
Tuberculosis Update Appendix d92
Tuberculosis Update Appendix d92
You might also like
- Mycoses - 2023 - Kato - A Systematic Review and Meta Analysis of Efficacy and Safety of Isavuconazole For The Treatment andDocument10 pagesMycoses - 2023 - Kato - A Systematic Review and Meta Analysis of Efficacy and Safety of Isavuconazole For The Treatment andc gNo ratings yet
- Cairo: Pilbeam's Mechanical Ventilation, 6th EditionDocument6 pagesCairo: Pilbeam's Mechanical Ventilation, 6th Editionفاتن المطيريNo ratings yet
- Test - Mark Klimek Yellow Book (KV) - QuizletDocument62 pagesTest - Mark Klimek Yellow Book (KV) - QuizletRonelyn Rachelle CabcabanNo ratings yet
- AdherenceDocument8 pagesAdherenceAbdurhman SeidNo ratings yet
- Short-Course Intraabdominal InfectionDocument10 pagesShort-Course Intraabdominal Infectionnicolás idárragaNo ratings yet
- TamifluDocument6 pagesTamifluFitri CwetzNo ratings yet
- Dafpus Tb-Hiv Ped2Document4 pagesDafpus Tb-Hiv Ped2Anonymous S0MyRHNo ratings yet
- Trial of Short-Course Antimicrobial Therapy For Intraabdominal InfectionDocument10 pagesTrial of Short-Course Antimicrobial Therapy For Intraabdominal InfectionMeygan CórdovaNo ratings yet
- Tele The Ruthr AbotuDocument5 pagesTele The Ruthr AbotukhanjanNo ratings yet
- JurnalDocument2 pagesJurnalHamba AllahNo ratings yet
- Efficacy and Safety of Abatacept in Lupus Nephritis: A Twelve-Month, Randomized, Double-Blind StudyDocument11 pagesEfficacy and Safety of Abatacept in Lupus Nephritis: A Twelve-Month, Randomized, Double-Blind StudyAndreea AdaNo ratings yet
- Population Pharmacokinetics of Paritaprevir, Ombitasvir, Dasabuvir, Ritonavir, and Ribavirin in Patients With Hepatitis C Virus Genotype 1 InfectionDocument11 pagesPopulation Pharmacokinetics of Paritaprevir, Ombitasvir, Dasabuvir, Ritonavir, and Ribavirin in Patients With Hepatitis C Virus Genotype 1 InfectionBagoes AsNo ratings yet
- Four-Month Moxifloxacin-Based Regimens For Drug-Sensitive TuberculosisDocument9 pagesFour-Month Moxifloxacin-Based Regimens For Drug-Sensitive TuberculosisTheodoraAnamariaNo ratings yet
- Sofosbuvir For Previously Untreated Chronic Hepatitis C InfectionDocument10 pagesSofosbuvir For Previously Untreated Chronic Hepatitis C InfectionSitta Grewo LiandarNo ratings yet
- Safety and Immunogenicity of Inactivated Hepatitis A Vaccine in Patients With Chronic Liver DiseaseDocument4 pagesSafety and Immunogenicity of Inactivated Hepatitis A Vaccine in Patients With Chronic Liver DiseaseShuaib AhmedNo ratings yet
- 10.1007 - s00405 002 0524 4Document5 pages10.1007 - s00405 002 0524 4Niar PramudyaningrumNo ratings yet
- 4-On 3-Off Journal Handout 3Document2 pages4-On 3-Off Journal Handout 3api-594366475No ratings yet
- Kiteria Inklusi & EkslusiDocument8 pagesKiteria Inklusi & EkslusiDorothy Karya Yogi LubisNo ratings yet
- Volume Probiotic Adjuvant Therapy Chronic Urticaria 4842allasp1Document8 pagesVolume Probiotic Adjuvant Therapy Chronic Urticaria 4842allasp1fatima amaliaNo ratings yet
- Divya Thesis Final (30th Jan)Document26 pagesDivya Thesis Final (30th Jan)smalaparaNo ratings yet
- Cancers 08 00084Document10 pagesCancers 08 00084Benny Chris TantoNo ratings yet
