Download as pdf or txt
You might also like
- FLCCC Alliance I RECOVER Management Protocol For Long Haul COVID 19 SyndromeDocument3 pagesFLCCC Alliance I RECOVER Management Protocol For Long Haul COVID 19 SyndromeAizaz ul HaqNo ratings yet
- FLCCC Alliance's I RECOVER Management Protocol For Long Haul COVID 19 SyndromeDocument3 pagesFLCCC Alliance's I RECOVER Management Protocol For Long Haul COVID 19 SyndromeAlan N100% (1)
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesFrom EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesRating: 4 out of 5 stars4/5 (3)
- Drug Study23Document2 pagesDrug Study23Joh Acedo BantingNo ratings yet
- Antimycobacterial Drugs: Camille E. Beauduy, Pharmd, & Lisa G. Winston, MDDocument17 pagesAntimycobacterial Drugs: Camille E. Beauduy, Pharmd, & Lisa G. Winston, MDRegine Coeli Menta LansanganNo ratings yet
- SMILEPEG HEM TCell ADocument5 pagesSMILEPEG HEM TCell Aphillip.chung89No ratings yet
- Kidney Protocol ImmunosuppressionDocument16 pagesKidney Protocol ImmunosuppressionmsreyaNo ratings yet
- Treatment: Chapter 67: TuberculosisDocument3 pagesTreatment: Chapter 67: TuberculosisNina MarlinaNo ratings yet
- Drug StudyDocument5 pagesDrug StudyinjilbalazoNo ratings yet
- Adult Patient Diagnosed With COVID-19: Ministry of Health & Family Welfare, Government of IndiaDocument1 pageAdult Patient Diagnosed With COVID-19: Ministry of Health & Family Welfare, Government of Indiapramodbankhele3845No ratings yet
- Hiv Current Trend in The Use of HaartDocument19 pagesHiv Current Trend in The Use of Haartapi-3705046No ratings yet
- MSHS Treatment Guidelines COVIDDocument4 pagesMSHS Treatment Guidelines COVIDFrancisco MuñozNo ratings yet
- Guidance For Treatment of Covid-19 in Adults and Children: Patient PopulationDocument7 pagesGuidance For Treatment of Covid-19 in Adults and Children: Patient PopulationonkarratheeNo ratings yet
- ELIQUIS HCP Electronic Combo Dosing Guide - Desktop PDFDocument29 pagesELIQUIS HCP Electronic Combo Dosing Guide - Desktop PDFAndreea Livia DumitrescuNo ratings yet
- AIIMS Issues New Guidelines For Treatment of Covid-19 Cases: (Enter Post Title Here)Document7 pagesAIIMS Issues New Guidelines For Treatment of Covid-19 Cases: (Enter Post Title Here)senthil kumarNo ratings yet
- Ambrisentan: Jamie D. Croxtall and Susan J. KeamDocument10 pagesAmbrisentan: Jamie D. Croxtall and Susan J. KeamElden Kyle BillonesNo ratings yet
- Assess The Patient If They Have Any Allergy To Ketoconazole, Fungal Meningitis, Hepatic Failure, Pregnancy, Lactation, Also in Physical ReactionDocument2 pagesAssess The Patient If They Have Any Allergy To Ketoconazole, Fungal Meningitis, Hepatic Failure, Pregnancy, Lactation, Also in Physical ReactionJane Decenine CativoNo ratings yet
- Pediatric Guidelines: Head and Neck Infections - MastoiditisDocument3 pagesPediatric Guidelines: Head and Neck Infections - MastoiditisJr SparkNo ratings yet
- AIIMS Issues New Guidelines For Treatment of CovidDocument7 pagesAIIMS Issues New Guidelines For Treatment of Covidsenthil kumarNo ratings yet
- Dosing Guide Xarelto Effective Protection Indications Worldwide 09 2018Document26 pagesDosing Guide Xarelto Effective Protection Indications Worldwide 09 2018Antonia AdinaNo ratings yet
- See Full Prescribing Information For Complete Boxed Warning: WWW - Fda.gov/medwatchDocument32 pagesSee Full Prescribing Information For Complete Boxed Warning: WWW - Fda.gov/medwatchQF Fredii Anthony GutyNo ratings yet
- Deep Vein ThrombosisDocument4 pagesDeep Vein ThrombosisStefania CristinaNo ratings yet
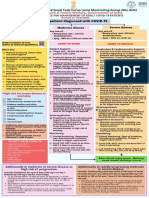
- COVID19 Management Algorithm 22042021 v1Document1 pageCOVID19 Management Algorithm 22042021 v1shivani shindeNo ratings yet
- WB Covid Protocol Book 25.09 .20 (1)Document49 pagesWB Covid Protocol Book 25.09 .20 (1)El MirageNo ratings yet
