
Bacterial Skin Infections
Bacterial Skin Infections
You might also like
- Wound Types Poster For ReviewDocument1 pageWound Types Poster For Reviewapi-702908151No ratings yet
- Case Summary Pediatrics32 5-Year-ODocument12 pagesCase Summary Pediatrics32 5-Year-OMaryam FadahNo ratings yet
- Khawater Makki Cover Letter.ADocument1 pageKhawater Makki Cover Letter.AAnonymous miK3qJxNo ratings yet
- VATS Bypass ModuleDocument3 pagesVATS Bypass ModuleSHOOTEENo ratings yet
- White Pony - DeftonesDocument7 pagesWhite Pony - DeftonesAarón Espinosa GarcíaNo ratings yet
- Bacterial Skin Infections: Basic Dermatology CurriculumDocument78 pagesBacterial Skin Infections: Basic Dermatology CurriculumAnthony Bravo CortezNo ratings yet
- Bacterial Skin Infections: Basic Dermatology CurriculumDocument75 pagesBacterial Skin Infections: Basic Dermatology CurriculummasithaNo ratings yet
- Integumentry PDFDocument17 pagesIntegumentry PDFMehul RathoreNo ratings yet
- Integumentry Dermatitis Bacterial Impetigo Cellulitis Abscess DefDocument17 pagesIntegumentry Dermatitis Bacterial Impetigo Cellulitis Abscess DefMehul RathoreNo ratings yet
- Skinlesionsteam 5Document33 pagesSkinlesionsteam 5Noemí TorresNo ratings yet
- 17 Epidermal New GrowthsDocument3 pages17 Epidermal New GrowthsWaiwit KritayakiranaNo ratings yet
- History and Epidemiology: Key FeaturesDocument8 pagesHistory and Epidemiology: Key FeaturesAswin KrishnaNo ratings yet
- AnnexIII DifferentialDiagnosis FromNLEP India PDFDocument3 pagesAnnexIII DifferentialDiagnosis FromNLEP India PDFAegirine RafilahNo ratings yet
- Eczema& Allergic Contact-DermatitisDocument70 pagesEczema& Allergic Contact-Dermatitisamraayman21No ratings yet
- ICD TableDocument1 pageICD TableJo CanensNo ratings yet
- Diagnosis and Management of Tinea Infections: Am Fam Physician. 2014 Nov 15 90 (10) :702-711Document20 pagesDiagnosis and Management of Tinea Infections: Am Fam Physician. 2014 Nov 15 90 (10) :702-711'rha' Ittuu IrraaNo ratings yet
- Skin Condition TableDocument3 pagesSkin Condition TableELI GOZONNo ratings yet
- Disorders of The Integumentary System: Internet ResourcesDocument4 pagesDisorders of The Integumentary System: Internet ResourcesDylan Dela CruzNo ratings yet
- Skin, Hair and Nails Ok - CompressedDocument67 pagesSkin, Hair and Nails Ok - CompressedFelya Elsa Pratiwi KurniaNo ratings yet
- Arterial, Venous, Lymph EdemaDocument2 pagesArterial, Venous, Lymph EdemapallenNo ratings yet
- Derm LOsDocument37 pagesDerm LOskatherine nunnNo ratings yet
- Skin Disorders 4-2-08Document14 pagesSkin Disorders 4-2-08api-3822433No ratings yet
- Handout2 - Major Clinical Features of Genital UlcersDocument1 pageHandout2 - Major Clinical Features of Genital Ulcersgdudex118811No ratings yet
- PsoriasisDocument27 pagesPsoriasisNikkaDablioNo ratings yet
- Dermatology ConditionsDocument8 pagesDermatology ConditionsmeilunlyNo ratings yet
- Shanz - PEDIA II 2.01 NEWDocument8 pagesShanz - PEDIA II 2.01 NEWPetrina XuNo ratings yet