- Correlation Between HLA Haplotypes and TheDocument5 pagesCorrelation Between HLA Haplotypes and TheNaziBrola TsivadzeNo ratings yet
- Sharma 2002Document4 pagesSharma 2002wosen wondNo ratings yet
- New England Journal Medicine: The ofDocument11 pagesNew England Journal Medicine: The ofFransisca PekertiNo ratings yet
- Original Article LongActing Cabotegravir and Rilpivirine For Maintanance of HIV1 SupressionDocument12 pagesOriginal Article LongActing Cabotegravir and Rilpivirine For Maintanance of HIV1 SupressionAdevilianiNo ratings yet
- New England Journal Medicine: The ofDocument11 pagesNew England Journal Medicine: The ofprabuNo ratings yet
- Jamainternal Gopalan 2018 Oi 180003Document9 pagesJamainternal Gopalan 2018 Oi 180003pentaxNo ratings yet
- ShingrixDocument6 pagesShingrixMarcus YoonNo ratings yet
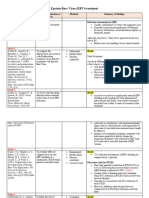
- Epstein-Barr Virus (EBV) Treatment: Study - Authors & Date Purpose of Evaluation or Research Methods Summary of FindingsDocument3 pagesEpstein-Barr Virus (EBV) Treatment: Study - Authors & Date Purpose of Evaluation or Research Methods Summary of Findingsapi-719803017No ratings yet
- Complementary Therapies in Medicine: Contents Lists Available atDocument13 pagesComplementary Therapies in Medicine: Contents Lists Available atAndi UmmahNo ratings yet
- Sofosbuvir For Previously Untreated Chronic Hepatitis C InfectionDocument23 pagesSofosbuvir For Previously Untreated Chronic Hepatitis C InfectionalfianfirdausNo ratings yet
- Ibru Benda Rituxi For Mantle Cell Lymphoma NEJMDocument13 pagesIbru Benda Rituxi For Mantle Cell Lymphoma NEJMMiriam AguilarNo ratings yet
- Dooley 2020Document9 pagesDooley 2020wahyuni yuniNo ratings yet
- Antifungal Treatment in Sarcoidosis A Pilot Intervent 2007 Respiratory MedicDocument5 pagesAntifungal Treatment in Sarcoidosis A Pilot Intervent 2007 Respiratory MedicTomasNo ratings yet
- Chou 2013Document19 pagesChou 2013rajeshskNo ratings yet
- Jurding Alergi - Adinda - Bismillah - OktoberDocument56 pagesJurding Alergi - Adinda - Bismillah - OktoberAdinda ParamarthaNo ratings yet
- RajaniDocument8 pagesRajaniArnette Castro de GuzmanNo ratings yet
- Betahistine Dihydrochloride in The Treatment of Peripheral Vestibular VertigoDocument6 pagesBetahistine Dihydrochloride in The Treatment of Peripheral Vestibular VertigoRidho HidayatullohNo ratings yet
- Natali Zuma BDocument6 pagesNatali Zuma BsarahmooNo ratings yet
- Trial of Short-Course Antimicrobial Therapy For IntraabdominalDocument15 pagesTrial of Short-Course Antimicrobial Therapy For IntraabdominalJohn TusselNo ratings yet
- HIV-1 Antiretroviral Resistance in Cuba, 2009-2014Document7 pagesHIV-1 Antiretroviral Resistance in Cuba, 2009-2014Yoan Alemán CamposNo ratings yet
- HeplisavDocument10 pagesHeplisavAngie GarciaNo ratings yet
- Acute Inflammatory: Laparoscopically (Salpingitis)Document7 pagesAcute Inflammatory: Laparoscopically (Salpingitis)Bella Ika LestariNo ratings yet
- Aps Ustekinumab Falla TNFDocument10 pagesAps Ustekinumab Falla TNFLeonardo GarciaNo ratings yet