- Generic Name Brand Name Classification Indication / Dosage Adverse Effect Contraindication Nursing ConsiderationDocument5 pagesGeneric Name Brand Name Classification Indication / Dosage Adverse Effect Contraindication Nursing ConsiderationHazel Ann MolinoNo ratings yet
- Final Haad (DOH) ExamDocument9 pagesFinal Haad (DOH) ExamsenthamizhselvanNo ratings yet
- Inpatient Guidance For Treatment of Covid-19 in Adults and ChildrenDocument7 pagesInpatient Guidance For Treatment of Covid-19 in Adults and ChildrenAmogh KurianNo ratings yet
- Suspected COVID-19 Cases Management in Triage HospitalsDocument6 pagesSuspected COVID-19 Cases Management in Triage HospitalsMuhamed RamadanNo ratings yet
- VeIP GU TESDocument6 pagesVeIP GU TESMohan KumarNo ratings yet
- Summary of Product Characteristics: 4.1 Therapeutic IndicationsDocument11 pagesSummary of Product Characteristics: 4.1 Therapeutic IndicationsAninditaSahaNo ratings yet
- ICE DrugsDocument2 pagesICE DrugsRichelle FrondaNo ratings yet
- New May2020 PDFDocument7 pagesNew May2020 PDFDoctorMoodyNo ratings yet
- MethylprednisoloneDocument4 pagesMethylprednisoloneadryananestesiNo ratings yet
- PCP Treatment GeneralDocument1 pagePCP Treatment GeneralLegolas gantengNo ratings yet
- Leukemia Treatment Regimens 7937Document3 pagesLeukemia Treatment Regimens 7937Irfan FathurrahmanNo ratings yet
- ParacetamolDocument3 pagesParacetamolheven myhomeNo ratings yet
- MMC Adult COVID 19 Treatment 3202020Document7 pagesMMC Adult COVID 19 Treatment 3202020Nidal RakanNo ratings yet
- SHC Heme Onc Antimicrobial ProphylaxisDocument4 pagesSHC Heme Onc Antimicrobial ProphylaxisTala MahmoudNo ratings yet
- VancomycinDocument1 pageVancomycinJUSTINE ALLYSA MAY CASTILLONo ratings yet
- COVID 19 TreatmentDocument8 pagesCOVID 19 TreatmentCWS ScapeNo ratings yet
- Drugs That Require Loading Doses Table FinalDocument1 pageDrugs That Require Loading Doses Table Finalandirio7486No ratings yet
- Direct Oral Anticoagulants (DOACs) For Treatment of DVTDocument11 pagesDirect Oral Anticoagulants (DOACs) For Treatment of DVTLuana MNo ratings yet
- Material, Vincent M. (Types of Anesthesia Used in Cesarean Section)Document22 pagesMaterial, Vincent M. (Types of Anesthesia Used in Cesarean Section)Vincent Maralit MaterialNo ratings yet
- 30 Glycopeptides Vancomycin and Teicoplanin 2015 Mandell Douglas and BDocument29 pages30 Glycopeptides Vancomycin and Teicoplanin 2015 Mandell Douglas and BHelen DyNo ratings yet
- Drugs Acting On Immune SystemDocument6 pagesDrugs Acting On Immune SystemSORENI SORENINo ratings yet
- How To RecoverDocument3 pagesHow To RecoverSterr LiingNo ratings yet
- COVID-19 Therapeutic Guidance COVID-19 Therapeutic Guidance COVID-19 Therapeutic GuidanceDocument1 pageCOVID-19 Therapeutic Guidance COVID-19 Therapeutic Guidance COVID-19 Therapeutic GuidanceAbdullah KhanNo ratings yet
- Doacs For VteDocument10 pagesDoacs For VteAhmed MohammedNo ratings yet
- Management of CAP in Adults - Ontario GovernmentDocument2 pagesManagement of CAP in Adults - Ontario GovernmentSukhvir AujlaNo ratings yet
- Domperidone Supps LeafletDocument1 pageDomperidone Supps LeafletABDULJWAD HADDADNo ratings yet
- Drug Study of TBDocument7 pagesDrug Study of TBMarc AntonioNo ratings yet
- Escalation Guide For Gram-Negative Bacteremia StanfordDocument3 pagesEscalation Guide For Gram-Negative Bacteremia StanfordLuis MedinaNo ratings yet
- Covid Drug TherapyDocument35 pagesCovid Drug TherapyNandha KumarNo ratings yet
- Denosumab-12mg Per 1.7ml Single Use Vial InjectionDocument10 pagesDenosumab-12mg Per 1.7ml Single Use Vial InjectionMd. Abdur RahmanNo ratings yet
- Early Treatment Information For Doctors Updated 11042022Document4 pagesEarly Treatment Information For Doctors Updated 11042022han tianNo ratings yet
- Chapter 11 PharmacogenomicsDocument2 pagesChapter 11 PharmacogenomicsDrashtibahen PatelNo ratings yet
- Targocid Article 30 Referral Annex III - enDocument32 pagesTargocid Article 30 Referral Annex III - enDR JAMAL WARISNo ratings yet