- Derm ChartDocument109 pagesDerm ChartAlana BolloneNo ratings yet
- Wound ManagementDocument6 pagesWound ManagementBianca Corina MusatNo ratings yet
- Skin and Body Membranes For AnaPhyDocument3 pagesSkin and Body Membranes For AnaPhyJASHEL M. CASTANARESNo ratings yet
- Med1 Skin Hair and NailsDocument15 pagesMed1 Skin Hair and NailsCathleen KirstenNo ratings yet
- Slide 11-17 by Ur BabyDocument6 pagesSlide 11-17 by Ur Babyfeloniacarl34No ratings yet
- Bacterial Skin InfectionsDocument9 pagesBacterial Skin InfectionskateverdadNo ratings yet
- JwillzDocument14 pagesJwillzWyatt WarawaNo ratings yet
- Skin Examination 1Document9 pagesSkin Examination 1Marry JuttNo ratings yet
- Male Genital DermDocument112 pagesMale Genital DermVũ CaoNo ratings yet
- Diabetic Foot Hajera FinalDocument38 pagesDiabetic Foot Hajera FinalAfifah SelamatNo ratings yet
- UlcerDocument3 pagesUlcerMd Ahsanuzzaman PinkuNo ratings yet
- Herpes Zoster: Iqbal Ainn Un A. Tutor 23Document21 pagesHerpes Zoster: Iqbal Ainn Un A. Tutor 23inunNo ratings yet
- Type of The Wound-JCF 4thDocument25 pagesType of The Wound-JCF 4thTaufik HidayantoNo ratings yet
- Triage: A - Raf B - Kath C - Cara D - Cesca E - Kyla F - Michelle G - AndreDocument4 pagesTriage: A - Raf B - Kath C - Cara D - Cesca E - Kyla F - Michelle G - AndreLeira BarbosaNo ratings yet
- PsoriasisDocument23 pagesPsoriasisvasavavipul38022No ratings yet
- Internal Medicine Finals ReviewerDocument8 pagesInternal Medicine Finals ReviewerRojales FrancisNo ratings yet
- Psoriasis Management in The Community: BY DR U.B.Buhari Gpwer FRCGP MHADocument50 pagesPsoriasis Management in The Community: BY DR U.B.Buhari Gpwer FRCGP MHAEng Abdikariim AbdillahiNo ratings yet
- Cause and PathogenesisDocument11 pagesCause and Pathogenesiswanaibor RyngksaiNo ratings yet
- Dermatitis and EczemaDocument67 pagesDermatitis and EczemaIts AnythingNo ratings yet
- Rashes: Paediatric Dermatology: Ellis HonDocument95 pagesRashes: Paediatric Dermatology: Ellis HonB AuNo ratings yet
- DDX Chart Part 4Document7 pagesDDX Chart Part 4api-26938624No ratings yet
- 005 Jennings Clinical DermDocument21 pages005 Jennings Clinical Dermshadhana sivakumarNo ratings yet
- Skin DisordersDocument8 pagesSkin Disordersmarie leeNo ratings yet
- 1) Bacterial Skin InfDocument32 pages1) Bacterial Skin InfsmrutuNo ratings yet
- ST ND RD THDocument8 pagesST ND RD THLuvleen KaurNo ratings yet
- 5 Skin Hair and NailsDocument6 pages5 Skin Hair and NailsGliselleNo ratings yet
- Swollen Face: Group EDocument35 pagesSwollen Face: Group EaliaNo ratings yet
- Lecture 2 Sept 15thDocument10 pagesLecture 2 Sept 15thapi-26938624No ratings yet
- Impetigo, Erysipela S, Cellulitis: Rasay, Joana Mikee DDocument48 pagesImpetigo, Erysipela S, Cellulitis: Rasay, Joana Mikee DJoana Mikee RasayNo ratings yet
- Dermatitisslide 200715172028Document45 pagesDermatitisslide 200715172028enam professorNo ratings yet
- Dr. R. Sekhon - Dermatology Telehealth Jan 27 MRDocument45 pagesDr. R. Sekhon - Dermatology Telehealth Jan 27 MRAnissa ADNo ratings yet
