
Submitted By: BSN 3Y2-9B: Nursing Care Plan (O.B.)
Submitted By: BSN 3Y2-9B: Nursing Care Plan (O.B.)
You might also like
- Nursing Care Plan - ConstipationDocument2 pagesNursing Care Plan - Constipationderic86% (72)
- Pre Reg Pharmacists Last MinuteDocument9 pagesPre Reg Pharmacists Last MinuteBob BobNo ratings yet
- Nursing Care Plan ConstipationDocument2 pagesNursing Care Plan ConstipationkazelleNo ratings yet
- Nursing Care Plan: Short Term: Difficulty in Swallowing Nursing Diagnosis Planning Implementation Rationale EvaluationDocument6 pagesNursing Care Plan: Short Term: Difficulty in Swallowing Nursing Diagnosis Planning Implementation Rationale EvaluationNico Angelo Hibaya TugononNo ratings yet
- Nursing Care Plan Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective: Short Term Goal: IndependentDocument2 pagesNursing Care Plan Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective: Short Term Goal: IndependentEva Marielle CezaldoNo ratings yet
- Bowel Incontinence ConstipationDocument3 pagesBowel Incontinence ConstipationMatty-b AskalaniNo ratings yet
- Diarrhea Nursing Care PlanDocument2 pagesDiarrhea Nursing Care PlanKrizha Angela NicolasNo ratings yet
- Nursing Problem Explanation Goal Intervention Rationale Evaluation SubjectiveDocument1 pageNursing Problem Explanation Goal Intervention Rationale Evaluation SubjectiveZed P. EstalillaNo ratings yet
- DiarrheaDocument3 pagesDiarrheaBert GasalNo ratings yet
- ConstipationDocument4 pagesConstipationprincess_bee100% (1)
- Constipation LeukemiaDocument1 pageConstipation LeukemiamawelNo ratings yet
- Constipation NCPDocument3 pagesConstipation NCPIRISH CACAYANNo ratings yet
- NCP ConstipationDocument2 pagesNCP ConstipationFaith Bingan Remiscal67% (6)
- Constipation NCPDocument2 pagesConstipation NCPAbby GonzalesNo ratings yet
- Assessment Diagnosis Planning Implementation Rationale Evaluation Subjective Data: Objective Data: Short Term: Independent: Short Term: Goal Partially MetDocument3 pagesAssessment Diagnosis Planning Implementation Rationale Evaluation Subjective Data: Objective Data: Short Term: Independent: Short Term: Goal Partially MetCess YNo ratings yet
- "Nagtatae Siya 4 Days Na" As Verbalized by The Mother. Inatake of Causative Agents Irritation of The Stomach Inflammation of The Stomach Increase GI Motility DiarrrheaDocument4 pages"Nagtatae Siya 4 Days Na" As Verbalized by The Mother. Inatake of Causative Agents Irritation of The Stomach Inflammation of The Stomach Increase GI Motility DiarrrheaMelissa MhelNo ratings yet
- A Nursing Care Plan On: Loose Bowel MovementDocument6 pagesA Nursing Care Plan On: Loose Bowel MovementakoitsmeNo ratings yet
- Name: de Guzman, Cameron Josh B. Section: 2Bsn-ADocument3 pagesName: de Guzman, Cameron Josh B. Section: 2Bsn-ACameron De GuzmanNo ratings yet
- Assessment Healt H Patte RN Nursing Diagnosis Desired Outcome (Edit) Intervention (Edit) Evaluation (EDIT) Rema RKSDocument3 pagesAssessment Healt H Patte RN Nursing Diagnosis Desired Outcome (Edit) Intervention (Edit) Evaluation (EDIT) Rema RKStflorenzNo ratings yet
- College of Nursing: Assessment Diagnosis Analysis Planning Implementation Rationale EvaluationDocument2 pagesCollege of Nursing: Assessment Diagnosis Analysis Planning Implementation Rationale EvaluationDiana Anne MarisNo ratings yet
- College of Nursing: Assessment Diagnosis Analysis Planning Implementation Rationale EvaluationDocument2 pagesCollege of Nursing: Assessment Diagnosis Analysis Planning Implementation Rationale EvaluationjoanneNo ratings yet
- NCP 1Document2 pagesNCP 1Cedmarc Francis RenionNo ratings yet
- Maraming Tubig at Kakain NG Prutas para Makadumi Ako."Document2 pagesMaraming Tubig at Kakain NG Prutas para Makadumi Ako."Cayla Mae CarlosNo ratings yet