- Long-Term Impact of Acyclovir Suppressive Therapy On Genital and Plasma HIV RNA in Tanzanian Women: A Randomized Controlled TrialDocument14 pagesLong-Term Impact of Acyclovir Suppressive Therapy On Genital and Plasma HIV RNA in Tanzanian Women: A Randomized Controlled TrialEpi PanjaitanNo ratings yet
- Dennis Slamon Ribociclib Plus Endocrine Therapy inDocument12 pagesDennis Slamon Ribociclib Plus Endocrine Therapy inandre.manzanoqNo ratings yet
- Bmjopen 2016 015233Document7 pagesBmjopen 2016 015233SEPTIANA SAPUTRINo ratings yet
- Beclabuvir in Combination With Asunaprevir and Daclatasvir For Hepatitis C Virus Genotype 1 InfectionDocument12 pagesBeclabuvir in Combination With Asunaprevir and Daclatasvir For Hepatitis C Virus Genotype 1 Infectiontruongduyhieu1311No ratings yet
- Randomized Clinical Trial of Antibiotic Therapy ForDocument5 pagesRandomized Clinical Trial of Antibiotic Therapy ForjimenacuadradoanguloNo ratings yet
- Zac 3843Document10 pagesZac 3843Juliän VillamizarNo ratings yet
- Predictors of Success With Highly Active Antiretroviral Therapy in An Antiretroviral-Naive Urban PopulationDocument6 pagesPredictors of Success With Highly Active Antiretroviral Therapy in An Antiretroviral-Naive Urban PopulationMuhammad Hafidzul HairulNo ratings yet
- Atorvastatin Improves Sputum Conversion and Chest X-Ray Severity ScoreDocument6 pagesAtorvastatin Improves Sputum Conversion and Chest X-Ray Severity Scorecharmainemargaret.parreno.medNo ratings yet
- HAI Guidelines 2010Document21 pagesHAI Guidelines 2010Mario Suarez MontalvoNo ratings yet
- Prevalence of Mutations Conferring Resistance Among Multi-And Extensively Drug-Resistant Mycobacterium Tuberculosis Isolates in ChinaDocument4 pagesPrevalence of Mutations Conferring Resistance Among Multi-And Extensively Drug-Resistant Mycobacterium Tuberculosis Isolates in ChinaKartikeya SinghNo ratings yet
- Revision de LesDocument12 pagesRevision de Lesroberto mendezNo ratings yet
- Tofacitinib As Induction and Maintenance Therapy For Ulcerative ColitisDocument14 pagesTofacitinib As Induction and Maintenance Therapy For Ulcerative Colitismichal ben meronNo ratings yet
- Oral Direct Acting Agent Therapy For Hepatitis C Virus Infection A Systematic ReviewDocument13 pagesOral Direct Acting Agent Therapy For Hepatitis C Virus Infection A Systematic ReviewRoberto López MataNo ratings yet
- RSV Vaccine Journal ClubDocument18 pagesRSV Vaccine Journal Clubapi-719803017100% (1)
- Krishna 26pDocument29 pagesKrishna 26pyanshutradelink.pvtNo ratings yet
- Brmedj00461 0017Document4 pagesBrmedj00461 0017muhammad24fayazNo ratings yet
- GastroparesisDocument4 pagesGastroparesisnadNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 5: GastrointestinalFrom EverandComplementary and Alternative Medical Lab Testing Part 5: GastrointestinalNo ratings yet
- Assessment and Management of Patients With Hepatic DisordersDocument3 pagesAssessment and Management of Patients With Hepatic DisordersaliNo ratings yet
- Acyanotic CHD-obstructiveDocument39 pagesAcyanotic CHD-obstructiveEbuka AniNo ratings yet
- Passmedicine MRCP Notes-Palliative Medicine and End of Life CareDocument5 pagesPassmedicine MRCP Notes-Palliative Medicine and End of Life CareMayar WaelNo ratings yet