- Eczematous EruptionsDocument27 pagesEczematous EruptionsSmartcool SoNo ratings yet
- Psoriasis and It's Homoeopathic ManagementDocument3 pagesPsoriasis and It's Homoeopathic ManagementInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Ulcer Genitalis EllenoDocument2 pagesUlcer Genitalis EllenoGabriela Sabatini GunawanNo ratings yet
- Primary Lesion: Carbuncles (Pustule) : Secondary Lesion: Dry Skin (Fissure)Document2 pagesPrimary Lesion: Carbuncles (Pustule) : Secondary Lesion: Dry Skin (Fissure)Catherine PradoNo ratings yet
- Hair Skin Nail AssessmentDocument6 pagesHair Skin Nail AssessmentJJNo ratings yet
- Dermatology Atlas for Medical StudentsFrom EverandDermatology Atlas for Medical StudentsRating: 4 out of 5 stars4/5 (6)
- Nms Ans Wb7 e Workbook Answers UE7Document3 pagesNms Ans Wb7 e Workbook Answers UE7nh kNo ratings yet
- Safety Standard For Horizontal Carousel Material Handling and Associated EquipmentDocument19 pagesSafety Standard For Horizontal Carousel Material Handling and Associated EquipmentIntegrated Systems DesignNo ratings yet
- Pregnancy TestDocument2 pagesPregnancy TestOsinachi WilsonNo ratings yet
- New Employees GuideDocument16 pagesNew Employees GuideDavid RobinsonNo ratings yet
- Brain Based Teaching and Learning2Document14 pagesBrain Based Teaching and Learning2Gerard-Ivan Apacible NotocseNo ratings yet
- Eating Well Recipe BookDocument92 pagesEating Well Recipe Bookwhite.serafimNo ratings yet
- Human Values & Professional EthicsDocument158 pagesHuman Values & Professional EthicsRaj Kumar67% (9)
- Core dSAT Vocabulary - Set 3Document2 pagesCore dSAT Vocabulary - Set 3Hưng NguyễnNo ratings yet
- 0500 s04 QP 2Document8 pages0500 s04 QP 2bluehorse99No ratings yet
- PP Ch2 3rdedDocument60 pagesPP Ch2 3rdedaying mugiwaraNo ratings yet
- Ingles III - Advantages and Disadvantages of Rapid Development in The Province of TeteDocument6 pagesIngles III - Advantages and Disadvantages of Rapid Development in The Province of TeteVercinio Teodoro VtbNo ratings yet
- WP Pharma PureSteam CIP en 58087042 Mar15Document8 pagesWP Pharma PureSteam CIP en 58087042 Mar15itung23No ratings yet
- RRLDocument6 pagesRRLTintin GatdulaNo ratings yet
- Abstract Book IccDocument97 pagesAbstract Book IccHasnain GoharNo ratings yet
- Restaurant - McdonaldsDocument9 pagesRestaurant - McdonaldsGABRIELA ELVIRA OSORIO MENDOZANo ratings yet
- This Study Resource Was: Piramal - E - Swasthya Case SubmissionDocument4 pagesThis Study Resource Was: Piramal - E - Swasthya Case SubmissiondjNo ratings yet
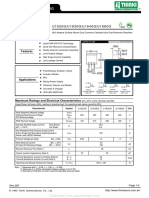
- U1620G Thru U1660G: U1620G/U1630G/U1640G/U1660GDocument2 pagesU1620G Thru U1660G: U1620G/U1630G/U1640G/U1660GTeles SilvaNo ratings yet
- Minetruck MT65: Underground Truck With 65-Tonne Load CapacityDocument5 pagesMinetruck MT65: Underground Truck With 65-Tonne Load CapacityAlvaro Patricio Garcia AlfaroNo ratings yet
- Topic 4 Duw1012 - EprDocument42 pagesTopic 4 Duw1012 - EprNazrina Rina100% (1)
