
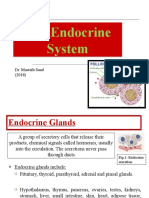
Endocrine Sys
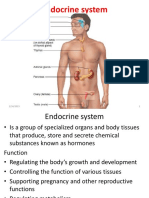
Endocrine Sys
You might also like
- Endocrine SystemDocument20 pagesEndocrine SystemSheena Pasion100% (2)
- The Endocrine SystemDocument14 pagesThe Endocrine SystemSairee AbianNo ratings yet
- Body System II 7 Endo 1Document27 pagesBody System II 7 Endo 1rrq8cwk2gnNo ratings yet
- Endocrine System (Finals)Document36 pagesEndocrine System (Finals)hjygcaingodNo ratings yet
- Chapter 2. Structure and Functions of Important Endocrine GlandsDocument17 pagesChapter 2. Structure and Functions of Important Endocrine GlandsAmit SharmaNo ratings yet
- Histology Lec-11 EndocrineDocument10 pagesHistology Lec-11 EndocrineKevin C. AguilarNo ratings yet
- Describe and Explained Organs Belong To Endocrine SystemDocument4 pagesDescribe and Explained Organs Belong To Endocrine SystemnilaahanifahNo ratings yet
- Endocrine GlandDocument14 pagesEndocrine Glandعلي عبدالله حسين سلمانNo ratings yet
- Pituitary Gland (Hypophysis)Document28 pagesPituitary Gland (Hypophysis)Nastase Daniela EcaterinaNo ratings yet
- 1st SCT Part 4Document63 pages1st SCT Part 4teeboyakegbesolaNo ratings yet
- Endocrine System Group 9Document77 pagesEndocrine System Group 9Jei SanNo ratings yet
- Endocrinal PathologyDocument81 pagesEndocrinal PathologyshehlaNo ratings yet
- Endo 1 2005Document53 pagesEndo 1 2005api-3698357No ratings yet
- A&P II Lab 1 Endocrine SystemDocument7 pagesA&P II Lab 1 Endocrine SystemWilliam DelphNo ratings yet
- Histology of Endocrine SystemMKDocument54 pagesHistology of Endocrine SystemMKDo Ra EmonNo ratings yet
- ENDODocument18 pagesENDOJoezer Gumangan VeranoNo ratings yet
- Physio RespiDocument17 pagesPhysio RespiJenica SorianoNo ratings yet
- Pituitary GlandDocument22 pagesPituitary GlandSara Musavi100% (2)
- Histology of Endocrine SystemMKDocument54 pagesHistology of Endocrine SystemMKDo Ra EmonNo ratings yet
- DR Zainuri Kuliahanatomi EndocrineDocument57 pagesDR Zainuri Kuliahanatomi EndocrinetomyhardiantoNo ratings yet
- Chemical Control and CoordinationDocument19 pagesChemical Control and CoordinationShubhamNo ratings yet
- Chap 3 Reproductive Hormones of Female AnimalsDocument80 pagesChap 3 Reproductive Hormones of Female Animalsyabsiradaniel930No ratings yet
- BiologyDocument21 pagesBiologynitesh.th15005No ratings yet
- Endocrine SystemDocument3 pagesEndocrine SystemFadhil Hussam AhmedNo ratings yet
- Pituitary Gland Anatomy: Embryologic DevelopmentDocument9 pagesPituitary Gland Anatomy: Embryologic DevelopmentRafaelPetitNo ratings yet
- Hypothalamus and PituitaryDocument13 pagesHypothalamus and PituitaryविपिनNo ratings yet
- Histology of Endocrine SystemDocument35 pagesHistology of Endocrine SystemX And ZNo ratings yet
- Muslimah D. Diangca - Activity 4Document4 pagesMuslimah D. Diangca - Activity 4Baby Corner MarawiNo ratings yet
- Note 30 Sep 2022Document96 pagesNote 30 Sep 2022ahmedagoz444No ratings yet
- Pouch and Will Develop Into The Anterior Pituitary orDocument130 pagesPouch and Will Develop Into The Anterior Pituitary orAnirudh AcharyaNo ratings yet
