Download as pdf or txt
You might also like
- FPE30806 Exam Excel File 2020Document18 pagesFPE30806 Exam Excel File 2020Antonio MoncayoNo ratings yet
- History of OrthodonticsDocument70 pagesHistory of Orthodonticsdr_nilofervevai236080% (5)
- Unit 1 TEO History of DentistryDocument4 pagesUnit 1 TEO History of DentistryMaria Jose CamposNo ratings yet
- Denturebaseresin 121213120311 Phpapp02Document129 pagesDenturebaseresin 121213120311 Phpapp02pooja nagojiNo ratings yet
- DENTURE BASE MATERIALfDocument128 pagesDENTURE BASE MATERIALfnandhini2k23No ratings yet
- Denture Base Resins Part1Document52 pagesDenture Base Resins Part1Aryudhi ArmisNo ratings yet
- Prosthodontics: Friday, February 19, 2021 11:53 AMDocument2 pagesProsthodontics: Friday, February 19, 2021 11:53 AMjunquelalaNo ratings yet
- Denture Base Materials From Past To Futu PDFDocument7 pagesDenture Base Materials From Past To Futu PDFmarwaNo ratings yet
- Denture Base ResinsDocument44 pagesDenture Base Resinshersimran waliaNo ratings yet
- Denture Base ResinsDocument22 pagesDenture Base ResinsAkshayaa BalajiNo ratings yet
- 5 Denture Base Materials and Processsing TechsDocument78 pages5 Denture Base Materials and Processsing TechsDRNIRBANMITRANo ratings yet
- Denture Teeth: Prof. Dr. Radnai Márta Univ. Szeged, Dental Faculty, Department of ProsthodonticsDocument8 pagesDenture Teeth: Prof. Dr. Radnai Márta Univ. Szeged, Dental Faculty, Department of ProsthodonticsShahriar honarmandNo ratings yet
- Denture Teeth: Prof. Dr. Radnai Márta Univ. Szeged, Dental Faculty, Department of ProsthodonticsDocument8 pagesDenture Teeth: Prof. Dr. Radnai Márta Univ. Szeged, Dental Faculty, Department of ProsthodonticsShahriar honarmandNo ratings yet
- Lec 1 Introduction To Dental MaterialsDocument24 pagesLec 1 Introduction To Dental MaterialsMaryam JawaidNo ratings yet
- Dental Ceramics - Seminar / Orthodontic Courses by Indian Dental AcademyDocument63 pagesDental Ceramics - Seminar / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- Enamelautosaved 180529103526Document195 pagesEnamelautosaved 180529103526AyeshaNo ratings yet
- Metal Free Ceramics / Orthodontic Courses by Indian Dental AcademyDocument166 pagesMetal Free Ceramics / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- Flexible Dentures: A Boon in Compromised Conditions: ReviewDocument4 pagesFlexible Dentures: A Boon in Compromised Conditions: ReviewAnisa DyahNo ratings yet
- Evolution of Denture Base Materials: Review ArticleDocument6 pagesEvolution of Denture Base Materials: Review ArticleshraddhaNo ratings yet
- History of ProsthodonticsDocument121 pagesHistory of ProsthodonticsArthi Ramalingam aNo ratings yet
- History: Full and Partial Coverage CrownsDocument7 pagesHistory: Full and Partial Coverage CrownsAki AvlonNo ratings yet
- The History of DentistryDocument11 pagesThe History of DentistryDima Cuzub100% (1)
- Oet 1Document7 pagesOet 1Yağız BakanayNo ratings yet
- Toothpaste Lab: Environmental Explorations Mr. Luis A. VelazquezDocument13 pagesToothpaste Lab: Environmental Explorations Mr. Luis A. VelazquezTanvi PatilNo ratings yet
- MFP MaterialsDocument64 pagesMFP MaterialsആനNo ratings yet
- Restoration of Endodontically Treated TeethDocument194 pagesRestoration of Endodontically Treated TeethBharti DuaNo ratings yet
- DENTAL MATERIALS - Lec MidtermsDocument13 pagesDENTAL MATERIALS - Lec MidtermsArjelyn LungcayNo ratings yet
- Maxillofacial Materials: Review ArticleDocument4 pagesMaxillofacial Materials: Review ArticleAli Faraz SiddiquiNo ratings yet