- PeristalticDocument2 pagesPeristalticAllyzah Faith BernalesNo ratings yet
- Nursing Care Plan 1BSN 14 Group 1Document8 pagesNursing Care Plan 1BSN 14 Group 1Mikaella GacostaNo ratings yet
- ConstipationDocument2 pagesConstipationjinsi georgeNo ratings yet
- NCP Ruth DeveraDocument8 pagesNCP Ruth DeveraBESA JERIC FLORESNo ratings yet
- Risk For Constipation Nursing Care Plan Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective Data: Independent: Goal MetDocument10 pagesRisk For Constipation Nursing Care Plan Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective Data: Independent: Goal MetHydie Mae AlcabedosNo ratings yet
- Nursing Care Plan ConstipationDocument2 pagesNursing Care Plan ConstipationGio Baduria100% (1)
- ConstipationDocument3 pagesConstipationmyer pasandalanNo ratings yet
- Any Up-Dates Are To Be Completed in Different Color Ink. The Student Is Expected To Document All Meds The Client Is Currently ReceivingDocument1 pageAny Up-Dates Are To Be Completed in Different Color Ink. The Student Is Expected To Document All Meds The Client Is Currently Receivinggeorgeloto12No ratings yet
- CARE PLAN Format - ConstipationDocument2 pagesCARE PLAN Format - Constipationjinsi georgeNo ratings yet
- University of The East Ramon Magsaysay Memorial Medical Center, Inc. College of NursingDocument23 pagesUniversity of The East Ramon Magsaysay Memorial Medical Center, Inc. College of NursingReina RamonesNo ratings yet
- NCP Risk For ConstipationDocument1 pageNCP Risk For Constipationjorgeacct50% (4)
- NCP3Document4 pagesNCP3Noreen GyleNo ratings yet
- Nursing Care Plan Assessment Diagnosis Outcome Intervention Rationale EvaluationDocument3 pagesNursing Care Plan Assessment Diagnosis Outcome Intervention Rationale EvaluationMarivic Yuson MalagarNo ratings yet
- CHOLELITHIASISDocument4 pagesCHOLELITHIASISKate ValdesNo ratings yet
- Discharge Planning and NCP SDocument8 pagesDischarge Planning and NCP SRainier RamosNo ratings yet
- COLON CANCER NCP-impaired nutrITIONDocument3 pagesCOLON CANCER NCP-impaired nutrITIONNicole cuencosNo ratings yet
- NCP WilliamDocument2 pagesNCP WilliamApril Louise PaluganNo ratings yet
- DIARRHEADocument2 pagesDIARRHEADanielNo ratings yet
- Assessment Diagnosis Inference Planning Intervention Rationale EvaluationDocument1 pageAssessment Diagnosis Inference Planning Intervention Rationale EvaluationLoverMind CabaronNo ratings yet
- NCP DiverticulitisDocument6 pagesNCP DiverticulitisLovely Cacapit100% (1)
- Viii. Nursing Care Plan: Asessment Diagnosis Planning Intervention Rationale EvaluationDocument3 pagesViii. Nursing Care Plan: Asessment Diagnosis Planning Intervention Rationale Evaluationhehehe29No ratings yet
- Assessment Diagnosis Planning Implementation Rationale Evaluation Subjective Data: Short Term: Independent: Short Term: Goal Partially MetDocument3 pagesAssessment Diagnosis Planning Implementation Rationale Evaluation Subjective Data: Short Term: Independent: Short Term: Goal Partially MetPrincess Mildred AbdonNo ratings yet
- Constipation NCPDocument3 pagesConstipation NCPSeth Amiel MotaNo ratings yet
- Name: Babu Kaji Maharjan: Patient's IdentificationDocument6 pagesName: Babu Kaji Maharjan: Patient's IdentificationAlisha MaharjanNo ratings yet
- NCP JaundiceDocument9 pagesNCP JaundiceMeena Koushal100% (1)
- CHA NCPDocument6 pagesCHA NCPMonty_Legaspi_5664No ratings yet
- Digestive System Nursing Diagnoses & Care PlansDocument7 pagesDigestive System Nursing Diagnoses & Care PlansyormahdNo ratings yet
- New Intestinal ObstructionDocument12 pagesNew Intestinal Obstructionmustafalotfy01No ratings yet
- NCP (Diarrhea)Document2 pagesNCP (Diarrhea)Rodj Bilang Jr.83% (30)