- 12 - Endocrine SystemDocument20 pages12 - Endocrine SystemNovie Roycell Fernandez RueloNo ratings yet
- Endocrine - HistoworldDocument12 pagesEndocrine - HistoworldKarl Torres Uganiza RmtNo ratings yet
- Endocrine SystemDocument25 pagesEndocrine SystemLits KhoNo ratings yet
- Endocrine Histology NotesDocument5 pagesEndocrine Histology NotesJulie TranNo ratings yet
- HISTOLOGY 4 - Endocrine SystemDocument9 pagesHISTOLOGY 4 - Endocrine SystemGauri SulekhaNo ratings yet
- Human Anatomy & Physiology: Autonomic Nervous SystemDocument8 pagesHuman Anatomy & Physiology: Autonomic Nervous SystemBeth EchavezNo ratings yet
- Hypothalamus, Pituitary, Thyroid & Parathyroid Glands-3Document70 pagesHypothalamus, Pituitary, Thyroid & Parathyroid Glands-3Benard NyaumaNo ratings yet
- Endocrine SystemDocument6 pagesEndocrine Systemrk749vbsk6No ratings yet
- HypothalamusDocument9 pagesHypothalamussnowNo ratings yet
- Endocrine System: Deference Between Hormone and EnzymeDocument9 pagesEndocrine System: Deference Between Hormone and EnzymeCurex QANo ratings yet
- Topic - Endocrine SystemDocument10 pagesTopic - Endocrine SystemAG05 Caperiña, Marcy Joy T.No ratings yet
- Introduction To EndocrinologyDocument15 pagesIntroduction To Endocrinologykazim786ahmedNo ratings yet
- Endocrine System - MedDocument124 pagesEndocrine System - Medrediet shimekachNo ratings yet
- The Endocrine SystemDocument37 pagesThe Endocrine SystemM Shafique SadiqeeNo ratings yet
- Histology of Endocrine GlandsDocument36 pagesHistology of Endocrine GlandsDaiva ŠiaulienėNo ratings yet
- Endocrine ResonanceDocument51 pagesEndocrine ResonanceEkta ManglaniNo ratings yet
- Hesto 1Document46 pagesHesto 1zsf8m52ky4No ratings yet
- Human Anatomy and Physiology - The Endocrine SystemDocument5 pagesHuman Anatomy and Physiology - The Endocrine SystemKraig Andre RellegueNo ratings yet
- The Endocrine SystemDocument101 pagesThe Endocrine SystemLeônidas ZazelisNo ratings yet
- Hypothlamic-Pituitary Physiology: Mona Abou Chebl MD. METABOLISM-2017 Lectures 1-2 March 20 2018Document197 pagesHypothlamic-Pituitary Physiology: Mona Abou Chebl MD. METABOLISM-2017 Lectures 1-2 March 20 2018rachid09No ratings yet
- (HISTOLOGY) Endocrine SystemDocument11 pages(HISTOLOGY) Endocrine Systemwipi112No ratings yet
- ANATOMY Endocrine TranscribedDocument9 pagesANATOMY Endocrine TranscribedYanyan PanesNo ratings yet
- Basic Human Anatomy: Lesson 10: Endocrine SystemDocument11 pagesBasic Human Anatomy: Lesson 10: Endocrine SystemIshita SinghNo ratings yet
- Lab Act 3 HistologyDocument15 pagesLab Act 3 HistologydiithandariNo ratings yet
- Role of Thalamus and HypothalamusDocument4 pagesRole of Thalamus and HypothalamusNishtha GuptaNo ratings yet
- EXCI360 Ch75 IntroductionDocument19 pagesEXCI360 Ch75 Introduction5xfz6hjkpgNo ratings yet
- EXCI360 Ch75 IntroductionDocument21 pagesEXCI360 Ch75 Introduction5xfz6hjkpgNo ratings yet
- 0405 Histo LectureDocument98 pages0405 Histo LectureJoe JNo ratings yet