- Chemical Kinetics: Chemistry: The Molecular Nature of Matter, 6EDocument128 pagesChemical Kinetics: Chemistry: The Molecular Nature of Matter, 6Eamel andiniNo ratings yet
- Plasma TV: Service ManualDocument34 pagesPlasma TV: Service ManualClaudelino ToffolettiNo ratings yet
- Title: Corrosion of Steel Reinforcement in Concrete and The Methods of Protection and MitigationDocument23 pagesTitle: Corrosion of Steel Reinforcement in Concrete and The Methods of Protection and MitigationMohammad AL HaririNo ratings yet
- Specification Chart of Pipes - Stainless Steel - Seamless Pipe - Mild Steel - Hollow SteelDocument5 pagesSpecification Chart of Pipes - Stainless Steel - Seamless Pipe - Mild Steel - Hollow SteelSarita BoteNo ratings yet
- Receivables P2Document4 pagesReceivables P2venice cambryNo ratings yet
- Project Standard Specification: Packaged Cooling Towers 15640 - Page 1/9Document9 pagesProject Standard Specification: Packaged Cooling Towers 15640 - Page 1/9adel rihanaNo ratings yet
- s555qw5w60101011010 Scalloppsnskskdndndn D Scalllpssond Sjsjsns S 3u373636191ir827472y152ta D D. DJDNDJFNFNF Ala. K K J N K nk755555511112727273737 11515152t2cawuwuwu272727 1116263636bllop - 1Document4 pagess555qw5w60101011010 Scalloppsnskskdndndn D Scalllpssond Sjsjsns S 3u373636191ir827472y152ta D D. DJDNDJFNFNF Ala. K K J N K nk755555511112727273737 11515152t2cawuwuwu272727 1116263636bllop - 1Red DiggerNo ratings yet
- Fpsyt 14 1244451Document8 pagesFpsyt 14 1244451Gilvan RangelNo ratings yet
























































































Download as pdf or txt
You might also like
- Wound Types Poster For ReviewDocument1 pageWound Types Poster For Reviewapi-702908151No ratings yet
- Case Summary Pediatrics32 5-Year-ODocument12 pagesCase Summary Pediatrics32 5-Year-OMaryam FadahNo ratings yet
- Khawater Makki Cover Letter.ADocument1 pageKhawater Makki Cover Letter.AAnonymous miK3qJxNo ratings yet
- VATS Bypass ModuleDocument3 pagesVATS Bypass ModuleSHOOTEENo ratings yet
- White Pony - DeftonesDocument7 pagesWhite Pony - DeftonesAarón Espinosa GarcíaNo ratings yet
- Bacterial Skin Infections: Basic Dermatology CurriculumDocument78 pagesBacterial Skin Infections: Basic Dermatology CurriculumAnthony Bravo CortezNo ratings yet
- Bacterial Skin Infections: Basic Dermatology CurriculumDocument75 pagesBacterial Skin Infections: Basic Dermatology CurriculummasithaNo ratings yet
- Integumentry PDFDocument17 pagesIntegumentry PDFMehul RathoreNo ratings yet
- Integumentry Dermatitis Bacterial Impetigo Cellulitis Abscess DefDocument17 pagesIntegumentry Dermatitis Bacterial Impetigo Cellulitis Abscess DefMehul RathoreNo ratings yet
- Skinlesionsteam 5Document33 pagesSkinlesionsteam 5Noemí TorresNo ratings yet
- 17 Epidermal New GrowthsDocument3 pages17 Epidermal New GrowthsWaiwit KritayakiranaNo ratings yet
- History and Epidemiology: Key FeaturesDocument8 pagesHistory and Epidemiology: Key FeaturesAswin KrishnaNo ratings yet