- Nursing Care Plan: Assessment Nursing Diagnosis Rationale Desired Outcome Nursing Intervention Justification EvaluationDocument2 pagesNursing Care Plan: Assessment Nursing Diagnosis Rationale Desired Outcome Nursing Intervention Justification EvaluationDan MandigNo ratings yet
- Food Is Figureoutable: AN ESSENTIAL GUIDE TO BODY SYSTEMSFrom EverandFood Is Figureoutable: AN ESSENTIAL GUIDE TO BODY SYSTEMSNo ratings yet
- Intestinal Failure: Diagnosis, Management and TransplantationFrom EverandIntestinal Failure: Diagnosis, Management and TransplantationAlan LangnasNo ratings yet
- Intermittent Fasting: The Most Effective Diet, the Healthiest LifestyleFrom EverandIntermittent Fasting: The Most Effective Diet, the Healthiest LifestyleNo ratings yet
- Natural Cures for Constipation: Curing Constipation PermanentlyFrom EverandNatural Cures for Constipation: Curing Constipation PermanentlyNo ratings yet
- Health Education PlanDocument3 pagesHealth Education PlanCamille VegaNo ratings yet
- Minutes of 290th Meeting of Registration BoardDocument1,286 pagesMinutes of 290th Meeting of Registration BoardUsman DarNo ratings yet
- Jurnal Tonsil Limfoma Non HodgkinDocument5 pagesJurnal Tonsil Limfoma Non HodgkinAhmad RamadhanuNo ratings yet
- Recommendations For Infection Control For The Practice of AnesthesiologyDocument86 pagesRecommendations For Infection Control For The Practice of AnesthesiologyAhmed MostafaNo ratings yet
- CandidiasisDocument27 pagesCandidiasisBhavesh SippyNo ratings yet
- Client Consultation Form - Pedicure AppoinmentDocument3 pagesClient Consultation Form - Pedicure AppoinmentMicheal McDowellNo ratings yet
- 1 Hospital Organisation & FunctionDocument16 pages1 Hospital Organisation & FunctionAtrao67% (3)
- Makalah Komplementer Pada Masa NifasDocument7 pagesMakalah Komplementer Pada Masa NifasWirda TariNo ratings yet
- A Review of Classification of Disease in AyurvedaDocument11 pagesA Review of Classification of Disease in AyurvedaEditor_IAIMNo ratings yet
- FLCCC Alliance Frequently Asked Questions On IvermectinDocument12 pagesFLCCC Alliance Frequently Asked Questions On IvermectinAndrés Mario Rivera RojasNo ratings yet
- CC C C: 1. Rapid Changes in Health Care Technology and Therapiesc " C CDocument18 pagesCC C C: 1. Rapid Changes in Health Care Technology and Therapiesc " C CEric Blahhal100% (6)
- Jurnal Transfusi Darah 2Document11 pagesJurnal Transfusi Darah 2widiamNo ratings yet
- Failure To Thrive JournalDocument13 pagesFailure To Thrive JournalApRil Anne BalanonNo ratings yet
- Oral Hygiene Dengan Kenyamanan Pasien Di Intensive Care Unit (Icu)Document13 pagesOral Hygiene Dengan Kenyamanan Pasien Di Intensive Care Unit (Icu)mufarikaNo ratings yet
- Cot Demo Health 6-Guro21 - 3q - March 16 2023Document5 pagesCot Demo Health 6-Guro21 - 3q - March 16 2023Diego MapulaNo ratings yet
- New Policies and Protocol On Essential Intrapartal Newborn CareDocument4 pagesNew Policies and Protocol On Essential Intrapartal Newborn CareJam Chelsea ChyNo ratings yet
- Mohss Patient CharterDocument20 pagesMohss Patient Charternaango98No ratings yet
- Older Adults Group ProjectDocument12 pagesOlder Adults Group Projectapi-606630589No ratings yet
- En Do Vascular NeurosurgeryDocument285 pagesEn Do Vascular NeurosurgeryDaniel Silva Rodriguez100% (6)
- TELAAH KRITIS Penyebab Dan Faktor ResikoDocument7 pagesTELAAH KRITIS Penyebab Dan Faktor ResikoTri PutraNo ratings yet
- DCVMN Protocol - Version 1.0 - Dated 14th April 2023Document42 pagesDCVMN Protocol - Version 1.0 - Dated 14th April 2023gunjan.guptaNo ratings yet
- Present Score Target Week 1-2 Week 3-4 Monthly and ThereafterDocument2 pagesPresent Score Target Week 1-2 Week 3-4 Monthly and ThereafterFret Ramirez Coronia RNNo ratings yet
