings yet
- Deslizamiento Epifisiario Femur OvidDocument7 pagesDeslizamiento Epifisiario Femur Ovidnathalia_pastasNo ratings yet
- Developmental Dysplasia of Hip (DDH) : Nizar Abdul MajeedDocument37 pagesDevelopmental Dysplasia of Hip (DDH) : Nizar Abdul MajeedAh ZhangNo ratings yet
- Congenital DeformitiesDocument102 pagesCongenital DeformitiesFahmi MujahidNo ratings yet
- Fracture-Dislocation of The Hip-KaizarDocument69 pagesFracture-Dislocation of The Hip-KaizarKaizar Ennis100% (1)
- DR - O. K. A. SamuelsDocument76 pagesDR - O. K. A. Samuelsgdudex118811No ratings yet
- Deformities OF The Lower Limb: DR - Tehreem NasirDocument57 pagesDeformities OF The Lower Limb: DR - Tehreem NasirAhmed SaeedNo ratings yet
- Perthes Ds SUFIDocument25 pagesPerthes Ds SUFIfreelancer.am1302No ratings yet
- Cord PresentationDocument24 pagesCord PresentationAmirNo ratings yet
- Assessing Cephalopelvic Disproportion: Back To The BasicsDocument27 pagesAssessing Cephalopelvic Disproportion: Back To The Basicsbeechrissanty_807904No ratings yet
- Femoral Neck FracturesDocument8 pagesFemoral Neck FracturesMorshed Mahbub AbirNo ratings yet
- CHD 1sDocument32 pagesCHD 1sLauNo ratings yet
- Common Lower Limb Fracture: DR Tarif Alakhras Orthopedic Surgeon KFMCDocument49 pagesCommon Lower Limb Fracture: DR Tarif Alakhras Orthopedic Surgeon KFMCahmad albab100% (1)
- Hip DislocDocument67 pagesHip DislocAli TawbeNo ratings yet
- Sprengel's ShoulderDocument21 pagesSprengel's ShoulderNahayo Xavier100% (1)
- Fractures and Dislocations About The Elbow in The Pediatric PatientDocument90 pagesFractures and Dislocations About The Elbow in The Pediatric PatientCezara TimofteNo ratings yet
- Dislocation of The Hip (July 2020)Document27 pagesDislocation of The Hip (July 2020)thehexhealthNo ratings yet
- Kyphosis Lordosis Defined This Drawing Represents The Spinal Condition ofDocument36 pagesKyphosis Lordosis Defined This Drawing Represents The Spinal Condition ofSoare Elena-CosminaNo ratings yet
- Chapter 5 Pediatric PodiatryDocument88 pagesChapter 5 Pediatric Podiatrypodmmgf100% (1)
- Congenital Dysplasia of Hip (CDH) Developmental Dysplasia of The Hip (DDH)Document50 pagesCongenital Dysplasia of Hip (CDH) Developmental Dysplasia of The Hip (DDH)NarishaAmeliaNo ratings yet
- Fractures of Shoulder and Elbow EditedDocument25 pagesFractures of Shoulder and Elbow EditedSurgicalgownNo ratings yet
- CPDDocument45 pagesCPDVijith.V.kumar100% (1)
- Andi Rahmat Hidayat C 111 07 104 Advisor: Dr. Andi Sirfa Dr. Helmiyadi Kuswardhana Supervisor: Dr. Henry Yurianto, M.Phill, PHD, SP - OtDocument30 pagesAndi Rahmat Hidayat C 111 07 104 Advisor: Dr. Andi Sirfa Dr. Helmiyadi Kuswardhana Supervisor: Dr. Henry Yurianto, M.Phill, PHD, SP - OtAndi Rahmat HidayatNo ratings yet
- CPD and Contracted PelvisDocument53 pagesCPD and Contracted Pelvismaxim tomuNo ratings yet
- DDHDocument30 pagesDDHsayedmNo ratings yet
- Myelography in ChildrenDocument16 pagesMyelography in ChildrenFinna Tryasti Fidianti1BNo ratings yet
- Developmental Dysplasia of The HipDocument72 pagesDevelopmental Dysplasia of The HipVignesh WaranNo ratings yet
- CTEVDocument46 pagesCTEVjhogie afitnandriNo ratings yet
- 13-Traumatic Injuries Related To Labour&BirthDocument27 pages13-Traumatic Injuries Related To Labour&BirthLittleThingsInsideNo ratings yet
- Pelvic Fractures PksDocument48 pagesPelvic Fractures PksprinceveettoorNo ratings yet
- Birth Injuries: Dr. Alsayed Alsharkawy Senior Pediatric Lecturer Widad University CollegeDocument35 pagesBirth Injuries: Dr. Alsayed Alsharkawy Senior Pediatric Lecturer Widad University CollegeEllis NabilaNo ratings yet