- AnnexIII DifferentialDiagnosis FromNLEP India PDFDocument3 pagesAnnexIII DifferentialDiagnosis FromNLEP India PDFAegirine RafilahNo ratings yet
- Eczema& Allergic Contact-DermatitisDocument70 pagesEczema& Allergic Contact-Dermatitisamraayman21No ratings yet
- ICD TableDocument1 pageICD TableJo CanensNo ratings yet
- Diagnosis and Management of Tinea Infections: Am Fam Physician. 2014 Nov 15 90 (10) :702-711Document20 pagesDiagnosis and Management of Tinea Infections: Am Fam Physician. 2014 Nov 15 90 (10) :702-711'rha' Ittuu IrraaNo ratings yet
- Skin Condition TableDocument3 pagesSkin Condition TableELI GOZONNo ratings yet
- Disorders of The Integumentary System: Internet ResourcesDocument4 pagesDisorders of The Integumentary System: Internet ResourcesDylan Dela CruzNo ratings yet
- Skin, Hair and Nails Ok - CompressedDocument67 pagesSkin, Hair and Nails Ok - CompressedFelya Elsa Pratiwi KurniaNo ratings yet
- Arterial, Venous, Lymph EdemaDocument2 pagesArterial, Venous, Lymph EdemapallenNo ratings yet
- Derm LOsDocument37 pagesDerm LOskatherine nunnNo ratings yet
- Skin Disorders 4-2-08Document14 pagesSkin Disorders 4-2-08api-3822433No ratings yet
- Handout2 - Major Clinical Features of Genital UlcersDocument1 pageHandout2 - Major Clinical Features of Genital Ulcersgdudex118811No ratings yet
- PsoriasisDocument27 pagesPsoriasisNikkaDablioNo ratings yet
- Dermatology ConditionsDocument8 pagesDermatology ConditionsmeilunlyNo ratings yet
- Shanz - PEDIA II 2.01 NEWDocument8 pagesShanz - PEDIA II 2.01 NEWPetrina XuNo ratings yet
- Derm ChartDocument109 pagesDerm ChartAlana BolloneNo ratings yet
- Wound ManagementDocument6 pagesWound ManagementBianca Corina MusatNo ratings yet
- Skin and Body Membranes For AnaPhyDocument3 pagesSkin and Body Membranes For AnaPhyJASHEL M. CASTANARESNo ratings yet
- Med1 Skin Hair and NailsDocument15 pagesMed1 Skin Hair and NailsCathleen KirstenNo ratings yet
- Slide 11-17 by Ur BabyDocument6 pagesSlide 11-17 by Ur Babyfeloniacarl34No ratings yet
- Bacterial Skin InfectionsDocument9 pagesBacterial Skin InfectionskateverdadNo ratings yet
- JwillzDocument14 pagesJwillzWyatt WarawaNo ratings yet
- Skin Examination 1Document9 pagesSkin Examination 1Marry JuttNo ratings yet
- Male Genital DermDocument112 pagesMale Genital DermVũ CaoNo ratings yet
- Diabetic Foot Hajera FinalDocument38 pagesDiabetic Foot Hajera FinalAfifah SelamatNo ratings yet
- UlcerDocument3 pagesUlcerMd Ahsanuzzaman PinkuNo ratings yet
- Herpes Zoster: Iqbal Ainn Un A. Tutor 23Document21 pagesHerpes Zoster: Iqbal Ainn Un A. Tutor 23inunNo ratings yet
- Type of The Wound-JCF 4thDocument25 pagesType of The Wound-JCF 4thTaufik HidayantoNo ratings yet
- Triage: A - Raf B - Kath C - Cara D - Cesca E - Kyla F - Michelle G - AndreDocument4 pagesTriage: A - Raf B - Kath C - Cara D - Cesca E - Kyla F - Michelle G - AndreLeira BarbosaNo ratings yet
- PsoriasisDocument23 pagesPsoriasisvasavavipul38022No ratings yet
- Internal Medicine Finals ReviewerDocument8 pagesInternal Medicine Finals ReviewerRojales FrancisNo ratings yet