- Alternative To The BPW Students of University of Makati 2021 20222Document33 pagesAlternative To The BPW Students of University of Makati 2021 20222Study BuddyNo ratings yet
- Immunization Requirements For Students in K12 in Texas 2018Document4 pagesImmunization Requirements For Students in K12 in Texas 2018KCEN Channel 6No ratings yet
- Modern and Classic Wound Dressing Comparison in WoDocument6 pagesModern and Classic Wound Dressing Comparison in WoJuan LuckyNo ratings yet
- 03PDF Flow Chart For Telepractice HomeDocument1 page03PDF Flow Chart For Telepractice HomeValentina VallésNo ratings yet
- Environmental EpidemiologyDocument39 pagesEnvironmental EpidemiologyAbdu YesufNo ratings yet
- Mark Scheme (Results) May 2016: NQF BTEC Level 1/level 2 Firsts in Animal Care Unit 1: Animal Health (21883G)Document11 pagesMark Scheme (Results) May 2016: NQF BTEC Level 1/level 2 Firsts in Animal Care Unit 1: Animal Health (21883G)boho14No ratings yet
- Coding With ModifiersDocument144 pagesCoding With ModifiersRohan Kulkarni100% (2)

























































































Download as docx, pdf, or txt
NURSING CARE PLAN
(O.B.)
Submitted by: BSN 3Y2- 9B
Nesnel Martin
Katherine Mondero
Danity Medina
Aiza Osabel
Jave Miolata
Joana Matitu
Frederick Murillo
Ezalene Palo
Jaypee Tesalona
Mark Mercado
Neil Montefalcon
Christine Samin
Nico Manio
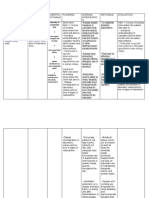
Assessment Background Diagnosis Planning Intervention Rationale Evaluation
knowledge
Decreased in Altered bowel After 8 hours of -Established -To gain cooperation After 8 hours
Subjective: normal movement nursing rapport to the through out the of nursing
“hirap akong frequency of related to intervention the client care. intervention
madumi ngayon ang defecation pregnancy as client will be the client were
tigas kasi minsan.” accompanied by evidenced by able to defecate -assess current -change in meal able to
As verbalized by the dry, hard stool. eating 3 meals atleast once in activity level and time, type of foods, defecate
client. in a day and my shift. tolerance in eating disruption of atleast once in
Increased insufficient unusual schedule my shift.
Objective: progesterone physical activity. can lead to
-Client in Regular level due to constipation.
diet Eating 100% pregnancy -encourage to take -easily soften the
3meals in a day. of atleast 8 glass stool and
of water /day. dehydration can
-Slow in general Decreased contribute to
movement even peristaltic constipation.
while at bed rest. movement of -encourage to eat -to increase
the Gastro or add in a diet peristaltic movement
Intestinal tract foods rich in fiber and soften the stool.
(fruits,cereals and
green leafy
Constipation vegetables.)
-encourage -ambulation
ambulation with strengthen the
assist in tolerance. abdominal muscle
that facilitates
defecation.
-evaluate -iron supplements
medication if any and other can
usage that may contribute to
contribute to constipation.
constipation.
Assessment Background Diagnosis Planning Intervention Rationale Evaluation
knowledge
Edema means Fluid Volume After 8 hours of -Established -To gain cooperation After 8 hours
Subjective: swelling in the Excess related Nursing rapport to the throughout the care. of Nursing
“nagmamanas yung small spaces to Pregnancy as Interventions client. Interventions
binti ko at paa.” that surround evidenced by the client will be -regular -to more accurately the client was
As verbalized by the the body tissues edema able to: monitoring of I&O determine the fluid able to:
patient. and organs. formation, visual and weight same excess.
