Download as docx, pdf, or txt
You might also like
- NUR3111 Post-Lecture QuizDocument28 pagesNUR3111 Post-Lecture QuizliNo ratings yet
- 2021 AHA ASA Guideline For The Prevention of Stroke in Patients With Stroke and TIA Clinical UpdateDocument43 pages2021 AHA ASA Guideline For The Prevention of Stroke in Patients With Stroke and TIA Clinical Updatejulioel1nico20100% (1)
- ET Tube Care, Tracheostomy CareDocument24 pagesET Tube Care, Tracheostomy CaretelilingNo ratings yet
- Portable VentilatorDocument31 pagesPortable VentilatorAshikin AriNo ratings yet
- The Effect of Structured Teaching Program On Knowledge About Arterial Blood Gas Analysis Among The Staff Nurses Working in Critical Care UnitDocument7 pagesThe Effect of Structured Teaching Program On Knowledge About Arterial Blood Gas Analysis Among The Staff Nurses Working in Critical Care UnitIJAR JOURNALNo ratings yet
- OP PoisoningDocument14 pagesOP PoisoningAnmol KudalNo ratings yet
- AHA For PregnancyDocument77 pagesAHA For PregnancyAndrew TimantaNo ratings yet
- Care of Patients With Chest TubesDocument2 pagesCare of Patients With Chest Tubesaurezea100% (1)
- Acute Coronary Syndromes AlgorithmDocument1 pageAcute Coronary Syndromes AlgorithmRed JimenoNo ratings yet
- Planning An Operation Theatre ComplexDocument4 pagesPlanning An Operation Theatre ComplexRaviraj PisheNo ratings yet
- Cost EffectivenessDocument22 pagesCost EffectivenessEdalyn CapiliNo ratings yet
- Definition of Professional NursingDocument2 pagesDefinition of Professional NursingQuenz OstiaNo ratings yet
- Classification of Congenital Heart DiseaseDocument1 pageClassification of Congenital Heart DiseaseClaudia SanchezNo ratings yet
- DIC - RLE #4 For HemaDocument12 pagesDIC - RLE #4 For HemaApril Mae Magos LabradorNo ratings yet
- Burn CareDocument3 pagesBurn CareRafaela LennyNo ratings yet
- Pre Anaesthetic Check-UpDocument4 pagesPre Anaesthetic Check-UpUdoy PaulNo ratings yet
- Monitoring in Operation TheatreDocument12 pagesMonitoring in Operation TheatreJunaid ebrahimNo ratings yet
- Management of The EVDDocument7 pagesManagement of The EVDplethoraldork100% (1)
- Modified Early Warning Score (MEWS) Observation Chart: Clinical ProtocolDocument4 pagesModified Early Warning Score (MEWS) Observation Chart: Clinical ProtocolElena DolcanNo ratings yet
- Acls AnpDocument20 pagesAcls AnpNirupama KsNo ratings yet
- 15Document21 pages15Tyson Easo JonesNo ratings yet
- Admission and EmergencyDocument12 pagesAdmission and EmergencyRashid AyubiNo ratings yet
- Intravenous CannulationDocument9 pagesIntravenous CannulationjeorjNo ratings yet
- Ventilator, Weaning, SuctioningDocument81 pagesVentilator, Weaning, SuctioningwaqarNo ratings yet
- Care of Patient With TPM Slide PresentationDocument16 pagesCare of Patient With TPM Slide PresentationirzehronNo ratings yet
- Ed Assessment Tool SampleDocument28 pagesEd Assessment Tool SampleAnonymous ibmeej9No ratings yet
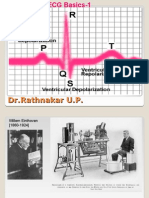
- ECG Basics 1Document24 pagesECG Basics 1Dr.U.P.Rathnakar.MD.DIH.PGDHMNo ratings yet
- Renal TransplantationDocument50 pagesRenal Transplantationregie cuaresmaNo ratings yet
- Common EmergenciesDocument29 pagesCommon EmergenciesVIRUPAKSHA KOOLINo ratings yet
- Epistaxis: Presenter: Elesia Powell-WilliamsDocument46 pagesEpistaxis: Presenter: Elesia Powell-Williamselesia powellNo ratings yet
- Instillation of Normal Saline in Endotracheal SuctioningDocument2 pagesInstillation of Normal Saline in Endotracheal SuctioningChiyouaLoverz Tharaztic JRsNo ratings yet