- Anomalies of Skeletal System-1Document44 pagesAnomalies of Skeletal System-1Meena Koushal100% (1)
- Malunion of An in Utero Metacarpal Fracture in A Standardbred Mare Presenting For DystociaDocument9 pagesMalunion of An in Utero Metacarpal Fracture in A Standardbred Mare Presenting For Dystociakarinda dyllaNo ratings yet
- Treatment of Neglegted Sternoclavicular (SC) Dislocation With Cannulated Screw and Cerclage Wire OsteosynthesisDocument5 pagesTreatment of Neglegted Sternoclavicular (SC) Dislocation With Cannulated Screw and Cerclage Wire OsteosynthesisPeko PekoNo ratings yet
- Cerebral PalsyDocument16 pagesCerebral PalsyReza Devianto HambaliNo ratings yet
- Foot Deformities Infant: AssessmentDocument5 pagesFoot Deformities Infant: AssessmentAnup PednekarNo ratings yet
- Traumatic Spondyloptosis Resulting in Complete SCI Final RevDocument9 pagesTraumatic Spondyloptosis Resulting in Complete SCI Final RevSamuel WillyartoNo ratings yet
- Tail Pull InjuryDocument10 pagesTail Pull InjuryClarissa NiciporciukasNo ratings yet
- Hip ProblemsDocument46 pagesHip ProblemsDhiya' VinaNo ratings yet
- Spine InjuriesDocument58 pagesSpine InjuriesVinwin777No ratings yet
- Scfe2 140618022225 Phpapp01Document48 pagesScfe2 140618022225 Phpapp01Alexandro WiyandaNo ratings yet
- Pephalo Pelvicdisproportion &contracted PelvisDocument38 pagesPephalo Pelvicdisproportion &contracted PelvisAltynaiNo ratings yet
- Femoral Neck FracturesDocument10 pagesFemoral Neck FracturesMorshed Mahbub AbirNo ratings yet
- Potentially Life-Threatening Extremity InjuriesDocument41 pagesPotentially Life-Threatening Extremity Injuriesyuliaoksiyulanda ingeniopadangNo ratings yet
- Transcript2021feb05 DCM 2017 71788Document5 pagesTranscript2021feb05 DCM 2017 71788ElvisNo ratings yet
- STANDARD OPERATING PROCEDURES For Establishing and Running Key Populations Clinics in KenyaDocument40 pagesSTANDARD OPERATING PROCEDURES For Establishing and Running Key Populations Clinics in KenyaElvisNo ratings yet
- National Guidelines For Safe Management of Health Care Waste Final1Document82 pagesNational Guidelines For Safe Management of Health Care Waste Final1ElvisNo ratings yet
- Puerperium and Its Management 1Document35 pagesPuerperium and Its Management 1Elvis100% (2)
- Pediatric Medical Emergencies Rev Oct 2016Document27 pagesPediatric Medical Emergencies Rev Oct 2016ElvisNo ratings yet
- MSU GS PolicyDocument42 pagesMSU GS PolicyElvisNo ratings yet
- Problems in Early Pregnancy - NBT002073Document8 pagesProblems in Early Pregnancy - NBT002073ElvisNo ratings yet
- Management of Postpartum Haemorrhage (C Obs 43) Review July 2017Document17 pagesManagement of Postpartum Haemorrhage (C Obs 43) Review July 2017ElvisNo ratings yet
- Juvenile ArthritisDocument11 pagesJuvenile ArthritisElvisNo ratings yet
- Dog Bite 3Document2 pagesDog Bite 3ElvisNo ratings yet
- Cerebrovascular Accident/Brain Attack: Gideon Gachihi Associate Faculty, MKUDocument52 pagesCerebrovascular Accident/Brain Attack: Gideon Gachihi Associate Faculty, MKUElvisNo ratings yet
- Dermatology Updated 2020Document57 pagesDermatology Updated 2020ElvisNo ratings yet
- The Physiology of The SkinDocument39 pagesThe Physiology of The SkinElvisNo ratings yet
- Hemolytic Disease of Newborn Class NotesDocument37 pagesHemolytic Disease of Newborn Class NotesElvisNo ratings yet
- Infant of A Diabetic MotherDocument20 pagesInfant of A Diabetic MotherElvisNo ratings yet
- Birth Asphyxia: by Anne E. Odaro MCM/2017/69852Document26 pagesBirth Asphyxia: by Anne E. Odaro MCM/2017/69852ElvisNo ratings yet