- Psoriasis Management in The Community: BY DR U.B.Buhari Gpwer FRCGP MHADocument50 pagesPsoriasis Management in The Community: BY DR U.B.Buhari Gpwer FRCGP MHAEng Abdikariim AbdillahiNo ratings yet
- Cause and PathogenesisDocument11 pagesCause and Pathogenesiswanaibor RyngksaiNo ratings yet
- Dermatitis and EczemaDocument67 pagesDermatitis and EczemaIts AnythingNo ratings yet
- Rashes: Paediatric Dermatology: Ellis HonDocument95 pagesRashes: Paediatric Dermatology: Ellis HonB AuNo ratings yet
- DDX Chart Part 4Document7 pagesDDX Chart Part 4api-26938624No ratings yet
- 005 Jennings Clinical DermDocument21 pages005 Jennings Clinical Dermshadhana sivakumarNo ratings yet
- Skin DisordersDocument8 pagesSkin Disordersmarie leeNo ratings yet
- 1) Bacterial Skin InfDocument32 pages1) Bacterial Skin InfsmrutuNo ratings yet
- ST ND RD THDocument8 pagesST ND RD THLuvleen KaurNo ratings yet
- 5 Skin Hair and NailsDocument6 pages5 Skin Hair and NailsGliselleNo ratings yet
- Swollen Face: Group EDocument35 pagesSwollen Face: Group EaliaNo ratings yet
- Lecture 2 Sept 15thDocument10 pagesLecture 2 Sept 15thapi-26938624No ratings yet
- Impetigo, Erysipela S, Cellulitis: Rasay, Joana Mikee DDocument48 pagesImpetigo, Erysipela S, Cellulitis: Rasay, Joana Mikee DJoana Mikee RasayNo ratings yet
- Dermatitisslide 200715172028Document45 pagesDermatitisslide 200715172028enam professorNo ratings yet
- Dr. R. Sekhon - Dermatology Telehealth Jan 27 MRDocument45 pagesDr. R. Sekhon - Dermatology Telehealth Jan 27 MRAnissa ADNo ratings yet
- Eczematous EruptionsDocument27 pagesEczematous EruptionsSmartcool SoNo ratings yet
- Psoriasis and It's Homoeopathic ManagementDocument3 pagesPsoriasis and It's Homoeopathic ManagementInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Ulcer Genitalis EllenoDocument2 pagesUlcer Genitalis EllenoGabriela Sabatini GunawanNo ratings yet
- Primary Lesion: Carbuncles (Pustule) : Secondary Lesion: Dry Skin (Fissure)Document2 pagesPrimary Lesion: Carbuncles (Pustule) : Secondary Lesion: Dry Skin (Fissure)Catherine PradoNo ratings yet
- Hair Skin Nail AssessmentDocument6 pagesHair Skin Nail AssessmentJJNo ratings yet
- Dermatology Atlas for Medical StudentsFrom EverandDermatology Atlas for Medical StudentsRating: 4 out of 5 stars4/5 (6)
- Nms Ans Wb7 e Workbook Answers UE7Document3 pagesNms Ans Wb7 e Workbook Answers UE7nh kNo ratings yet
- Safety Standard For Horizontal Carousel Material Handling and Associated EquipmentDocument19 pagesSafety Standard For Horizontal Carousel Material Handling and Associated EquipmentIntegrated Systems DesignNo ratings yet
- Pregnancy TestDocument2 pagesPregnancy TestOsinachi WilsonNo ratings yet
- New Employees GuideDocument16 pagesNew Employees GuideDavid RobinsonNo ratings yet
- Brain Based Teaching and Learning2Document14 pagesBrain Based Teaching and Learning2Gerard-Ivan Apacible NotocseNo ratings yet
- Eating Well Recipe BookDocument92 pagesEating Well Recipe Bookwhite.serafimNo ratings yet
