Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Curvas Parálisis Cerebral Brooks 2011Document36 pagesCurvas Parálisis Cerebral Brooks 2011veronicaNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Black Book of Strength - Andy BoltonDocument49 pagesThe Black Book of Strength - Andy BoltonGawen100% (3)
- Comprehensive Textbook of Echocardiography Volume 1 PDFDocument1,174 pagesComprehensive Textbook of Echocardiography Volume 1 PDFAlina Badulescu100% (10)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Good Manufacturing Practices PolicyDocument3 pagesGood Manufacturing Practices PolicyJon Mark100% (1)
- MN Thesis Stream Progress ReportDocument4 pagesMN Thesis Stream Progress ReportFarhana AnuarNo ratings yet
- SPE 86863 Health Risk Assessment in Oil and Gas Exploration: Siesmic WorkDocument6 pagesSPE 86863 Health Risk Assessment in Oil and Gas Exploration: Siesmic WorkWaleed Barakat MariaNo ratings yet
- Microbiological Enviromental MonitoringDocument34 pagesMicrobiological Enviromental MonitoringAna Dulce100% (1)
- Pneumoperitoneum: Abdominal X-Rays Made Easy. 2nd Edition, James D. BeggDocument30 pagesPneumoperitoneum: Abdominal X-Rays Made Easy. 2nd Edition, James D. BeggFaizal AzizNo ratings yet
- Thosai FermentationDocument15 pagesThosai FermentationVithyia Murugiah100% (1)
- Organic Chemistry Lab Independent Project ProposalDocument8 pagesOrganic Chemistry Lab Independent Project Proposalapi-281150432No ratings yet
- Model Test 4 Reading Passage 1 One Hundred Days of Reform: Reformer in Control of The GovernmentDocument5 pagesModel Test 4 Reading Passage 1 One Hundred Days of Reform: Reformer in Control of The GovernmentphuongthaospkNo ratings yet
- Reckitt Benckiser - Original PrateekDocument55 pagesReckitt Benckiser - Original PrateekGovind Bisht100% (2)
- Aerial Lift TrainingDocument81 pagesAerial Lift TrainingCesar Augusto Vera JaimesNo ratings yet
- National Nutrition Strategy and Action PlanDocument97 pagesNational Nutrition Strategy and Action PlanBglpoo OfficerNo ratings yet
- Edited PPT HEALTH 4th (Autosaved)Document23 pagesEdited PPT HEALTH 4th (Autosaved)Chloe Belamare JaplitNo ratings yet
- Soffit and PCD PDFDocument4 pagesSoffit and PCD PDFKalpanaNo ratings yet
- Mysthenia Gravis DR NajeebDocument11 pagesMysthenia Gravis DR NajeebJay kumarNo ratings yet
- Canadian Red Cross Business Development StrategyDocument14 pagesCanadian Red Cross Business Development StrategyMonu BhagatNo ratings yet
- PHCT Lec Topic 1Document3 pagesPHCT Lec Topic 1armand bayoranNo ratings yet
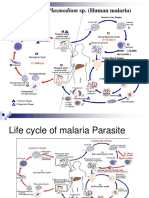
- The Life Cycle & The Transmission Dynamic Versi 1Document14 pagesThe Life Cycle & The Transmission Dynamic Versi 1rayNo ratings yet
- Tio2mesh Flyer A4 4seitig Englisch 2016-09Document2 pagesTio2mesh Flyer A4 4seitig Englisch 2016-09Erik CanosNo ratings yet
- Childhood EssayDocument3 pagesChildhood EssayAddison CharlletNo ratings yet
- 2-Hyperprolinemia As A Clue in The Diagnosis of A Patientwith Psychiatric ManifestationsDocument3 pages2-Hyperprolinemia As A Clue in The Diagnosis of A Patientwith Psychiatric ManifestationsAli Emre KöseNo ratings yet
- MRSA BookDocument228 pagesMRSA BookIgd Pondok TjandraNo ratings yet
- Noticias 1368018543 PDFDocument14 pagesNoticias 1368018543 PDFdrzana78No ratings yet
- CLF 12 Preparatory-Learning-Activity - JHSDocument6 pagesCLF 12 Preparatory-Learning-Activity - JHSUSJRBALAMBAN JUNIOR HIGH SCHOOLNo ratings yet
- Introduction To Medicine PDFDocument15 pagesIntroduction To Medicine PDFTATYNo ratings yet
- Un Pan 92431Document12 pagesUn Pan 92431Farid HilmiNo ratings yet
- 2 Cholinergic BlockersDocument49 pages2 Cholinergic BlockersAmanuel MaruNo ratings yet
- PM&QS Capability Statement - GSKDocument58 pagesPM&QS Capability Statement - GSKcollincucNo ratings yet