- COVID-19: PandemicDocument39 pagesCOVID-19: PandemicGuillermo Rodriguez LopezNo ratings yet
- Exercise 1. Complete The Text Using The Words From The BoxDocument5 pagesExercise 1. Complete The Text Using The Words From The BoxВлада ВоеводинаNo ratings yet
- hs486 Document OSHA Recording Work-Related Injuries and IllnessesDocument13 pageshs486 Document OSHA Recording Work-Related Injuries and Illnessesfatmata koromaNo ratings yet
- Smoking Is DangerousDocument3 pagesSmoking Is DangerousAbdulmalkNo ratings yet
- Depressed People of The Bible Freedom From A Cave of Depression To The Light of Life (Jeff Zaremsky) (Z-Library)Document167 pagesDepressed People of The Bible Freedom From A Cave of Depression To The Light of Life (Jeff Zaremsky) (Z-Library)Isaac GisoreNo ratings yet
- Evd Evd Evd Evd Accudrain Accudrain Accudrain Accudrain: External Ventricular DeviceDocument1 pageEvd Evd Evd Evd Accudrain Accudrain Accudrain Accudrain: External Ventricular DeviceQueenNo ratings yet
- 7-5 (Nhóm 7)Document7 pages7-5 (Nhóm 7)Nguyễn Văn VượngNo ratings yet
- 17 ADD Type TestDocument7 pages17 ADD Type TestEvandro Pinho0% (1)
- The Complete Guide To Weight Loss and FitnessDocument4 pagesThe Complete Guide To Weight Loss and FitnessOnika BoteroNo ratings yet
- Tribute ofDocument10 pagesTribute ofAlvaro Andres Flores JimenezNo ratings yet
- English Conversation Discussion About AllergiesDocument3 pagesEnglish Conversation Discussion About AllergiesKevin ScottNo ratings yet
- TriageDocument37 pagesTriagekyuleen05No ratings yet
- Instant Download Ebook PDF Foundations of Nursing Enrolled Division 2 Nurses 1st Edition PDF ScribdDocument41 pagesInstant Download Ebook PDF Foundations of Nursing Enrolled Division 2 Nurses 1st Edition PDF Scribddanny.bradt610100% (48)
- ANA101 Respiratory System DR GIEDocument44 pagesANA101 Respiratory System DR GIEMarian Kyla MarianoNo ratings yet
- Scrotal Conditions: Done By: Enas Almazraway Sarah Al-HawamdehDocument65 pagesScrotal Conditions: Done By: Enas Almazraway Sarah Al-HawamdehMohammad GharaibehNo ratings yet
- LD Final PriyankaDocument108 pagesLD Final PriyankaPriyanka GandhiNo ratings yet
- Drug Induced Movement DisordersDocument65 pagesDrug Induced Movement DisordersShaunak Patil100% (1)
- Clin Transl Allergy (2019)Document7 pagesClin Transl Allergy (2019)Nimesh ModiNo ratings yet
- 1439019766-7. Nursing - Couvade Syndrome - Bency AbrahamDocument4 pages1439019766-7. Nursing - Couvade Syndrome - Bency AbrahamGeorgi GugicevNo ratings yet
- Daftar Pasien Neurologi RABU 22 APRIL 2020: Lontara 3 Saraf Kamar 1Document4 pagesDaftar Pasien Neurologi RABU 22 APRIL 2020: Lontara 3 Saraf Kamar 1Ilham Habib DjarkoniNo ratings yet
- The Marketing Experiment of Melody ToffeeDocument13 pagesThe Marketing Experiment of Melody ToffeeRishabh RajNo ratings yet
- 0 - Locally Endemic and Communicable Diseases-1Document10 pages0 - Locally Endemic and Communicable Diseases-1jonaNo ratings yet
- Group 3 Diabetes MellitusDocument9 pagesGroup 3 Diabetes MellitusMary0% (1)
- ĐỀ THI THỬ- TRƯỜNGDocument4 pagesĐỀ THI THỬ- TRƯỜNGAdiecenNo ratings yet
- Feyer 2020 WvngoshawkDocument13 pagesFeyer 2020 WvngoshawkAgnieszka CzujkowskaNo ratings yet

























































