- Typhoid Fever,-WPS OfficeDocument5 pagesTyphoid Fever,-WPS OfficeElvisNo ratings yet
- Written in My Own Hearts Blood by Diana Gabaldon ExtractDocument50 pagesWritten in My Own Hearts Blood by Diana Gabaldon ExtractOrion Publishing Group33% (3)
- Trauma: Dr. Hasanain Abdulammer JasimDocument41 pagesTrauma: Dr. Hasanain Abdulammer Jasimميمونه عبد الرحيم مصطفىNo ratings yet
- LUS-HSE-FM4-453-003.01 - Incident Investigation ReportDocument11 pagesLUS-HSE-FM4-453-003.01 - Incident Investigation ReportamalNo ratings yet
- Surfers Shoulder Ebook Surf ShoreDocument8 pagesSurfers Shoulder Ebook Surf ShoreDhaiba IsmailNo ratings yet
- Genu Valgus & Genu VarusDocument51 pagesGenu Valgus & Genu VarusAlfionita WikaNo ratings yet
- Power Steel Specialist Trading Corp. and Barlines: A. Responsibilities of TransporterDocument3 pagesPower Steel Specialist Trading Corp. and Barlines: A. Responsibilities of Transportererikha_aranetaNo ratings yet
- Scapular Dyskinesis: From Basic Science To Ultimate TreatmentDocument17 pagesScapular Dyskinesis: From Basic Science To Ultimate TreatmentAlonso FernandezNo ratings yet
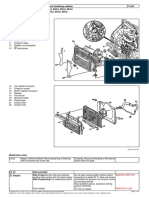
- Removing and Installing RadiatorDocument2 pagesRemoving and Installing RadiatorAnonymous d8ermLyF3No ratings yet
- Pappu Kalani Inder Bhatija Murder Case JudgementDocument76 pagesPappu Kalani Inder Bhatija Murder Case JudgementSampath Bulusu100% (1)
- Peter BanagDocument3 pagesPeter BanagRonald Caringal CusiNo ratings yet
- 24 Top Orthopedic TestsDocument29 pages24 Top Orthopedic TestsDavid Gal100% (1)
- Thorax: Thoracic Spine Anatomy and Biomechanics Level IIIDocument23 pagesThorax: Thoracic Spine Anatomy and Biomechanics Level IIIAnonymous ecI8GUbaNo ratings yet
- Comparison of Moist Exposed Burn Ointment (MEBO) With Silver Sulfadiazine (Ag-S) For The Treatment of Deep Burn InjuryDocument89 pagesComparison of Moist Exposed Burn Ointment (MEBO) With Silver Sulfadiazine (Ag-S) For The Treatment of Deep Burn InjuryElis Sri AlawiyahNo ratings yet
- Physical Therapy Protocols For Conditions of Thorax RegionDocument52 pagesPhysical Therapy Protocols For Conditions of Thorax RegionVytautas PilelisNo ratings yet
- A Fighter's Lines by Marzuki AliDocument5 pagesA Fighter's Lines by Marzuki AliAnonymous TADs3BevnNo ratings yet
- MotionquadDocument4 pagesMotionquadapi-279506854No ratings yet
- 2012 Bars ManualDocument12 pages2012 Bars Manual12378aNo ratings yet
- Was There Ever A Time in Your Life When You Had A Strong Fear ofDocument58 pagesWas There Ever A Time in Your Life When You Had A Strong Fear ofark1974No ratings yet
- Fballi Ho-1Document5 pagesFballi Ho-1isaiah bungalsoNo ratings yet
- Dr. Darryl Auston Joins OrthoONE at North Suburban Medical CenterDocument3 pagesDr. Darryl Auston Joins OrthoONE at North Suburban Medical CenterPR.comNo ratings yet
- Cesar Issac vs. A.L. Ammen TransportationDocument1 pageCesar Issac vs. A.L. Ammen TransportationEarl LarroderNo ratings yet
- Anatomy of The Face and Neck: Peter M. PrendergastDocument18 pagesAnatomy of The Face and Neck: Peter M. PrendergastPaul SalahoruNo ratings yet
- Death in Relation To Torts - LawDocument4 pagesDeath in Relation To Torts - Lawvawuku2003No ratings yet
- 207R Datasheet - FBE Rough OvercoatingDocument2 pages207R Datasheet - FBE Rough Overcoatingbello imamNo ratings yet
- Detailed Health History: PneumoniaDocument6 pagesDetailed Health History: PneumoniaBakushido100% (2)
- Intracranial AneurysmDocument5 pagesIntracranial AneurysmSarah Eddiah0% (1)
- Right Inguinal Hernia RepairDocument1 pageRight Inguinal Hernia Repairsgod34No ratings yet