- Tele MedicineDocument34 pagesTele MedicineKiran DuggarajuNo ratings yet
- Advanced Airway Care: Intensive Care Unit PerspectiveDocument42 pagesAdvanced Airway Care: Intensive Care Unit PerspectiveJeffery Samuel100% (1)
- 208-Audit Checklist-Autoclave Operation - FinalDocument6 pages208-Audit Checklist-Autoclave Operation - FinalCherry Hope MistioNo ratings yet
- Adrenal CrisisDocument6 pagesAdrenal CrisisSteven SetioNo ratings yet
- CPR - Cardiopulmonary ResuscitationDocument31 pagesCPR - Cardiopulmonary ResuscitationPanji HerlambangNo ratings yet
- Guidline of Management of Porta CathDocument8 pagesGuidline of Management of Porta CathroncekeyNo ratings yet
- OT Equipments: Hold The Highest Standard With Best Pieces of EquipmentsDocument71 pagesOT Equipments: Hold The Highest Standard With Best Pieces of Equipmentsradhika333100% (1)
- Exercise Stress TestingDocument18 pagesExercise Stress TestingSereinNo ratings yet
- Report of Departmental Study On Ot Complex: ObjectivesDocument52 pagesReport of Departmental Study On Ot Complex: Objectivesvvvvtusebt100% (1)
- Drug Heart Failure MDocument24 pagesDrug Heart Failure MAthari KhanNo ratings yet
- Early Warning Scoring System (Unit 9) - 1Document6 pagesEarly Warning Scoring System (Unit 9) - 1Zharlene PadillaNo ratings yet
- College of Medicine and Health Sciences: For Public Health C-I StudentsDocument29 pagesCollege of Medicine and Health Sciences: For Public Health C-I StudentsWĩž BŕëãžÿNo ratings yet
- Shubha Clilical RotationDocument3 pagesShubha Clilical Rotationshubha jeniferNo ratings yet
- Triage in Disaster ManagementDocument10 pagesTriage in Disaster ManagementHazel Mei MalvarNo ratings yet
- Neb Ul Ization 2Document31 pagesNeb Ul Ization 2RegineJoyCarinoNo ratings yet
- 3 - Transfer of Unstable PatientDocument7 pages3 - Transfer of Unstable PatientShailendra SinghNo ratings yet
- Documenting ConferringDocument40 pagesDocumenting ConferringDidik Atmojo0% (1)
- Plasma P Here SisDocument13 pagesPlasma P Here SisSampath GoudNo ratings yet
- Instruments and Equipment For Labour RoomDocument3 pagesInstruments and Equipment For Labour RoomHerrero, Donna Bhel A.No ratings yet
- ShockDocument63 pagesShockAhmedNo ratings yet
- Pulmonary Function Tests ScribdDocument34 pagesPulmonary Function Tests ScribdNamita JadhaoNo ratings yet
- Hospital: Ms .Neethu Vincent Asst Professor KVM College of NursingDocument29 pagesHospital: Ms .Neethu Vincent Asst Professor KVM College of NursingNeethu VincentNo ratings yet
- Family Nursing and Home NursingDocument35 pagesFamily Nursing and Home NursingSamjhana Neupane100% (1)
- Care of Patient On I C DDocument15 pagesCare of Patient On I C DGeorge John Jeelu SusanNo ratings yet
- Anesthesiology Pre-Op Evaluation: ExovsrtsDocument1 pageAnesthesiology Pre-Op Evaluation: Exovsrtssabbo morsNo ratings yet
- Protocol For The Management of Choking in AdultsDocument3 pagesProtocol For The Management of Choking in AdultsSarinah RynaNo ratings yet
- Centrel Venous CatheterizationDocument77 pagesCentrel Venous CatheterizationAli100% (1)
- Holter Monitor: 'Ambulatory Electrocardiography Device''Document22 pagesHolter Monitor: 'Ambulatory Electrocardiography Device''Rachel PeredaNo ratings yet
- The COAT & Review Approach: How to recognise and manage unwell patientsFrom EverandThe COAT & Review Approach: How to recognise and manage unwell patientsRating: 5 out of 5 stars5/5 (1)
- The Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesFrom EverandThe Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesNo ratings yet