Download as pdf or txt
You might also like
- Mycoses - 2023 - Kato - A Systematic Review and Meta Analysis of Efficacy and Safety of Isavuconazole For The Treatment andDocument10 pagesMycoses - 2023 - Kato - A Systematic Review and Meta Analysis of Efficacy and Safety of Isavuconazole For The Treatment andc gNo ratings yet
- Cairo: Pilbeam's Mechanical Ventilation, 6th EditionDocument6 pagesCairo: Pilbeam's Mechanical Ventilation, 6th Editionفاتن المطيريNo ratings yet
- Test - Mark Klimek Yellow Book (KV) - QuizletDocument62 pagesTest - Mark Klimek Yellow Book (KV) - QuizletRonelyn Rachelle CabcabanNo ratings yet
- AdherenceDocument8 pagesAdherenceAbdurhman SeidNo ratings yet
- Short-Course Intraabdominal InfectionDocument10 pagesShort-Course Intraabdominal Infectionnicolás idárragaNo ratings yet
- TamifluDocument6 pagesTamifluFitri CwetzNo ratings yet
- Dafpus Tb-Hiv Ped2Document4 pagesDafpus Tb-Hiv Ped2Anonymous S0MyRHNo ratings yet
- Trial of Short-Course Antimicrobial Therapy For Intraabdominal InfectionDocument10 pagesTrial of Short-Course Antimicrobial Therapy For Intraabdominal InfectionMeygan CórdovaNo ratings yet
- Tele The Ruthr AbotuDocument5 pagesTele The Ruthr AbotukhanjanNo ratings yet
- JurnalDocument2 pagesJurnalHamba AllahNo ratings yet
- Efficacy and Safety of Abatacept in Lupus Nephritis: A Twelve-Month, Randomized, Double-Blind StudyDocument11 pagesEfficacy and Safety of Abatacept in Lupus Nephritis: A Twelve-Month, Randomized, Double-Blind StudyAndreea AdaNo ratings yet
- Population Pharmacokinetics of Paritaprevir, Ombitasvir, Dasabuvir, Ritonavir, and Ribavirin in Patients With Hepatitis C Virus Genotype 1 InfectionDocument11 pagesPopulation Pharmacokinetics of Paritaprevir, Ombitasvir, Dasabuvir, Ritonavir, and Ribavirin in Patients With Hepatitis C Virus Genotype 1 InfectionBagoes AsNo ratings yet
- Four-Month Moxifloxacin-Based Regimens For Drug-Sensitive TuberculosisDocument9 pagesFour-Month Moxifloxacin-Based Regimens For Drug-Sensitive TuberculosisTheodoraAnamariaNo ratings yet
- Sofosbuvir For Previously Untreated Chronic Hepatitis C InfectionDocument10 pagesSofosbuvir For Previously Untreated Chronic Hepatitis C InfectionSitta Grewo LiandarNo ratings yet
- Safety and Immunogenicity of Inactivated Hepatitis A Vaccine in Patients With Chronic Liver DiseaseDocument4 pagesSafety and Immunogenicity of Inactivated Hepatitis A Vaccine in Patients With Chronic Liver DiseaseShuaib AhmedNo ratings yet
- 10.1007 - s00405 002 0524 4Document5 pages10.1007 - s00405 002 0524 4Niar PramudyaningrumNo ratings yet
- 4-On 3-Off Journal Handout 3Document2 pages4-On 3-Off Journal Handout 3api-594366475No ratings yet
- Kiteria Inklusi & EkslusiDocument8 pagesKiteria Inklusi & EkslusiDorothy Karya Yogi LubisNo ratings yet
- Volume Probiotic Adjuvant Therapy Chronic Urticaria 4842allasp1Document8 pagesVolume Probiotic Adjuvant Therapy Chronic Urticaria 4842allasp1fatima amaliaNo ratings yet
- Divya Thesis Final (30th Jan)Document26 pagesDivya Thesis Final (30th Jan)smalaparaNo ratings yet
