
9 Attending Physician's Statement (Death Claim)
9 Attending Physician's Statement (Death Claim)
You might also like
- KIZEN - Infinite Off SeasonDocument13 pagesKIZEN - Infinite Off SeasonLeon50% (4)
- Drug-Induced Diseases PDFDocument1,135 pagesDrug-Induced Diseases PDFGiang Vớ Vẩn100% (1)
- Etiqa-Attending Physician's StatementDocument2 pagesEtiqa-Attending Physician's StatementJohn AraojoNo ratings yet
- LIC Claim Form B 3784 Medical Attendant's CertificateDocument3 pagesLIC Claim Form B 3784 Medical Attendant's Certificategdbdgbd xc v xvNo ratings yet
- Death Claim Form: CLAIMFORM DC-aps Nov2016 v2 Page 1 of 2Document5 pagesDeath Claim Form: CLAIMFORM DC-aps Nov2016 v2 Page 1 of 2Lisa MendilloNo ratings yet
- Death Claim Checklist 2017Document4 pagesDeath Claim Checklist 2017Cheche GonzalesNo ratings yet
- Kenyataan Pegawai Perubatan (Kematian) : Attending Physician Statement (Death)Document2 pagesKenyataan Pegawai Perubatan (Kematian) : Attending Physician Statement (Death)Rosli Bin HussainNo ratings yet
- Attending - Physician's - Statement - Form Death ClaimDocument4 pagesAttending - Physician's - Statement - Form Death ClaimrogeliolacsamanaNo ratings yet
- Certificate of Hospital TreatmentDocument2 pagesCertificate of Hospital TreatmentRohit KumarNo ratings yet
- Forrm 4aDocument4 pagesForrm 4aJ.L. Jumbo XeroxNo ratings yet
- QUIZ 1 - Intro QUIZ 2 - DeathDocument6 pagesQUIZ 1 - Intro QUIZ 2 - DeathmemelandNo ratings yet
- Form Claim Request Life Insurance Declaration Physician 13386 512Document2 pagesForm Claim Request Life Insurance Declaration Physician 13386 512ashlstpiNo ratings yet
- Attending Physicians Statement Crisis Cover Muscular Dystrophy - 041222Document2 pagesAttending Physicians Statement Crisis Cover Muscular Dystrophy - 041222laraNo ratings yet
- Attending Physicians Statement Death Claim - 041222Document2 pagesAttending Physicians Statement Death Claim - 041222Lhen TrinidadNo ratings yet
- Personal Accident Critical Illness Hospital Income Claim FormDocument3 pagesPersonal Accident Critical Illness Hospital Income Claim FormHihiNo ratings yet
- Docs To Be SubmittedDocument15 pagesDocs To Be Submittedgourkanti213No ratings yet
- Declaration FormDocument1 pageDeclaration FormJzelNo ratings yet
- Hospital Benefit Claim FormDocument7 pagesHospital Benefit Claim FormEmmanuel MichaelNo ratings yet
- Proposal of APGLI ProformaDocument5 pagesProposal of APGLI ProformaVenkataSubrahmanyamVennelakantiNo ratings yet
- St. Peter Life Plan, Inc: (State Relationship To Deceased)Document1 pageSt. Peter Life Plan, Inc: (State Relationship To Deceased)Janice SobejanoNo ratings yet
- Death Claim Doctor'S Statement: Symptoms Presented at First Consultation Date Symptoms First Started (DD/MM/YY)Document2 pagesDeath Claim Doctor'S Statement: Symptoms Presented at First Consultation Date Symptoms First Started (DD/MM/YY)onlineNo ratings yet
- Cocolife Insurance Claim 2022Document5 pagesCocolife Insurance Claim 2022Shazar CarloNo ratings yet
- SHCS.01.16 : Relating To The Person InsuredDocument3 pagesSHCS.01.16 : Relating To The Person InsuredkathreentracyNo ratings yet
