Download as pdf or txt
You might also like
- Grand Rounds Amdekar PDFDocument324 pagesGrand Rounds Amdekar PDFBhagyashree SawardekarNo ratings yet
- SNLE Applicant Guide 2020Document14 pagesSNLE Applicant Guide 2020Tati MaryatiNo ratings yet
- Department of Nursing Initial Competency Validation Checklist: Orientation: RNDocument4 pagesDepartment of Nursing Initial Competency Validation Checklist: Orientation: RNAmeng GosimNo ratings yet
- FANCAS AssessmentDocument19 pagesFANCAS AssessmentNelly Q. NisaNo ratings yet
- Certificate and Duties and ResponsibilitiesDocument2 pagesCertificate and Duties and ResponsibilitiesShiredan Rose BagarinaoNo ratings yet
- Restraint CompetencyDocument6 pagesRestraint CompetencyFrederick RyanNo ratings yet
- Preceptor EvaluationDocument2 pagesPreceptor Evaluationapi-380898658No ratings yet
- Beyond The Breech Trial. Maggie BanksDocument4 pagesBeyond The Breech Trial. Maggie Bankspurpleanvil100% (2)
- Gall Bladder Cleanse Process Based On Andreas Moritz Book - Prof Prabhat Ranjan's BlogDocument8 pagesGall Bladder Cleanse Process Based On Andreas Moritz Book - Prof Prabhat Ranjan's Blogashukla_rgipt67% (3)
- The COAT & Review Approach: How to recognise and manage unwell patientsFrom EverandThe COAT & Review Approach: How to recognise and manage unwell patientsRating: 5 out of 5 stars5/5 (1)
- Textbook of Urgent Care Management: Chapter 34, Engaging Accountable Care Organizations in Urgent Care CentersFrom EverandTextbook of Urgent Care Management: Chapter 34, Engaging Accountable Care Organizations in Urgent Care CentersNo ratings yet
- 2023 OB/GYN Coding Manual: Components of Correct CodingFrom Everand2023 OB/GYN Coding Manual: Components of Correct CodingNo ratings yet
- Early EmergencyDocument53 pagesEarly EmergencyDwi ayu oktaveni100% (1)
- Trauma NurseDocument11 pagesTrauma Nurseapi-247119922No ratings yet
- ENA Leadership Conference 2013 ProgramDocument17 pagesENA Leadership Conference 2013 ProgramEmergency Nurses AssociationNo ratings yet
- Early Warning Score & Rapid Response TeamDocument26 pagesEarly Warning Score & Rapid Response TeamAsim IdreesNo ratings yet
- Nurs 6900 Syllabus Summer 22 1Document8 pagesNurs 6900 Syllabus Summer 22 1api-635690065No ratings yet
- Initial Assessment and ManagementDocument8 pagesInitial Assessment and ManagementAlvin De LunaNo ratings yet
- Rapid Response Team WorksheetDocument1 pageRapid Response Team Worksheetapi-403028741No ratings yet
- Emergency Trauma CareDocument49 pagesEmergency Trauma Careandrei neagNo ratings yet
- TransitionDocument13 pagesTransitionDonna NituraNo ratings yet
- Necrotizing Otitis 2022Document20 pagesNecrotizing Otitis 2022asmashNo ratings yet
- W1L1 - Initial Assessment For Trauma - 2Document44 pagesW1L1 - Initial Assessment For Trauma - 2Baihaqi SaharunNo ratings yet
- Nursing in EmergenciesDocument5 pagesNursing in EmergenciesAvisheel KalsiNo ratings yet
- Medical-Surgical Nursing Review Flashcards - QuizletDocument14 pagesMedical-Surgical Nursing Review Flashcards - QuizletNursyNurse100% (1)
- Bedside BrochureDocument2 pagesBedside Brochureapi-438607141100% (1)
- Nsg241 Study Guide Exam 5Document76 pagesNsg241 Study Guide Exam 5NatalieAndersonNo ratings yet
- Rapid Sequence Intubation: BackgroundDocument8 pagesRapid Sequence Intubation: Backgroundmarsh86No ratings yet
- Emergency Nursing: Roles of Emergency NurseDocument6 pagesEmergency Nursing: Roles of Emergency NursejorgeacctNo ratings yet
- CEN Guide 4: Guide For The Inclusion of Environmental Aspects in Product StandardsDocument18 pagesCEN Guide 4: Guide For The Inclusion of Environmental Aspects in Product StandardsLauren GarciaNo ratings yet
- Interdisciplinary Nursing DocumentationDocument6 pagesInterdisciplinary Nursing Documentationgrace_nakateNo ratings yet