Edema can changes and -maintain fluid time using hospital -maintained
Objective: occur nearly stretched shiny volume at a gowns everyday. fluid volume at
-visual anywhere in the skin. functional level. -encourage to -A high sodium level a functional
changes body. Reduce sodium causes or level.
-demonstrate a intake aggravates fluid
-edema formation Increased positive attitude In the diet. retention. -demonstrated
on progesterone toward the the positive
the lower level due to nurse’s -encourage -regular exercise attitude toward
extremities pregnancy. teaching. ambulation or stimulates the health
exercise. circulation. teaching.
-stretched shiny
skin. Increased
aldosterone that, -Elevation of the - stimulates excess
legs. Placing the fluid re-entry into
legs at least 12 the circulatory
Increased inches (30.5 cm) system
sodium (Na) and above the level of
water retention. the heart for 10-15
minutes, three to
four times a day.
Formation of -Use of support -it will compress the
Edema. stocking. Elastic leg vessels,
stockings. promoting
circulation and
decreasing
pooling of fluid due
to gravity.
- Massage the - Massaging the
affected part or body part can help
muscles. to stimulate the
release of excess
fluids, but should be
avoided if the
patient has blood
clots in the veins.
-Avoidance of -it facilitates
prolong standing formation of edema.
without moving.
Assessment Background Diagnosis Planning Intervention Rationale Evaluation
knowledge
High blood Ineffective After 8 hours of -Monitor VS -To identify After 8 hours of
Subjective: pressure tissue perfusion Nursing particular BP physiological Nursing
“nahihilo ako disorders of r/t constriction Intervention the responses Intervention the
masakit ulo at batok pregnancy. of blood vessel client will able to associated with client was able
ko “ as manifested display medical to display
“ang bilis kong Vasospasm by elevated hemodynamic conditions. hemodynamic
mapagod” Blood Pressure blood pressure blood pressure
As verbalized by the as evidenced by within normal -Monitor I/O -To determine within 130/80.
patient. discomfort due range or if not the fluid volume
Vasoconstriction to headache. decline into balance.
Of the blood 130/80.
Objective: vessel -Promote adequate -To maximize
rest by decreasing rest and sleep
-BP- 140/190 stimuli.
- Discomfort due to Decreased tissue -Encourage -To reduce
headache. perfusion relaxation anxiety
technique.
-Administer -To decrease
Decreased antihypertensive and control the
oxygen supply drug analgesic as Blood Pressure.
prescribed by the
physician
Decreased
Cardiac -Administer -To prevents or
Output(CO) magnesium sulfate control seizures
as ordered in pre-
eclampsia.
Increased blood
pressure
You might also like
- Nursing Care Plan - ConstipationDocument2 pagesNursing Care Plan - Constipationderic86% (72)
- Pre Reg Pharmacists Last MinuteDocument9 pagesPre Reg Pharmacists Last MinuteBob BobNo ratings yet
- Nursing Care Plan ConstipationDocument2 pagesNursing Care Plan ConstipationkazelleNo ratings yet
- Nursing Care Plan: Short Term: Difficulty in Swallowing Nursing Diagnosis Planning Implementation Rationale EvaluationDocument6 pagesNursing Care Plan: Short Term: Difficulty in Swallowing Nursing Diagnosis Planning Implementation Rationale EvaluationNico Angelo Hibaya TugononNo ratings yet
- Nursing Care Plan Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective: Short Term Goal: IndependentDocument2 pagesNursing Care Plan Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective: Short Term Goal: IndependentEva Marielle CezaldoNo ratings yet
- Bowel Incontinence ConstipationDocument3 pagesBowel Incontinence ConstipationMatty-b AskalaniNo ratings yet