- Cancers 08 00084Document10 pagesCancers 08 00084Benny Chris TantoNo ratings yet
- Correlation Between HLA Haplotypes and TheDocument5 pagesCorrelation Between HLA Haplotypes and TheNaziBrola TsivadzeNo ratings yet
- Sharma 2002Document4 pagesSharma 2002wosen wondNo ratings yet
- New England Journal Medicine: The ofDocument11 pagesNew England Journal Medicine: The ofFransisca PekertiNo ratings yet
- Original Article LongActing Cabotegravir and Rilpivirine For Maintanance of HIV1 SupressionDocument12 pagesOriginal Article LongActing Cabotegravir and Rilpivirine For Maintanance of HIV1 SupressionAdevilianiNo ratings yet
- New England Journal Medicine: The ofDocument11 pagesNew England Journal Medicine: The ofprabuNo ratings yet
- Jamainternal Gopalan 2018 Oi 180003Document9 pagesJamainternal Gopalan 2018 Oi 180003pentaxNo ratings yet
- ShingrixDocument6 pagesShingrixMarcus YoonNo ratings yet
- Epstein-Barr Virus (EBV) Treatment: Study - Authors & Date Purpose of Evaluation or Research Methods Summary of FindingsDocument3 pagesEpstein-Barr Virus (EBV) Treatment: Study - Authors & Date Purpose of Evaluation or Research Methods Summary of Findingsapi-719803017No ratings yet
- Complementary Therapies in Medicine: Contents Lists Available atDocument13 pagesComplementary Therapies in Medicine: Contents Lists Available atAndi UmmahNo ratings yet
- Sofosbuvir For Previously Untreated Chronic Hepatitis C InfectionDocument23 pagesSofosbuvir For Previously Untreated Chronic Hepatitis C InfectionalfianfirdausNo ratings yet
- Ibru Benda Rituxi For Mantle Cell Lymphoma NEJMDocument13 pagesIbru Benda Rituxi For Mantle Cell Lymphoma NEJMMiriam AguilarNo ratings yet
- Dooley 2020Document9 pagesDooley 2020wahyuni yuniNo ratings yet
- Antifungal Treatment in Sarcoidosis A Pilot Intervent 2007 Respiratory MedicDocument5 pagesAntifungal Treatment in Sarcoidosis A Pilot Intervent 2007 Respiratory MedicTomasNo ratings yet
- Chou 2013Document19 pagesChou 2013rajeshskNo ratings yet
- Jurding Alergi - Adinda - Bismillah - OktoberDocument56 pagesJurding Alergi - Adinda - Bismillah - OktoberAdinda ParamarthaNo ratings yet
- RajaniDocument8 pagesRajaniArnette Castro de GuzmanNo ratings yet
- Betahistine Dihydrochloride in The Treatment of Peripheral Vestibular VertigoDocument6 pagesBetahistine Dihydrochloride in The Treatment of Peripheral Vestibular VertigoRidho HidayatullohNo ratings yet
- Natali Zuma BDocument6 pagesNatali Zuma BsarahmooNo ratings yet
- Trial of Short-Course Antimicrobial Therapy For IntraabdominalDocument15 pagesTrial of Short-Course Antimicrobial Therapy For IntraabdominalJohn TusselNo ratings yet
- HIV-1 Antiretroviral Resistance in Cuba, 2009-2014Document7 pagesHIV-1 Antiretroviral Resistance in Cuba, 2009-2014Yoan Alemán CamposNo ratings yet
- HeplisavDocument10 pagesHeplisavAngie GarciaNo ratings yet
- Acute Inflammatory: Laparoscopically (Salpingitis)Document7 pagesAcute Inflammatory: Laparoscopically (Salpingitis)Bella Ika LestariNo ratings yet
- Aps Ustekinumab Falla TNFDocument10 pagesAps Ustekinumab Falla TNFLeonardo GarciaNo ratings yet