- Affidavit of Vaccine Adverse EffectDocument4 pagesAffidavit of Vaccine Adverse EffectRichard BalaisNo ratings yet
- Medical Examiner'S Confidential ReportDocument2 pagesMedical Examiner'S Confidential ReportParesh BorboruahNo ratings yet
- D ReportDocument2 pagesD ReportHihiNo ratings yet
- Attending Physician's Statement (Death Claim) : 1. General InformationDocument1 pageAttending Physician's Statement (Death Claim) : 1. General InformationPenielle SaguindanNo ratings yet
- IX InsuDocument19 pagesIX InsunikkimaxinevaldezNo ratings yet
- Iiisla Benevolent Fund (Ibf) : Claim FormDocument2 pagesIiisla Benevolent Fund (Ibf) : Claim FormSachin PrajapatiNo ratings yet
- GPMRDocument5 pagesGPMRwisdom hameloNo ratings yet
- Health Certificate To Work in Confined SpaceDocument6 pagesHealth Certificate To Work in Confined SpacenmmarhelNo ratings yet
- Biedron v. Anonymous Physician 1 - 2018 Ind. App. LEXIS SJ AffidavitsDocument15 pagesBiedron v. Anonymous Physician 1 - 2018 Ind. App. LEXIS SJ AffidavitsCourt FanaticNo ratings yet
- Great Eastern Life - Confidential Medical Certificate (Stroke) - CLMLAMCSDocument2 pagesGreat Eastern Life - Confidential Medical Certificate (Stroke) - CLMLAMCSsimpoonNo ratings yet
- Care of Dying PatientDocument22 pagesCare of Dying PatientMANEESH MANINo ratings yet
- PDF ResizeDocument99 pagesPDF ResizeRiazNo ratings yet
- Andrea F. Demars v. The Equitable Life Assurance Society of The United States, 610 F.2d 55, 1st Cir. (1979)Document16 pagesAndrea F. Demars v. The Equitable Life Assurance Society of The United States, 610 F.2d 55, 1st Cir. (1979)Scribd Government DocsNo ratings yet
- Takaful Forms For BAHLDocument4 pagesTakaful Forms For BAHLfayazaliteewno fayazaliteewnoNo ratings yet
- Betarie Anum Almira - RMIK (A) - BIK Ringkasan Masuk Dan KeluarDocument1 pageBetarie Anum Almira - RMIK (A) - BIK Ringkasan Masuk Dan KeluarBetarie Anum Almira100% (1)
- 4n6-Anam & VeR-4printDocument20 pages4n6-Anam & VeR-4printnessNo ratings yet
- Unified - POLICIES AND GUIDELINES ON ISSUANCE OF CERTIFICATESDocument2 pagesUnified - POLICIES AND GUIDELINES ON ISSUANCE OF CERTIFICATESrv bombetaNo ratings yet
- 11874158590df Agada Vyavahara AyurvedaDocument34 pages11874158590df Agada Vyavahara Ayurvedariyasukumar574No ratings yet
- Batiquim vs. CADocument4 pagesBatiquim vs. CARICKY ALEGARBESNo ratings yet
- Doctors CertificateDocument2 pagesDoctors CertificateequalseriousNo ratings yet
- Cdin BDocument13 pagesCdin Bjrjklm1627No ratings yet
- Cashless FormDocument2 pagesCashless FormHitendra PatelNo ratings yet
- Great Eastern Life - Confidential Medical Certificate (Other Illnesses) - CLMLAMCODocument2 pagesGreat Eastern Life - Confidential Medical Certificate (Other Illnesses) - CLMLAMCOsimpoonNo ratings yet
- Dying DeclararationDocument8 pagesDying Declararationmani pariatNo ratings yet
- Injury Examination ReportDocument2 pagesInjury Examination ReportHD EFFECTSNo ratings yet
- Attending Physicians Statement Crisis Cover Major Organ Transplant - 041222Document2 pagesAttending Physicians Statement Crisis Cover Major Organ Transplant - 041222max leeNo ratings yet
- Medical Fitness PDFDocument5 pagesMedical Fitness PDFVenkateshwara ReddyNo ratings yet