- Human Values & Professional EthicsDocument158 pagesHuman Values & Professional EthicsRaj Kumar67% (9)
- Core dSAT Vocabulary - Set 3Document2 pagesCore dSAT Vocabulary - Set 3Hưng NguyễnNo ratings yet
- 0500 s04 QP 2Document8 pages0500 s04 QP 2bluehorse99No ratings yet
- PP Ch2 3rdedDocument60 pagesPP Ch2 3rdedaying mugiwaraNo ratings yet
- Ingles III - Advantages and Disadvantages of Rapid Development in The Province of TeteDocument6 pagesIngles III - Advantages and Disadvantages of Rapid Development in The Province of TeteVercinio Teodoro VtbNo ratings yet
- WP Pharma PureSteam CIP en 58087042 Mar15Document8 pagesWP Pharma PureSteam CIP en 58087042 Mar15itung23No ratings yet
- RRLDocument6 pagesRRLTintin GatdulaNo ratings yet
- Abstract Book IccDocument97 pagesAbstract Book IccHasnain GoharNo ratings yet
- Restaurant - McdonaldsDocument9 pagesRestaurant - McdonaldsGABRIELA ELVIRA OSORIO MENDOZANo ratings yet
- This Study Resource Was: Piramal - E - Swasthya Case SubmissionDocument4 pagesThis Study Resource Was: Piramal - E - Swasthya Case SubmissiondjNo ratings yet
- U1620G Thru U1660G: U1620G/U1630G/U1640G/U1660GDocument2 pagesU1620G Thru U1660G: U1620G/U1630G/U1640G/U1660GTeles SilvaNo ratings yet
- Minetruck MT65: Underground Truck With 65-Tonne Load CapacityDocument5 pagesMinetruck MT65: Underground Truck With 65-Tonne Load CapacityAlvaro Patricio Garcia AlfaroNo ratings yet
- Topic 4 Duw1012 - EprDocument42 pagesTopic 4 Duw1012 - EprNazrina Rina100% (1)
- Chemical Kinetics: Chemistry: The Molecular Nature of Matter, 6EDocument128 pagesChemical Kinetics: Chemistry: The Molecular Nature of Matter, 6Eamel andiniNo ratings yet
- Plasma TV: Service ManualDocument34 pagesPlasma TV: Service ManualClaudelino ToffolettiNo ratings yet
- Title: Corrosion of Steel Reinforcement in Concrete and The Methods of Protection and MitigationDocument23 pagesTitle: Corrosion of Steel Reinforcement in Concrete and The Methods of Protection and MitigationMohammad AL HaririNo ratings yet
- Specification Chart of Pipes - Stainless Steel - Seamless Pipe - Mild Steel - Hollow SteelDocument5 pagesSpecification Chart of Pipes - Stainless Steel - Seamless Pipe - Mild Steel - Hollow SteelSarita BoteNo ratings yet
- Receivables P2Document4 pagesReceivables P2venice cambryNo ratings yet
- Project Standard Specification: Packaged Cooling Towers 15640 - Page 1/9Document9 pagesProject Standard Specification: Packaged Cooling Towers 15640 - Page 1/9adel rihanaNo ratings yet
- s555qw5w60101011010 Scalloppsnskskdndndn D Scalllpssond Sjsjsns S 3u373636191ir827472y152ta D D. DJDNDJFNFNF Ala. K K J N K nk755555511112727273737 11515152t2cawuwuwu272727 1116263636bllop - 1Document4 pagess555qw5w60101011010 Scalloppsnskskdndndn D Scalllpssond Sjsjsns S 3u373636191ir827472y152ta D D. DJDNDJFNFNF Ala. K K J N K nk755555511112727273737 11515152t2cawuwuwu272727 1116263636bllop - 1Red DiggerNo ratings yet
- Fpsyt 14 1244451Document8 pagesFpsyt 14 1244451Gilvan RangelNo ratings yet