- Metal Free Ceramics in DentistryDocument5 pagesMetal Free Ceramics in DentistryAkanksha MahajanNo ratings yet
- Jurnal Implant Gigi 4 PDFDocument6 pagesJurnal Implant Gigi 4 PDFFaiqotul KumalaNo ratings yet
- Bahasa InggrisDocument13 pagesBahasa InggrisCantikaNo ratings yet
- Latihan TkbiDocument4 pagesLatihan Tkbiyd pNo ratings yet
- DBRDocument262 pagesDBRDr.Ragini PandeyNo ratings yet
- Sesión 10 - SincrónicaDocument34 pagesSesión 10 - SincrónicaGRISSEL ROSARIO PARDAVE CABELLONo ratings yet
- Introduction To Ceramics1Document98 pagesIntroduction To Ceramics1smritinarayanNo ratings yet
- Complete Denture ImpressionsDocument208 pagesComplete Denture ImpressionsRohan Grover100% (1)
- 2.dental CeramicsDocument320 pages2.dental CeramicsNamitha AP100% (1)
- Glassionomercement 160205135333Document167 pagesGlassionomercement 160205135333Hemant ChourhaNo ratings yet
- E Bne Sajjad 2011Document47 pagesE Bne Sajjad 2011Princekumar MishraNo ratings yet
- Casey 1981Document10 pagesCasey 1981ArdeamusfarNo ratings yet
- History of EndodonticsDocument47 pagesHistory of EndodonticsMohhamad Reza JouyandehNo ratings yet
- An Assesment On How Will The Oyster Shell Contribute in Crafting A Tile in Modern DayDocument11 pagesAn Assesment On How Will The Oyster Shell Contribute in Crafting A Tile in Modern DayKent Bryan Navarro VillamarNo ratings yet
- Ceramics DypDocument168 pagesCeramics DypRukhsar VankaniNo ratings yet
- Complete Denture ImpressionsDocument222 pagesComplete Denture ImpressionsAmar BimavarapuNo ratings yet
- Polymers: Dr. Shilan Hameed Fatah M.SC in ProsthodonticsDocument26 pagesPolymers: Dr. Shilan Hameed Fatah M.SC in Prosthodonticsمحمد مظفر سعيد حسينNo ratings yet
- Bahasa Inggris 2Document14 pagesBahasa Inggris 2CantikaNo ratings yet
- History of DentistryDocument49 pagesHistory of DentistryJoury ABNo ratings yet
- Porcelain Esthetics For The 21st CenturyDocument5 pagesPorcelain Esthetics For The 21st CenturyCah YaniNo ratings yet
- Review On History of Complete Denture. Mohamad Qulam Zaki, DR Preetham Prasad NitlaDocument4 pagesReview On History of Complete Denture. Mohamad Qulam Zaki, DR Preetham Prasad NitlaMohamad Qulam ZakiNo ratings yet
- Future of Dental Biomaterials Gazing Into Bob S Crystal BallDocument7 pagesFuture of Dental Biomaterials Gazing Into Bob S Crystal BallliguojieNo ratings yet
- Historical Interest of Denture Base Materials: Dr.M.Vasantha Kumar, DR - Swati Bhagath, Dr.J.Brintha JeiDocument3 pagesHistorical Interest of Denture Base Materials: Dr.M.Vasantha Kumar, DR - Swati Bhagath, Dr.J.Brintha Jeiஹரி ராமச்சந்திரன்No ratings yet
- History of Maxillofacial ProsthesisDocument34 pagesHistory of Maxillofacial ProsthesisMoataz Mohamed Barakat100% (1)
- Began in The 17th CenturyDocument82 pagesBegan in The 17th CenturyCharlene LunaNo ratings yet
- Impression Making-Theories and Techniques: DR - Priyanka Makkar P.G. 2 Year Dept of ProsthodonticsDocument114 pagesImpression Making-Theories and Techniques: DR - Priyanka Makkar P.G. 2 Year Dept of ProsthodonticsZachary DuongNo ratings yet
- Dental Material IntroductionDocument3 pagesDental Material Introductionbrizacia vaniaNo ratings yet
- Ashok Sir Arch WireDocument130 pagesAshok Sir Arch WireDeepuUrs100% (1)
- Dental ImplantDocument7 pagesDental ImplantMohammed HassanNo ratings yet
- Dental Caries: Sohail PGT: 1 Yr Dept of Pedodontics SVS Institute of Dental SciencesDocument255 pagesDental Caries: Sohail PGT: 1 Yr Dept of Pedodontics SVS Institute of Dental SciencesRaj Kumar GundlaNo ratings yet