- Claim Requirement - Attending Physician Report (APR)Document2 pagesClaim Requirement - Attending Physician Report (APR)kst.mpc091192No ratings yet
- Visum Et Revertum (Korban Hidup)Document20 pagesVisum Et Revertum (Korban Hidup)Rey AlwiwikhNo ratings yet
- Insurance Ombudsman: You Can Approach The Ombudsman With Complaint IfDocument4 pagesInsurance Ombudsman: You Can Approach The Ombudsman With Complaint IfArpit GuptaNo ratings yet
- Raksha New Pre-Authorization FormDocument1 pageRaksha New Pre-Authorization Formjigerpanchal0% (1)
- Respiratory Disorder Questionnaire: Application # Agent #Document1 pageRespiratory Disorder Questionnaire: Application # Agent #Ivory Ace PalacioNo ratings yet
- Agartala: High Court of TripuraDocument4 pagesAgartala: High Court of TripuraLawbuzz CornerNo ratings yet
- Post Mortem CertificateDocument4 pagesPost Mortem CertificatePRINCENo ratings yet
- Admed Statement of Attending Physician or SurgeonDocument2 pagesAdmed Statement of Attending Physician or Surgeonshemina armorerNo ratings yet
- Q and A Legal MedicineDocument10 pagesQ and A Legal MedicineQayes Al-QuqaNo ratings yet
- Pcso Mam Program Services and RequirementsDocument12 pagesPcso Mam Program Services and RequirementsJen UmlanoNo ratings yet
- 5 6212887793887085843 PDFDocument11 pages5 6212887793887085843 PDFeruditeNo ratings yet
- Aids to Forensic Medicine and ToxicologyFrom EverandAids to Forensic Medicine and ToxicologyNo ratings yet
- Variable Pay & Executive Compensation Submmitted BY Shweta Nayak SuchitraDocument63 pagesVariable Pay & Executive Compensation Submmitted BY Shweta Nayak SuchitrabsbhavaniNo ratings yet
- Gen 017 - Sas Lesson #4Document5 pagesGen 017 - Sas Lesson #4ABM - Villanueva, Jaimee Lyn C.No ratings yet
- JuvenilleDocument5 pagesJuvenilleelviemjmontemayorNo ratings yet
- Balsamic VinegarDocument4 pagesBalsamic Vinegarfaruzzi.ceciliaNo ratings yet
- Prayer Points Pregnancy Mothers 18.11.14Document3 pagesPrayer Points Pregnancy Mothers 18.11.14MosesSivakumar100% (2)
- Naphthenic Acid / Naphthenate Stabilized Emulsions and The Influence of Crude Oil ComponentsDocument1 pageNaphthenic Acid / Naphthenate Stabilized Emulsions and The Influence of Crude Oil ComponentsLuis Alberto ChirinosNo ratings yet
- Fresh and Simple PDFDocument3 pagesFresh and Simple PDFthivashnee padayacheeNo ratings yet
- Egypt Agribusiness Report - Q1 2021Document78 pagesEgypt Agribusiness Report - Q1 2021Mina GeorgeNo ratings yet
- Anxiety DisordersDocument10 pagesAnxiety DisordersAhmed AntarNo ratings yet
- 2-BP-3.5K-5K 220v ManualDocument42 pages2-BP-3.5K-5K 220v ManualEcosenseTechnologies GreenenergyNo ratings yet
- Orthopaedic Study Guide 2014Document126 pagesOrthopaedic Study Guide 2014Yip Kar Jun100% (1)
- Datasheet DD2603Document3 pagesDatasheet DD2603RONALD TERRAZASNo ratings yet
- Neuro SnellDocument10 pagesNeuro SnellDoodsDiagoNo ratings yet
- Zoology Mammals (Rabbit)Document3 pagesZoology Mammals (Rabbit)PerrieNo ratings yet
- Steril DiskDocument3 pagesSteril DisklukasjoNo ratings yet
- Sala Ta Orn Dam Bill of QuantitiesDocument38 pagesSala Ta Orn Dam Bill of QuantitiesSothearaThengNo ratings yet