- Diarrhea Nursing Care PlanDocument2 pagesDiarrhea Nursing Care PlanKrizha Angela NicolasNo ratings yet
- Nursing Problem Explanation Goal Intervention Rationale Evaluation SubjectiveDocument1 pageNursing Problem Explanation Goal Intervention Rationale Evaluation SubjectiveZed P. EstalillaNo ratings yet
- DiarrheaDocument3 pagesDiarrheaBert GasalNo ratings yet
- ConstipationDocument4 pagesConstipationprincess_bee100% (1)
- Constipation LeukemiaDocument1 pageConstipation LeukemiamawelNo ratings yet
- Constipation NCPDocument3 pagesConstipation NCPIRISH CACAYANNo ratings yet
- NCP ConstipationDocument2 pagesNCP ConstipationFaith Bingan Remiscal67% (6)
- Constipation NCPDocument2 pagesConstipation NCPAbby GonzalesNo ratings yet
- Assessment Diagnosis Planning Implementation Rationale Evaluation Subjective Data: Objective Data: Short Term: Independent: Short Term: Goal Partially MetDocument3 pagesAssessment Diagnosis Planning Implementation Rationale Evaluation Subjective Data: Objective Data: Short Term: Independent: Short Term: Goal Partially MetCess YNo ratings yet
- "Nagtatae Siya 4 Days Na" As Verbalized by The Mother. Inatake of Causative Agents Irritation of The Stomach Inflammation of The Stomach Increase GI Motility DiarrrheaDocument4 pages"Nagtatae Siya 4 Days Na" As Verbalized by The Mother. Inatake of Causative Agents Irritation of The Stomach Inflammation of The Stomach Increase GI Motility DiarrrheaMelissa MhelNo ratings yet
- A Nursing Care Plan On: Loose Bowel MovementDocument6 pagesA Nursing Care Plan On: Loose Bowel MovementakoitsmeNo ratings yet
- Name: de Guzman, Cameron Josh B. Section: 2Bsn-ADocument3 pagesName: de Guzman, Cameron Josh B. Section: 2Bsn-ACameron De GuzmanNo ratings yet
- Assessment Healt H Patte RN Nursing Diagnosis Desired Outcome (Edit) Intervention (Edit) Evaluation (EDIT) Rema RKSDocument3 pagesAssessment Healt H Patte RN Nursing Diagnosis Desired Outcome (Edit) Intervention (Edit) Evaluation (EDIT) Rema RKStflorenzNo ratings yet
- College of Nursing: Assessment Diagnosis Analysis Planning Implementation Rationale EvaluationDocument2 pagesCollege of Nursing: Assessment Diagnosis Analysis Planning Implementation Rationale EvaluationDiana Anne MarisNo ratings yet
- College of Nursing: Assessment Diagnosis Analysis Planning Implementation Rationale EvaluationDocument2 pagesCollege of Nursing: Assessment Diagnosis Analysis Planning Implementation Rationale EvaluationjoanneNo ratings yet
- NCP 1Document2 pagesNCP 1Cedmarc Francis RenionNo ratings yet
- Maraming Tubig at Kakain NG Prutas para Makadumi Ako."Document2 pagesMaraming Tubig at Kakain NG Prutas para Makadumi Ako."Cayla Mae CarlosNo ratings yet
- PeristalticDocument2 pagesPeristalticAllyzah Faith BernalesNo ratings yet
- Nursing Care Plan 1BSN 14 Group 1Document8 pagesNursing Care Plan 1BSN 14 Group 1Mikaella GacostaNo ratings yet
- ConstipationDocument2 pagesConstipationjinsi georgeNo ratings yet
- NCP Ruth DeveraDocument8 pagesNCP Ruth DeveraBESA JERIC FLORESNo ratings yet
- Risk For Constipation Nursing Care Plan Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective Data: Independent: Goal MetDocument10 pagesRisk For Constipation Nursing Care Plan Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective Data: Independent: Goal MetHydie Mae AlcabedosNo ratings yet
- Nursing Care Plan ConstipationDocument2 pagesNursing Care Plan ConstipationGio Baduria100% (1)
- ConstipationDocument3 pagesConstipationmyer pasandalanNo ratings yet
- Any Up-Dates Are To Be Completed in Different Color Ink. The Student Is Expected To Document All Meds The Client Is Currently ReceivingDocument1 pageAny Up-Dates Are To Be Completed in Different Color Ink. The Student Is Expected To Document All Meds The Client Is Currently Receivinggeorgeloto12No ratings yet