- National Clinical Guideline No. 5 Clinical Handover Nov2014Document306 pagesNational Clinical Guideline No. 5 Clinical Handover Nov2014Ahmad JuliadiNo ratings yet
- Normal Ranges Vital Signs 2017Document2 pagesNormal Ranges Vital Signs 2017Elvis Nguyen100% (1)
- Stroke Clinical PathwayDocument1 pageStroke Clinical PathwayKanoknun PisitpatcaragulNo ratings yet
- Trauma Nursing Core Course: Preparation PacketDocument13 pagesTrauma Nursing Core Course: Preparation PacketJimmy NaglesNo ratings yet
- Assessment and Re-Assessment of Patients According To The Scope of ServiceDocument9 pagesAssessment and Re-Assessment of Patients According To The Scope of Servicegiya nursingNo ratings yet
- Ebook PDF Nursing Diagnosis Manual Planning Individualizing and Documenting Client Care 6th EditionDocument35 pagesEbook PDF Nursing Diagnosis Manual Planning Individualizing and Documenting Client Care 6th Editionbarbara.slagle967No ratings yet
- Evidence Based Emergency Care PDFDocument2 pagesEvidence Based Emergency Care PDFMelissa0% (1)
- Assessment of An ICU PatientDocument71 pagesAssessment of An ICU PatientTito Tesfaye100% (1)
- Cardiovascular CareDocument4 pagesCardiovascular Carenoble786No ratings yet
- Access To Care and Continuity of CareDocument44 pagesAccess To Care and Continuity of CareCamille Honeyleith Lanuza FernandoNo ratings yet
- Trauma Assessment: Aims of The Initial Evaluation of Trauma PatientsDocument6 pagesTrauma Assessment: Aims of The Initial Evaluation of Trauma Patientsece142No ratings yet
- Push 3Document2 pagesPush 3Sandeep SharmaNo ratings yet
- Simulation Acute Coronary Syndrome (Learner)Document2 pagesSimulation Acute Coronary Syndrome (Learner)Wanda Nowell0% (1)
- Triage NurseDocument1 pageTriage NurseJeyser T. GamutiaNo ratings yet
- Hourly Round ProjectDocument8 pagesHourly Round ProjectaustinisaacNo ratings yet
- Revisions To The Canadian Emergency Department Triage and Acuity Scale Implementation GuidelinesDocument8 pagesRevisions To The Canadian Emergency Department Triage and Acuity Scale Implementation GuidelinesTiti Multi SaariNo ratings yet
- Short Term Training Curriculum Handbook - EMT-B - 1 June 2017 - 1Document48 pagesShort Term Training Curriculum Handbook - EMT-B - 1 June 2017 - 1navneetNo ratings yet
- 15Document21 pages15Tyson Easo JonesNo ratings yet
- BLS Study Guide 020620013Document38 pagesBLS Study Guide 020620013R RatheeshNo ratings yet
- Internship LogbookDocument9 pagesInternship Logbooksarhang talebaniNo ratings yet
- Pre Hos TraumaDocument11 pagesPre Hos TraumaGel OmugtongNo ratings yet
- Clinical Nursing JudgementDocument6 pagesClinical Nursing Judgementapi-508132058No ratings yet
- Periop Power PointDocument97 pagesPeriop Power PointAldrine Albor Anyayahan INo ratings yet
- Admission To ICUDocument4 pagesAdmission To ICUSapiah RamanNo ratings yet
- Malignant Hyperthermia Fact SheetDocument2 pagesMalignant Hyperthermia Fact Sheetapi-301819201No ratings yet
- Harley L. Dela Cruz, RN LecturerDocument110 pagesHarley L. Dela Cruz, RN LecturerHarley Justiniani Dela CruzNo ratings yet
- Canadian Triage and Acuity Scale PediaDocument30 pagesCanadian Triage and Acuity Scale PediaPrince Jhessie L. AbellaNo ratings yet
- Clinical ExemplarDocument5 pagesClinical Exemplarapi-605270704No ratings yet
- Notes For Perioperative NursingDocument5 pagesNotes For Perioperative NursingNey JuneNo ratings yet
- Primary Trauma CareDocument48 pagesPrimary Trauma CareKABERA RENENo ratings yet
- Case StudyPainDocument1 pageCase StudyPainlovesalad100% (1)
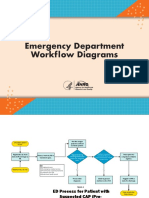
- Emergency Department Workflow DiagramsDocument5 pagesEmergency Department Workflow DiagramsMarwa El SayedNo ratings yet