- Nurse-Patient Interaction Process Recording: College of NursingDocument3 pagesNurse-Patient Interaction Process Recording: College of NursingBianx Flores DosdosNo ratings yet
- Timber GrowthDocument17 pagesTimber GrowthAbdul Sukur Kamsir100% (3)
- TirupathiDocument14 pagesTirupathiEkta Adlakha100% (1)
- The Hidden World That Feeds Us - The Living SoilDocument40 pagesThe Hidden World That Feeds Us - The Living SoilmrmiscNo ratings yet
- Yokogawa RAGN ManualDocument46 pagesYokogawa RAGN ManualJohn AdewaleNo ratings yet
- Epaper 20 October 2022Document22 pagesEpaper 20 October 2022Tauya DauramanziNo ratings yet
- Vibrant Yet Under-Resourced: The State of Lesbian, Bisexual, and Queer MovementsDocument44 pagesVibrant Yet Under-Resourced: The State of Lesbian, Bisexual, and Queer MovementsSeres KozmicNo ratings yet
- The Food Chain Consists of Four Main PartsDocument3 pagesThe Food Chain Consists of Four Main PartskoiaitraazNo ratings yet
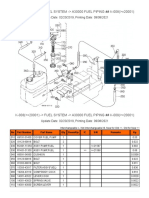
- K-008 ( 20001) - Fuel System - A30000 Fuel Piping ## K-008 ( 20001)Document2 pagesK-008 ( 20001) - Fuel System - A30000 Fuel Piping ## K-008 ( 20001)Martin LindbergNo ratings yet
- Definition of Terms Mine SurveyingDocument2 pagesDefinition of Terms Mine Surveyingaquariuspj25100% (3)
- Acquaintance Games: Morning Games Team Building Activity: The Boat Is SinkingDocument3 pagesAcquaintance Games: Morning Games Team Building Activity: The Boat Is SinkingAnonymous iZJv305rNo ratings yet
- 2.0 17-02-IM-f (Installation Manual)Document90 pages2.0 17-02-IM-f (Installation Manual)ARMANDOROSAS100% (1)





















































































Download as pdf or txt
You might also like
- KIZEN - Infinite Off SeasonDocument13 pagesKIZEN - Infinite Off SeasonLeon50% (4)
- Drug-Induced Diseases PDFDocument1,135 pagesDrug-Induced Diseases PDFGiang Vớ Vẩn100% (1)
- Etiqa-Attending Physician's StatementDocument2 pagesEtiqa-Attending Physician's StatementJohn AraojoNo ratings yet
- LIC Claim Form B 3784 Medical Attendant's CertificateDocument3 pagesLIC Claim Form B 3784 Medical Attendant's Certificategdbdgbd xc v xvNo ratings yet
- Death Claim Form: CLAIMFORM DC-aps Nov2016 v2 Page 1 of 2Document5 pagesDeath Claim Form: CLAIMFORM DC-aps Nov2016 v2 Page 1 of 2Lisa MendilloNo ratings yet
- Death Claim Checklist 2017Document4 pagesDeath Claim Checklist 2017Cheche GonzalesNo ratings yet
- Kenyataan Pegawai Perubatan (Kematian) : Attending Physician Statement (Death)Document2 pagesKenyataan Pegawai Perubatan (Kematian) : Attending Physician Statement (Death)Rosli Bin HussainNo ratings yet
- Attending - Physician's - Statement - Form Death ClaimDocument4 pagesAttending - Physician's - Statement - Form Death ClaimrogeliolacsamanaNo ratings yet
- Certificate of Hospital TreatmentDocument2 pagesCertificate of Hospital TreatmentRohit KumarNo ratings yet
- Forrm 4aDocument4 pagesForrm 4aJ.L. Jumbo XeroxNo ratings yet
- QUIZ 1 - Intro QUIZ 2 - DeathDocument6 pagesQUIZ 1 - Intro QUIZ 2 - DeathmemelandNo ratings yet
- Form Claim Request Life Insurance Declaration Physician 13386 512Document2 pagesForm Claim Request Life Insurance Declaration Physician 13386 512ashlstpiNo ratings yet