- CARE PLAN Format - ConstipationDocument2 pagesCARE PLAN Format - Constipationjinsi georgeNo ratings yet
- University of The East Ramon Magsaysay Memorial Medical Center, Inc. College of NursingDocument23 pagesUniversity of The East Ramon Magsaysay Memorial Medical Center, Inc. College of NursingReina RamonesNo ratings yet
- NCP Risk For ConstipationDocument1 pageNCP Risk For Constipationjorgeacct50% (4)
- NCP3Document4 pagesNCP3Noreen GyleNo ratings yet
- Nursing Care Plan Assessment Diagnosis Outcome Intervention Rationale EvaluationDocument3 pagesNursing Care Plan Assessment Diagnosis Outcome Intervention Rationale EvaluationMarivic Yuson MalagarNo ratings yet
- CHOLELITHIASISDocument4 pagesCHOLELITHIASISKate ValdesNo ratings yet
- Discharge Planning and NCP SDocument8 pagesDischarge Planning and NCP SRainier RamosNo ratings yet
- COLON CANCER NCP-impaired nutrITIONDocument3 pagesCOLON CANCER NCP-impaired nutrITIONNicole cuencosNo ratings yet
- NCP WilliamDocument2 pagesNCP WilliamApril Louise PaluganNo ratings yet
- DIARRHEADocument2 pagesDIARRHEADanielNo ratings yet
- Assessment Diagnosis Inference Planning Intervention Rationale EvaluationDocument1 pageAssessment Diagnosis Inference Planning Intervention Rationale EvaluationLoverMind CabaronNo ratings yet
- NCP DiverticulitisDocument6 pagesNCP DiverticulitisLovely Cacapit100% (1)
- Viii. Nursing Care Plan: Asessment Diagnosis Planning Intervention Rationale EvaluationDocument3 pagesViii. Nursing Care Plan: Asessment Diagnosis Planning Intervention Rationale Evaluationhehehe29No ratings yet
- Assessment Diagnosis Planning Implementation Rationale Evaluation Subjective Data: Short Term: Independent: Short Term: Goal Partially MetDocument3 pagesAssessment Diagnosis Planning Implementation Rationale Evaluation Subjective Data: Short Term: Independent: Short Term: Goal Partially MetPrincess Mildred AbdonNo ratings yet
- Constipation NCPDocument3 pagesConstipation NCPSeth Amiel MotaNo ratings yet
- Name: Babu Kaji Maharjan: Patient's IdentificationDocument6 pagesName: Babu Kaji Maharjan: Patient's IdentificationAlisha MaharjanNo ratings yet
- NCP JaundiceDocument9 pagesNCP JaundiceMeena Koushal100% (1)
- CHA NCPDocument6 pagesCHA NCPMonty_Legaspi_5664No ratings yet
- Digestive System Nursing Diagnoses & Care PlansDocument7 pagesDigestive System Nursing Diagnoses & Care PlansyormahdNo ratings yet
- New Intestinal ObstructionDocument12 pagesNew Intestinal Obstructionmustafalotfy01No ratings yet
- NCP (Diarrhea)Document2 pagesNCP (Diarrhea)Rodj Bilang Jr.83% (30)
- Nursing Care Plan: Assessment Nursing Diagnosis Rationale Desired Outcome Nursing Intervention Justification EvaluationDocument2 pagesNursing Care Plan: Assessment Nursing Diagnosis Rationale Desired Outcome Nursing Intervention Justification EvaluationDan MandigNo ratings yet
- Food Is Figureoutable: AN ESSENTIAL GUIDE TO BODY SYSTEMSFrom EverandFood Is Figureoutable: AN ESSENTIAL GUIDE TO BODY SYSTEMSNo ratings yet
- Intestinal Failure: Diagnosis, Management and TransplantationFrom EverandIntestinal Failure: Diagnosis, Management and TransplantationAlan LangnasNo ratings yet
- Intermittent Fasting: The Most Effective Diet, the Healthiest LifestyleFrom EverandIntermittent Fasting: The Most Effective Diet, the Healthiest LifestyleNo ratings yet
- Natural Cures for Constipation: Curing Constipation PermanentlyFrom EverandNatural Cures for Constipation: Curing Constipation PermanentlyNo ratings yet
- Health Education PlanDocument3 pagesHealth Education PlanCamille VegaNo ratings yet
- Minutes of 290th Meeting of Registration BoardDocument1,286 pagesMinutes of 290th Meeting of Registration BoardUsman DarNo ratings yet