- Quick Quirk Quiz: Science & TechnologyFrom EverandQuick Quirk Quiz: Science & TechnologyRating: 2 out of 5 stars2/5 (1)
- Molecular Structure of Solid Liquid and GasDocument2 pagesMolecular Structure of Solid Liquid and GasKoser IrshadNo ratings yet
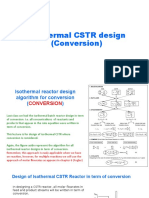
- Lecture 8 Isothermal CSTR Design (Conversion)Document11 pagesLecture 8 Isothermal CSTR Design (Conversion)Mhmad E. HerzallahNo ratings yet
- NptelDocument2 pagesNptelscorpionarnoldNo ratings yet
- Supreme A006 Super Shield SBSDocument2 pagesSupreme A006 Super Shield SBSatrijoshiNo ratings yet
- Polyethylene (PE) Plastic Pipe (SIDR-PR) Based On Controlled Inside DiameterDocument7 pagesPolyethylene (PE) Plastic Pipe (SIDR-PR) Based On Controlled Inside DiameterDavid SolisNo ratings yet
- PV 1303Document10 pagesPV 1303tufantasma100% (2)
- 2 Caterpillar Drive ChainDocument1 page2 Caterpillar Drive ChainFernando Mendoza0% (1)
- Report On Gas TurbineDocument33 pagesReport On Gas TurbineKanika Kumar100% (1)
- 3M FC 600F Light WaterDocument7 pages3M FC 600F Light WaterJose Luis RodriguezNo ratings yet
- Stud Calculations C16 B3 LevelDocument1 pageStud Calculations C16 B3 LevelRonakShahNo ratings yet
- Principles, Operational Challenges, and Perspectives in Boiler Feedwater Treatment ProcessDocument11 pagesPrinciples, Operational Challenges, and Perspectives in Boiler Feedwater Treatment ProcessNguyễn Quốc ViệtNo ratings yet
- Item Analysis-Section HDocument8 pagesItem Analysis-Section HLiezelNo ratings yet
- Fluid Bed ProcessorDocument16 pagesFluid Bed ProcessorjavierbravoantonNo ratings yet
- Transport in Plants: Pre-Medical: Biology AllenDocument16 pagesTransport in Plants: Pre-Medical: Biology AllenJK JHANo ratings yet
- TP GB Re Laf 030Document17 pagesTP GB Re Laf 030mljaininsulationNo ratings yet
- C Ce 0432 CPD 221051 enDocument54 pagesC Ce 0432 CPD 221051 enKhuyến Nguyễn VănNo ratings yet
- Class 12 Chemistry One LinerDocument4 pagesClass 12 Chemistry One Lineranoopkumar8127798122No ratings yet
- NCM 106 PHARMACOLOGY - PrelimsDocument26 pagesNCM 106 PHARMACOLOGY - PrelimsKelsey Macaraig100% (3)
- Chapter 10 The Factorial Method of Cost EstimationDocument8 pagesChapter 10 The Factorial Method of Cost Estimationภูมิรพี ศรีโวทานัยNo ratings yet
- 4000 MTPD Ammonia Plant Based On Proven Technology: Joachim Rüther, John Larsen, Dennis Lippmann, Detlev ClaesDocument8 pages4000 MTPD Ammonia Plant Based On Proven Technology: Joachim Rüther, John Larsen, Dennis Lippmann, Detlev Claesvaratharajan g rNo ratings yet
- Pulp Mill and Chemical Recovery Control With Advanced Analyzers - From Trees To Final ProductDocument9 pagesPulp Mill and Chemical Recovery Control With Advanced Analyzers - From Trees To Final ProductLarisse BatalhaNo ratings yet
- Tall Form Spray Dryer by RichiezDocument34 pagesTall Form Spray Dryer by RichiezRichard Obinna100% (1)
- Calculation of Brine PropertiesDocument26 pagesCalculation of Brine PropertiesacfernandezNo ratings yet
- Wetico Water Tank 70m Shell Ultimate ChecksDocument2 pagesWetico Water Tank 70m Shell Ultimate ChecksChristian Paul SanguyoNo ratings yet
- 3,5-Dinitrobenzoic AcidDocument3 pages3,5-Dinitrobenzoic Acidpulkit asatiNo ratings yet
- 1-3 Cold Welding, EtcDocument50 pages1-3 Cold Welding, EtcNguyễn Hồng Thanh100% (2)
- MaterialDocument4 pagesMaterialAmit PandeyNo ratings yet
- Sika PDS E PVC WaterstopDocument3 pagesSika PDS E PVC Waterstoplwin_oo2435No ratings yet
- Compress Report For Pressure VesselDocument394 pagesCompress Report For Pressure VesselgaurangNo ratings yet