- Attending Physicians Statement Crisis Cover Muscular Dystrophy - 041222Document2 pagesAttending Physicians Statement Crisis Cover Muscular Dystrophy - 041222laraNo ratings yet
- Attending Physicians Statement Death Claim - 041222Document2 pagesAttending Physicians Statement Death Claim - 041222Lhen TrinidadNo ratings yet
- Personal Accident Critical Illness Hospital Income Claim FormDocument3 pagesPersonal Accident Critical Illness Hospital Income Claim FormHihiNo ratings yet
- Docs To Be SubmittedDocument15 pagesDocs To Be Submittedgourkanti213No ratings yet
- Declaration FormDocument1 pageDeclaration FormJzelNo ratings yet
- Hospital Benefit Claim FormDocument7 pagesHospital Benefit Claim FormEmmanuel MichaelNo ratings yet
- Proposal of APGLI ProformaDocument5 pagesProposal of APGLI ProformaVenkataSubrahmanyamVennelakantiNo ratings yet
- St. Peter Life Plan, Inc: (State Relationship To Deceased)Document1 pageSt. Peter Life Plan, Inc: (State Relationship To Deceased)Janice SobejanoNo ratings yet
- Death Claim Doctor'S Statement: Symptoms Presented at First Consultation Date Symptoms First Started (DD/MM/YY)Document2 pagesDeath Claim Doctor'S Statement: Symptoms Presented at First Consultation Date Symptoms First Started (DD/MM/YY)onlineNo ratings yet
- Cocolife Insurance Claim 2022Document5 pagesCocolife Insurance Claim 2022Shazar CarloNo ratings yet
- SHCS.01.16 : Relating To The Person InsuredDocument3 pagesSHCS.01.16 : Relating To The Person InsuredkathreentracyNo ratings yet
- Affidavit of Vaccine Adverse EffectDocument4 pagesAffidavit of Vaccine Adverse EffectRichard BalaisNo ratings yet
- Medical Examiner'S Confidential ReportDocument2 pagesMedical Examiner'S Confidential ReportParesh BorboruahNo ratings yet
- D ReportDocument2 pagesD ReportHihiNo ratings yet
- Attending Physician's Statement (Death Claim) : 1. General InformationDocument1 pageAttending Physician's Statement (Death Claim) : 1. General InformationPenielle SaguindanNo ratings yet
- IX InsuDocument19 pagesIX InsunikkimaxinevaldezNo ratings yet
- Iiisla Benevolent Fund (Ibf) : Claim FormDocument2 pagesIiisla Benevolent Fund (Ibf) : Claim FormSachin PrajapatiNo ratings yet
- GPMRDocument5 pagesGPMRwisdom hameloNo ratings yet
- Health Certificate To Work in Confined SpaceDocument6 pagesHealth Certificate To Work in Confined SpacenmmarhelNo ratings yet
- Biedron v. Anonymous Physician 1 - 2018 Ind. App. LEXIS SJ AffidavitsDocument15 pagesBiedron v. Anonymous Physician 1 - 2018 Ind. App. LEXIS SJ AffidavitsCourt FanaticNo ratings yet
- Great Eastern Life - Confidential Medical Certificate (Stroke) - CLMLAMCSDocument2 pagesGreat Eastern Life - Confidential Medical Certificate (Stroke) - CLMLAMCSsimpoonNo ratings yet
- Care of Dying PatientDocument22 pagesCare of Dying PatientMANEESH MANINo ratings yet
- PDF ResizeDocument99 pagesPDF ResizeRiazNo ratings yet
- Andrea F. Demars v. The Equitable Life Assurance Society of The United States, 610 F.2d 55, 1st Cir. (1979)Document16 pagesAndrea F. Demars v. The Equitable Life Assurance Society of The United States, 610 F.2d 55, 1st Cir. (1979)Scribd Government DocsNo ratings yet