- Reducing Waiting Time at An Emergency Department Using Design For Six Sigma and Discrete Event SimulationDocument15 pagesReducing Waiting Time at An Emergency Department Using Design For Six Sigma and Discrete Event SimulationMarwa El SayedNo ratings yet
- Nyu Winthrop Hospital: Patient Flow Data and Joint Commission ComplianceDocument5 pagesNyu Winthrop Hospital: Patient Flow Data and Joint Commission ComplianceMarwa El SayedNo ratings yet
- EDPerformanceMeasures ConsensusStatementDocument10 pagesEDPerformanceMeasures ConsensusStatementMarwa El SayedNo ratings yet
- PromoCellKatalog2013 LowresDocument212 pagesPromoCellKatalog2013 LowresmohdkhairNo ratings yet
- Acid Base BalanceDocument13 pagesAcid Base BalanceRashed ShatnawiNo ratings yet
- SANCON 2013 Programme ScheduleDocument2 pagesSANCON 2013 Programme ScheduleNafeesa AlamNo ratings yet
- Carti Electronice OfflineDocument33 pagesCarti Electronice OfflineCorinaNo ratings yet
- Homeopathy For Sports and Exercise InjuriesDocument4 pagesHomeopathy For Sports and Exercise Injurieskaravi schiniasNo ratings yet
- Penuntun Praktikum Mikrobiologi Tractus UrinariusDocument52 pagesPenuntun Praktikum Mikrobiologi Tractus UrinariusRiyan WirawanNo ratings yet
- Health Check-Up BriefDocument5 pagesHealth Check-Up Briefજીસીએસ હોસ્પિટલNo ratings yet
- Rubylyn's ResumeDocument6 pagesRubylyn's ResumeRÜbzz AlamanNo ratings yet
- Brief History of Barangay Centro EastDocument11 pagesBrief History of Barangay Centro EastIrene Soriano BayubayNo ratings yet
- EpiphoraDocument17 pagesEpiphoraDhivya SekarNo ratings yet
- Esophageal Atresia: Elvita Rahmi DaulayDocument21 pagesEsophageal Atresia: Elvita Rahmi DaulayabdullahshiddiqadamNo ratings yet
- Characteristics of Memories For Near-Death Experiences Lauren E. Moore, Bruce GreysonDocument10 pagesCharacteristics of Memories For Near-Death Experiences Lauren E. Moore, Bruce GreysonJuanMaNo ratings yet
- Nama: Yoga Eka Prasetyo NIM: 16105 Mata Kuliah: Bahasa Inggris 2 Tugas: Make A SentenceDocument10 pagesNama: Yoga Eka Prasetyo NIM: 16105 Mata Kuliah: Bahasa Inggris 2 Tugas: Make A SentenceYoga EkaNo ratings yet
- ENG - Advertisement Body Language Journal December 67 - S.A.F.E.R.®/NeoGraft® Hair Transplant TechniqueDocument3 pagesENG - Advertisement Body Language Journal December 67 - S.A.F.E.R.®/NeoGraft® Hair Transplant TechniqueMedicamatNo ratings yet
- Tepid Sponge BathDocument11 pagesTepid Sponge BathArva Glazel Defensor Gallofin100% (1)
- Catalog Kami SurgicalDocument430 pagesCatalog Kami SurgicalsavinNo ratings yet
- Quality Manual - 2022Document150 pagesQuality Manual - 2022CATHERINE MARIE TADIQUENo ratings yet
- Region X Cogon National High SchoolDocument2 pagesRegion X Cogon National High SchoolmusicaBGNo ratings yet
- Allergic Contact Dermatitis Caused by Titanium Screws and Dental ImplantsDocument7 pagesAllergic Contact Dermatitis Caused by Titanium Screws and Dental ImplantsAlexandra LauraNo ratings yet
- شريحه 1 مصطلحات طبيةDocument37 pagesشريحه 1 مصطلحات طبيةMohamed WahidNo ratings yet
- Physical Assessment CataractDocument12 pagesPhysical Assessment CataractEries Lacanlale LumbaNo ratings yet
- Transesophageal EchocardiogramDocument3 pagesTransesophageal EchocardiogramsiddharthaNo ratings yet
- Acute GastroenteritisDocument48 pagesAcute GastroenteritisAbel QuisquisNo ratings yet
- Cast, Brace, Traction CompilationDocument13 pagesCast, Brace, Traction CompilationMar Ordanza100% (1)
- Professional Therapies, Inc.: Vestibular Rehabilitation Therapy (VRT)Document4 pagesProfessional Therapies, Inc.: Vestibular Rehabilitation Therapy (VRT)blemmonptorNo ratings yet
- 688 1732 441841 82357 3 1 PDFDocument144 pages688 1732 441841 82357 3 1 PDFNuraisaNo ratings yet
- Maurice Nicoll - Dream PsychologyDocument204 pagesMaurice Nicoll - Dream PsychologyInderMatharuNo ratings yet