- FluticasoneDocument3 pagesFluticasoneAmberNo ratings yet
- Critical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsNo ratings yet
- Blood Grouping Reagents: (Murine Monoclonal)Document10 pagesBlood Grouping Reagents: (Murine Monoclonal)Roshan KashyapNo ratings yet
- OSHA 2232 - Longshoring IndustryDocument291 pagesOSHA 2232 - Longshoring IndustryWahed Mn ElnasNo ratings yet
- Food Drugs and Chemical Substances CAP 254, Revised Edition 2012Document19 pagesFood Drugs and Chemical Substances CAP 254, Revised Edition 2012Janet NjorogeNo ratings yet
- In The Court of Appeal of The Democratic Socialist Republic of Sri LankaDocument13 pagesIn The Court of Appeal of The Democratic Socialist Republic of Sri LankaMalith DhananjayaNo ratings yet
- Friedreich 'S Ataxia: Clinical Features, Pathogenesis and ManagementDocument12 pagesFriedreich 'S Ataxia: Clinical Features, Pathogenesis and ManagementVaibhav BhatiaNo ratings yet
- PDFDocument28 pagesPDFlikun mishra0% (1)
- WWW Medindia Net Patients Lifestyleandwellness Curry LeavesDocument22 pagesWWW Medindia Net Patients Lifestyleandwellness Curry LeaveskartikkeyyanNo ratings yet
- Torrington Emergency Management Director Job DescriptionDocument3 pagesTorrington Emergency Management Director Job DescriptionRepublican-AmericanNo ratings yet
- Clinton Email Batch 2Document743 pagesClinton Email Batch 2DavidKihara100% (1)
- Mosh RoomDocument21 pagesMosh RoomBrandon DishmanNo ratings yet
- Material Safety Data Sheet: Product IdentificationDocument4 pagesMaterial Safety Data Sheet: Product Identificationمحمد عزتNo ratings yet
- Process Safety ManagementDocument9 pagesProcess Safety ManagementDeepak Kumar100% (3)
- Water Quality AnalysisDocument33 pagesWater Quality AnalysisksbbsNo ratings yet
- Virus Influenza Guidlines PDFDocument47 pagesVirus Influenza Guidlines PDFМарија СерафимовскаNo ratings yet
- DMSO Health and Safety InformationDocument16 pagesDMSO Health and Safety InformationPapaindoNo ratings yet
- Seers+servicemanual+ +genereltDocument143 pagesSeers+servicemanual+ +genereltdianNo ratings yet
- Lapkin Dini Feb 2023Document10 pagesLapkin Dini Feb 2023s6fjfw77v7No ratings yet
- Master The Habit Loop To Break Bad Habits and Build Better OnesDocument11 pagesMaster The Habit Loop To Break Bad Habits and Build Better OnesSenarath BandaraNo ratings yet
- Food and Nutrition PoliciesDocument54 pagesFood and Nutrition PoliciesDawud AsnakewNo ratings yet
- A Retrospectie Study of Cranial Strain Patterns in Patients With Idiopathic Parkinson's DiseaseDocument6 pagesA Retrospectie Study of Cranial Strain Patterns in Patients With Idiopathic Parkinson's DiseaserafaelNo ratings yet
- ORGDEV CH 13 Employee InvolvementDocument13 pagesORGDEV CH 13 Employee InvolvementAmy BCNo ratings yet
- A Case Study On Arav in D Eye Care SystemsDocument4 pagesA Case Study On Arav in D Eye Care SystemsSaugatoDuttoNo ratings yet
- Advance Care Planning, Palliative Care, and End-Of-Life Care Interventions For Homeless People: A Systematic ReviewDocument11 pagesAdvance Care Planning, Palliative Care, and End-Of-Life Care Interventions For Homeless People: A Systematic Reviewelver galargaNo ratings yet
- Prevalence and Associated Risk Factors of Sepsis Among Neonates Admitted Into Neonatal Intensive Care Units of Public Hospitals in DhakaDocument12 pagesPrevalence and Associated Risk Factors of Sepsis Among Neonates Admitted Into Neonatal Intensive Care Units of Public Hospitals in DhakaAnonymous SMLzNANo ratings yet
- Nutrilan Keratin OPP - BASF NewDocument1 pageNutrilan Keratin OPP - BASF NewWilliam Davila GuerraNo ratings yet
- Soal MCQ Blok 16Document14 pagesSoal MCQ Blok 16Mira Pandora100% (1)
- Psychosocial TheoryDocument13 pagesPsychosocial Theoryapi-433239461No ratings yet
- Confined Space TrainingDocument18 pagesConfined Space Trainingmortadha husainNo ratings yet
- JKSMRM 18 151 1 PDFDocument6 pagesJKSMRM 18 151 1 PDFMcj MirandaNo ratings yet