- Takaful Forms For BAHLDocument4 pagesTakaful Forms For BAHLfayazaliteewno fayazaliteewnoNo ratings yet
- Betarie Anum Almira - RMIK (A) - BIK Ringkasan Masuk Dan KeluarDocument1 pageBetarie Anum Almira - RMIK (A) - BIK Ringkasan Masuk Dan KeluarBetarie Anum Almira100% (1)
- 4n6-Anam & VeR-4printDocument20 pages4n6-Anam & VeR-4printnessNo ratings yet
- Unified - POLICIES AND GUIDELINES ON ISSUANCE OF CERTIFICATESDocument2 pagesUnified - POLICIES AND GUIDELINES ON ISSUANCE OF CERTIFICATESrv bombetaNo ratings yet
- 11874158590df Agada Vyavahara AyurvedaDocument34 pages11874158590df Agada Vyavahara Ayurvedariyasukumar574No ratings yet
- Batiquim vs. CADocument4 pagesBatiquim vs. CARICKY ALEGARBESNo ratings yet
- Doctors CertificateDocument2 pagesDoctors CertificateequalseriousNo ratings yet
- Cdin BDocument13 pagesCdin Bjrjklm1627No ratings yet
- Cashless FormDocument2 pagesCashless FormHitendra PatelNo ratings yet
- Great Eastern Life - Confidential Medical Certificate (Other Illnesses) - CLMLAMCODocument2 pagesGreat Eastern Life - Confidential Medical Certificate (Other Illnesses) - CLMLAMCOsimpoonNo ratings yet
- Dying DeclararationDocument8 pagesDying Declararationmani pariatNo ratings yet
- Injury Examination ReportDocument2 pagesInjury Examination ReportHD EFFECTSNo ratings yet
- Attending Physicians Statement Crisis Cover Major Organ Transplant - 041222Document2 pagesAttending Physicians Statement Crisis Cover Major Organ Transplant - 041222max leeNo ratings yet
- Medical Fitness PDFDocument5 pagesMedical Fitness PDFVenkateshwara ReddyNo ratings yet
- Claim Requirement - Attending Physician Report (APR)Document2 pagesClaim Requirement - Attending Physician Report (APR)kst.mpc091192No ratings yet
- Visum Et Revertum (Korban Hidup)Document20 pagesVisum Et Revertum (Korban Hidup)Rey AlwiwikhNo ratings yet
- Insurance Ombudsman: You Can Approach The Ombudsman With Complaint IfDocument4 pagesInsurance Ombudsman: You Can Approach The Ombudsman With Complaint IfArpit GuptaNo ratings yet
- Raksha New Pre-Authorization FormDocument1 pageRaksha New Pre-Authorization Formjigerpanchal0% (1)
- Respiratory Disorder Questionnaire: Application # Agent #Document1 pageRespiratory Disorder Questionnaire: Application # Agent #Ivory Ace PalacioNo ratings yet
- Agartala: High Court of TripuraDocument4 pagesAgartala: High Court of TripuraLawbuzz CornerNo ratings yet
- Post Mortem CertificateDocument4 pagesPost Mortem CertificatePRINCENo ratings yet
- Admed Statement of Attending Physician or SurgeonDocument2 pagesAdmed Statement of Attending Physician or Surgeonshemina armorerNo ratings yet
- Q and A Legal MedicineDocument10 pagesQ and A Legal MedicineQayes Al-QuqaNo ratings yet
- Pcso Mam Program Services and RequirementsDocument12 pagesPcso Mam Program Services and RequirementsJen UmlanoNo ratings yet
- 5 6212887793887085843 PDFDocument11 pages5 6212887793887085843 PDFeruditeNo ratings yet
- Aids to Forensic Medicine and ToxicologyFrom EverandAids to Forensic Medicine and ToxicologyNo ratings yet