- Jurnal Tonsil Limfoma Non HodgkinDocument5 pagesJurnal Tonsil Limfoma Non HodgkinAhmad RamadhanuNo ratings yet
- Recommendations For Infection Control For The Practice of AnesthesiologyDocument86 pagesRecommendations For Infection Control For The Practice of AnesthesiologyAhmed MostafaNo ratings yet
- CandidiasisDocument27 pagesCandidiasisBhavesh SippyNo ratings yet
- Client Consultation Form - Pedicure AppoinmentDocument3 pagesClient Consultation Form - Pedicure AppoinmentMicheal McDowellNo ratings yet
- 1 Hospital Organisation & FunctionDocument16 pages1 Hospital Organisation & FunctionAtrao67% (3)
- Makalah Komplementer Pada Masa NifasDocument7 pagesMakalah Komplementer Pada Masa NifasWirda TariNo ratings yet
- A Review of Classification of Disease in AyurvedaDocument11 pagesA Review of Classification of Disease in AyurvedaEditor_IAIMNo ratings yet
- FLCCC Alliance Frequently Asked Questions On IvermectinDocument12 pagesFLCCC Alliance Frequently Asked Questions On IvermectinAndrés Mario Rivera RojasNo ratings yet
- CC C C: 1. Rapid Changes in Health Care Technology and Therapiesc " C CDocument18 pagesCC C C: 1. Rapid Changes in Health Care Technology and Therapiesc " C CEric Blahhal100% (6)
- Jurnal Transfusi Darah 2Document11 pagesJurnal Transfusi Darah 2widiamNo ratings yet
- Failure To Thrive JournalDocument13 pagesFailure To Thrive JournalApRil Anne BalanonNo ratings yet
- Oral Hygiene Dengan Kenyamanan Pasien Di Intensive Care Unit (Icu)Document13 pagesOral Hygiene Dengan Kenyamanan Pasien Di Intensive Care Unit (Icu)mufarikaNo ratings yet
- Cot Demo Health 6-Guro21 - 3q - March 16 2023Document5 pagesCot Demo Health 6-Guro21 - 3q - March 16 2023Diego MapulaNo ratings yet
- New Policies and Protocol On Essential Intrapartal Newborn CareDocument4 pagesNew Policies and Protocol On Essential Intrapartal Newborn CareJam Chelsea ChyNo ratings yet
- Mohss Patient CharterDocument20 pagesMohss Patient Charternaango98No ratings yet
- Older Adults Group ProjectDocument12 pagesOlder Adults Group Projectapi-606630589No ratings yet
- En Do Vascular NeurosurgeryDocument285 pagesEn Do Vascular NeurosurgeryDaniel Silva Rodriguez100% (6)
- TELAAH KRITIS Penyebab Dan Faktor ResikoDocument7 pagesTELAAH KRITIS Penyebab Dan Faktor ResikoTri PutraNo ratings yet
- DCVMN Protocol - Version 1.0 - Dated 14th April 2023Document42 pagesDCVMN Protocol - Version 1.0 - Dated 14th April 2023gunjan.guptaNo ratings yet
- Present Score Target Week 1-2 Week 3-4 Monthly and ThereafterDocument2 pagesPresent Score Target Week 1-2 Week 3-4 Monthly and ThereafterFret Ramirez Coronia RNNo ratings yet
- Alternative To The BPW Students of University of Makati 2021 20222Document33 pagesAlternative To The BPW Students of University of Makati 2021 20222Study BuddyNo ratings yet
- Immunization Requirements For Students in K12 in Texas 2018Document4 pagesImmunization Requirements For Students in K12 in Texas 2018KCEN Channel 6No ratings yet
- Modern and Classic Wound Dressing Comparison in WoDocument6 pagesModern and Classic Wound Dressing Comparison in WoJuan LuckyNo ratings yet
- 03PDF Flow Chart For Telepractice HomeDocument1 page03PDF Flow Chart For Telepractice HomeValentina VallésNo ratings yet
- Environmental EpidemiologyDocument39 pagesEnvironmental EpidemiologyAbdu YesufNo ratings yet
- Mark Scheme (Results) May 2016: NQF BTEC Level 1/level 2 Firsts in Animal Care Unit 1: Animal Health (21883G)Document11 pagesMark Scheme (Results) May 2016: NQF BTEC Level 1/level 2 Firsts in Animal Care Unit 1: Animal Health (21883G)boho14No ratings yet
- Coding With ModifiersDocument144 pagesCoding With ModifiersRohan Kulkarni100% (2)