- Long-Term Impact of Acyclovir Suppressive Therapy On Genital and Plasma HIV RNA in Tanzanian Women: A Randomized Controlled TrialDocument14 pagesLong-Term Impact of Acyclovir Suppressive Therapy On Genital and Plasma HIV RNA in Tanzanian Women: A Randomized Controlled TrialEpi PanjaitanNo ratings yet
- Dennis Slamon Ribociclib Plus Endocrine Therapy inDocument12 pagesDennis Slamon Ribociclib Plus Endocrine Therapy inandre.manzanoqNo ratings yet
- Bmjopen 2016 015233Document7 pagesBmjopen 2016 015233SEPTIANA SAPUTRINo ratings yet
- Beclabuvir in Combination With Asunaprevir and Daclatasvir For Hepatitis C Virus Genotype 1 InfectionDocument12 pagesBeclabuvir in Combination With Asunaprevir and Daclatasvir For Hepatitis C Virus Genotype 1 Infectiontruongduyhieu1311No ratings yet
- Randomized Clinical Trial of Antibiotic Therapy ForDocument5 pagesRandomized Clinical Trial of Antibiotic Therapy ForjimenacuadradoanguloNo ratings yet
- Zac 3843Document10 pagesZac 3843Juliän VillamizarNo ratings yet
- Predictors of Success With Highly Active Antiretroviral Therapy in An Antiretroviral-Naive Urban PopulationDocument6 pagesPredictors of Success With Highly Active Antiretroviral Therapy in An Antiretroviral-Naive Urban PopulationMuhammad Hafidzul HairulNo ratings yet
- Atorvastatin Improves Sputum Conversion and Chest X-Ray Severity ScoreDocument6 pagesAtorvastatin Improves Sputum Conversion and Chest X-Ray Severity Scorecharmainemargaret.parreno.medNo ratings yet
- HAI Guidelines 2010Document21 pagesHAI Guidelines 2010Mario Suarez MontalvoNo ratings yet
- Prevalence of Mutations Conferring Resistance Among Multi-And Extensively Drug-Resistant Mycobacterium Tuberculosis Isolates in ChinaDocument4 pagesPrevalence of Mutations Conferring Resistance Among Multi-And Extensively Drug-Resistant Mycobacterium Tuberculosis Isolates in ChinaKartikeya SinghNo ratings yet
- Revision de LesDocument12 pagesRevision de Lesroberto mendezNo ratings yet
- Tofacitinib As Induction and Maintenance Therapy For Ulcerative ColitisDocument14 pagesTofacitinib As Induction and Maintenance Therapy For Ulcerative Colitismichal ben meronNo ratings yet
- Oral Direct Acting Agent Therapy For Hepatitis C Virus Infection A Systematic ReviewDocument13 pagesOral Direct Acting Agent Therapy For Hepatitis C Virus Infection A Systematic ReviewRoberto López MataNo ratings yet
- RSV Vaccine Journal ClubDocument18 pagesRSV Vaccine Journal Clubapi-719803017100% (1)
- Krishna 26pDocument29 pagesKrishna 26pyanshutradelink.pvtNo ratings yet
- Brmedj00461 0017Document4 pagesBrmedj00461 0017muhammad24fayazNo ratings yet
- GastroparesisDocument4 pagesGastroparesisnadNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 5: GastrointestinalFrom EverandComplementary and Alternative Medical Lab Testing Part 5: GastrointestinalNo ratings yet
- Assessment and Management of Patients With Hepatic DisordersDocument3 pagesAssessment and Management of Patients With Hepatic DisordersaliNo ratings yet
- Acyanotic CHD-obstructiveDocument39 pagesAcyanotic CHD-obstructiveEbuka AniNo ratings yet
- Passmedicine MRCP Notes-Palliative Medicine and End of Life CareDocument5 pagesPassmedicine MRCP Notes-Palliative Medicine and End of Life CareMayar WaelNo ratings yet