- Variable Pay & Executive Compensation Submmitted BY Shweta Nayak SuchitraDocument63 pagesVariable Pay & Executive Compensation Submmitted BY Shweta Nayak SuchitrabsbhavaniNo ratings yet
- Gen 017 - Sas Lesson #4Document5 pagesGen 017 - Sas Lesson #4ABM - Villanueva, Jaimee Lyn C.No ratings yet
- JuvenilleDocument5 pagesJuvenilleelviemjmontemayorNo ratings yet
- Balsamic VinegarDocument4 pagesBalsamic Vinegarfaruzzi.ceciliaNo ratings yet
- Prayer Points Pregnancy Mothers 18.11.14Document3 pagesPrayer Points Pregnancy Mothers 18.11.14MosesSivakumar100% (2)
- Naphthenic Acid / Naphthenate Stabilized Emulsions and The Influence of Crude Oil ComponentsDocument1 pageNaphthenic Acid / Naphthenate Stabilized Emulsions and The Influence of Crude Oil ComponentsLuis Alberto ChirinosNo ratings yet
- Fresh and Simple PDFDocument3 pagesFresh and Simple PDFthivashnee padayacheeNo ratings yet
- Egypt Agribusiness Report - Q1 2021Document78 pagesEgypt Agribusiness Report - Q1 2021Mina GeorgeNo ratings yet
- Anxiety DisordersDocument10 pagesAnxiety DisordersAhmed AntarNo ratings yet
- 2-BP-3.5K-5K 220v ManualDocument42 pages2-BP-3.5K-5K 220v ManualEcosenseTechnologies GreenenergyNo ratings yet
- Orthopaedic Study Guide 2014Document126 pagesOrthopaedic Study Guide 2014Yip Kar Jun100% (1)
- Datasheet DD2603Document3 pagesDatasheet DD2603RONALD TERRAZASNo ratings yet
- Neuro SnellDocument10 pagesNeuro SnellDoodsDiagoNo ratings yet
- Zoology Mammals (Rabbit)Document3 pagesZoology Mammals (Rabbit)PerrieNo ratings yet
- Steril DiskDocument3 pagesSteril DisklukasjoNo ratings yet
- Sala Ta Orn Dam Bill of QuantitiesDocument38 pagesSala Ta Orn Dam Bill of QuantitiesSothearaThengNo ratings yet
- Nurse-Patient Interaction Process Recording: College of NursingDocument3 pagesNurse-Patient Interaction Process Recording: College of NursingBianx Flores DosdosNo ratings yet
- Timber GrowthDocument17 pagesTimber GrowthAbdul Sukur Kamsir100% (3)
- TirupathiDocument14 pagesTirupathiEkta Adlakha100% (1)
- The Hidden World That Feeds Us - The Living SoilDocument40 pagesThe Hidden World That Feeds Us - The Living SoilmrmiscNo ratings yet
- Yokogawa RAGN ManualDocument46 pagesYokogawa RAGN ManualJohn AdewaleNo ratings yet
- Epaper 20 October 2022Document22 pagesEpaper 20 October 2022Tauya DauramanziNo ratings yet
- Vibrant Yet Under-Resourced: The State of Lesbian, Bisexual, and Queer MovementsDocument44 pagesVibrant Yet Under-Resourced: The State of Lesbian, Bisexual, and Queer MovementsSeres KozmicNo ratings yet
- The Food Chain Consists of Four Main PartsDocument3 pagesThe Food Chain Consists of Four Main PartskoiaitraazNo ratings yet
- K-008 ( 20001) - Fuel System - A30000 Fuel Piping ## K-008 ( 20001)Document2 pagesK-008 ( 20001) - Fuel System - A30000 Fuel Piping ## K-008 ( 20001)Martin LindbergNo ratings yet
- Definition of Terms Mine SurveyingDocument2 pagesDefinition of Terms Mine Surveyingaquariuspj25100% (3)
- Acquaintance Games: Morning Games Team Building Activity: The Boat Is SinkingDocument3 pagesAcquaintance Games: Morning Games Team Building Activity: The Boat Is SinkingAnonymous iZJv305rNo ratings yet
- 2.0 17-02-IM-f (Installation Manual)Document90 pages2.0 17-02-IM-f (Installation Manual)ARMANDOROSAS100% (1)