- Anaesthetic Implications in A Patient With Poor LV Function by DR Sanjula VirmaniDocument39 pagesAnaesthetic Implications in A Patient With Poor LV Function by DR Sanjula VirmanicardiacanesthesiaNo ratings yet
- ICU Lines TubesDocument7 pagesICU Lines TubesCindy MurphyNo ratings yet
- (JURNAL, Eng) A Retrospective Cohort Review of Prescribing in Hospitalised Patients With Heart Failure Using Beers Criteria and STOPP RecommendationsDocument7 pages(JURNAL, Eng) A Retrospective Cohort Review of Prescribing in Hospitalised Patients With Heart Failure Using Beers Criteria and STOPP RecommendationsAurellia Annisa WulandariNo ratings yet
- Staff Training PowerpointDocument12 pagesStaff Training Powerpointapi-282305740No ratings yet
- Nababaliw Na Ako Sa Drug StudyDocument52 pagesNababaliw Na Ako Sa Drug StudyKate Husslein ErumNo ratings yet
- APRV VentilationDocument5 pagesAPRV VentilationIrina UngureanuNo ratings yet
- The Ecg Made Practical 7Th Edition John Hampton Full ChapterDocument67 pagesThe Ecg Made Practical 7Th Edition John Hampton Full Chapterjohn.staten431100% (8)
- Chap 18 Body Fluids and Circulation Mind Map Class 11 PDF - WatermarkDocument3 pagesChap 18 Body Fluids and Circulation Mind Map Class 11 PDF - Watermarkmominameen7No ratings yet
- Diagnosis and Management of Transient Ischemic.10-1Document11 pagesDiagnosis and Management of Transient Ischemic.10-1Cristina GhizdavetNo ratings yet
- Uterine Sarcoma - Pharmacologic Management - Cancer Therapy AdvisorDocument32 pagesUterine Sarcoma - Pharmacologic Management - Cancer Therapy AdvisorIrfan FathurrahmanNo ratings yet
- Arrows Consele PDFDocument221 pagesArrows Consele PDFIsai Lara OsoriaNo ratings yet
- Adachi Autopsy ReportDocument25 pagesAdachi Autopsy ReportMissionLocalNo ratings yet
- Role of glycerol-3-phosphate phosphatase (G3PP) in pancreatic β-cells and liverDocument220 pagesRole of glycerol-3-phosphate phosphatase (G3PP) in pancreatic β-cells and liverNicolas de andreisNo ratings yet
- Doze FarmaDocument1 pageDoze FarmaCorina MunteanuNo ratings yet
- Fellowship Medical RetinaDocument5 pagesFellowship Medical RetinaThe Doctor's InterestsNo ratings yet
- PUBlic Challenges An Extended Stay ASSIGN 1Document7 pagesPUBlic Challenges An Extended Stay ASSIGN 1Areesha KaleemNo ratings yet
- PMLS 2 Lesson 7Document3 pagesPMLS 2 Lesson 7Jam LozanoNo ratings yet
- Epithelial Tissues MnemonicsDocument3 pagesEpithelial Tissues MnemonicsDaniel AyanlekeNo ratings yet
- Pathophysiology The Biologic Basis For Disease in Adults and Children 5th Edition Huether Mccance Test BankDocument8 pagesPathophysiology The Biologic Basis For Disease in Adults and Children 5th Edition Huether Mccance Test BankHarry Coston100% (38)
- 1.5A Copd: OutlineDocument12 pages1.5A Copd: OutlineCecille Ann Cayetano100% (1)
- APPICON AbstractsDocument1 pageAPPICON Abstractssaumya.sharmaNo ratings yet
- Textbook of MedicineDocument198 pagesTextbook of MedicineSoumyadip pradhanNo ratings yet
- Ecg 1Document5 pagesEcg 1Hêny CarlênicNo ratings yet
- Local Exam 5Document68 pagesLocal Exam 5drnasir31No ratings yet
- Annotated Bibliograhy: Submitted ToDocument4 pagesAnnotated Bibliograhy: Submitted ToRumela Ganguly ChakrabortyNo ratings yet
- GlaucomaDocument20 pagesGlaucomaandrema123No ratings yet
- Emergencies in Dental Clinic: How To DealDocument94 pagesEmergencies in Dental Clinic: How To DealhassonamonaNo ratings yet
- OnePlan BookletDocument40 pagesOnePlan BookletStelian IanaNo ratings yet