- COVID-19: PandemicDocument39 pagesCOVID-19: PandemicGuillermo Rodriguez LopezNo ratings yet
- Exercise 1. Complete The Text Using The Words From The BoxDocument5 pagesExercise 1. Complete The Text Using The Words From The BoxВлада ВоеводинаNo ratings yet
- hs486 Document OSHA Recording Work-Related Injuries and IllnessesDocument13 pageshs486 Document OSHA Recording Work-Related Injuries and Illnessesfatmata koromaNo ratings yet
- Smoking Is DangerousDocument3 pagesSmoking Is DangerousAbdulmalkNo ratings yet
- Depressed People of The Bible Freedom From A Cave of Depression To The Light of Life (Jeff Zaremsky) (Z-Library)Document167 pagesDepressed People of The Bible Freedom From A Cave of Depression To The Light of Life (Jeff Zaremsky) (Z-Library)Isaac GisoreNo ratings yet
- Evd Evd Evd Evd Accudrain Accudrain Accudrain Accudrain: External Ventricular DeviceDocument1 pageEvd Evd Evd Evd Accudrain Accudrain Accudrain Accudrain: External Ventricular DeviceQueenNo ratings yet
- 7-5 (Nhóm 7)Document7 pages7-5 (Nhóm 7)Nguyễn Văn VượngNo ratings yet
- 17 ADD Type TestDocument7 pages17 ADD Type TestEvandro Pinho0% (1)
- The Complete Guide To Weight Loss and FitnessDocument4 pagesThe Complete Guide To Weight Loss and FitnessOnika BoteroNo ratings yet
- Tribute ofDocument10 pagesTribute ofAlvaro Andres Flores JimenezNo ratings yet
- English Conversation Discussion About AllergiesDocument3 pagesEnglish Conversation Discussion About AllergiesKevin ScottNo ratings yet
- TriageDocument37 pagesTriagekyuleen05No ratings yet
- Instant Download Ebook PDF Foundations of Nursing Enrolled Division 2 Nurses 1st Edition PDF ScribdDocument41 pagesInstant Download Ebook PDF Foundations of Nursing Enrolled Division 2 Nurses 1st Edition PDF Scribddanny.bradt610100% (48)
- ANA101 Respiratory System DR GIEDocument44 pagesANA101 Respiratory System DR GIEMarian Kyla MarianoNo ratings yet
- Scrotal Conditions: Done By: Enas Almazraway Sarah Al-HawamdehDocument65 pagesScrotal Conditions: Done By: Enas Almazraway Sarah Al-HawamdehMohammad GharaibehNo ratings yet
- LD Final PriyankaDocument108 pagesLD Final PriyankaPriyanka GandhiNo ratings yet
- Drug Induced Movement DisordersDocument65 pagesDrug Induced Movement DisordersShaunak Patil100% (1)
- Clin Transl Allergy (2019)Document7 pagesClin Transl Allergy (2019)Nimesh ModiNo ratings yet
- 1439019766-7. Nursing - Couvade Syndrome - Bency AbrahamDocument4 pages1439019766-7. Nursing - Couvade Syndrome - Bency AbrahamGeorgi GugicevNo ratings yet
- Daftar Pasien Neurologi RABU 22 APRIL 2020: Lontara 3 Saraf Kamar 1Document4 pagesDaftar Pasien Neurologi RABU 22 APRIL 2020: Lontara 3 Saraf Kamar 1Ilham Habib DjarkoniNo ratings yet
- The Marketing Experiment of Melody ToffeeDocument13 pagesThe Marketing Experiment of Melody ToffeeRishabh RajNo ratings yet
- 0 - Locally Endemic and Communicable Diseases-1Document10 pages0 - Locally Endemic and Communicable Diseases-1jonaNo ratings yet
- Group 3 Diabetes MellitusDocument9 pagesGroup 3 Diabetes MellitusMary0% (1)
- ĐỀ THI THỬ- TRƯỜNGDocument4 pagesĐỀ THI THỬ- TRƯỜNGAdiecenNo ratings yet
- Feyer 2020 WvngoshawkDocument13 pagesFeyer 2020 WvngoshawkAgnieszka CzujkowskaNo ratings yet