- Endocrine System: Definition & BackgroundDocument11 pagesEndocrine System: Definition & Backgroundعبدالرحمن عدي عبدالفتاحNo ratings yet
- Endocrine System ReviewerDocument23 pagesEndocrine System ReviewerKimberly Joy GregorioNo ratings yet
- Deciphering nCoV19, Quest for Cure, Prophylaxis, and VaccineFrom EverandDeciphering nCoV19, Quest for Cure, Prophylaxis, and VaccineNo ratings yet
- Pituitary GlandDocument15 pagesPituitary GlandVincent Lau Bi ShengNo ratings yet
- Histology of Endocrine GlandsDocument36 pagesHistology of Endocrine GlandsDaiva ŠiaulienėNo ratings yet
- The Hypothalamus and Pituitary GlandDocument44 pagesThe Hypothalamus and Pituitary GlandRujha Haniena Ahmad RidzuanNo ratings yet
- HAP Practical PDFDocument44 pagesHAP Practical PDFVaishnavi SinghNo ratings yet
- Di and SiadhDocument15 pagesDi and SiadhSandra Martini SimmonsNo ratings yet
- Human Hypothalamus - Basic and Clinical Aspects, Part 2Document588 pagesHuman Hypothalamus - Basic and Clinical Aspects, Part 2Rodrigo Dumas DinizNo ratings yet
- The Endocrine Glands & Their HormonesDocument35 pagesThe Endocrine Glands & Their HormonesEtta Sagita Leonora100% (1)
- XII Zoology PC ReasoningDocument6 pagesXII Zoology PC ReasoningAmrah ShahNo ratings yet
- Science 10 A2.2 Pituitary and Hypothalamus The Bodys Control CentersDocument40 pagesScience 10 A2.2 Pituitary and Hypothalamus The Bodys Control CentersKhobie PabilicoNo ratings yet
- Endocrine Histology NotesDocument5 pagesEndocrine Histology NotesJulie TranNo ratings yet
- Chemical Coordination and IntegrationDocument17 pagesChemical Coordination and IntegrationHemant KumarNo ratings yet
- Endocrine System TransDocument21 pagesEndocrine System TransMa. Mil Adrianne PamaNo ratings yet
- Endocrine System Group 9Document77 pagesEndocrine System Group 9Jei SanNo ratings yet
- Sem 4 MCQ Week 4 Jan 2014 CTL McqsDocument15 pagesSem 4 MCQ Week 4 Jan 2014 CTL McqsFlowerNo ratings yet
- Endocrine System - MedDocument124 pagesEndocrine System - Medrediet shimekachNo ratings yet
- SGD Physiology Endocrine and MetabolismDocument7 pagesSGD Physiology Endocrine and MetabolismTinesh RajahNo ratings yet
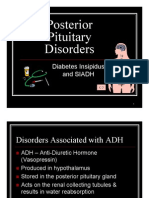
- Posterior Pituitary Disorder RomeoDocument19 pagesPosterior Pituitary Disorder RomeoSavin PetersNo ratings yet
- Coordination and Control (Ch#12) (1) .PDF FinalDocument19 pagesCoordination and Control (Ch#12) (1) .PDF FinalUmme AbdullahNo ratings yet
- EndocrineDocument144 pagesEndocrinedaffodilrachagNo ratings yet
- Module 1: The Endocrine System: Learning ObjectivesDocument1 pageModule 1: The Endocrine System: Learning ObjectivesZeina SharkasNo ratings yet
- Histology Finals ReviewerDocument14 pagesHistology Finals ReviewerRYABELLE JESUSA SANCHEZNo ratings yet
- Hypophysis CerebriDocument21 pagesHypophysis CerebriAli Akand AsifNo ratings yet
- Pituitary Gland Anatomy: Embryologic DevelopmentDocument9 pagesPituitary Gland Anatomy: Embryologic DevelopmentRafaelPetitNo ratings yet
- l8 Cc2 Lab Hypothalamus and Pituitary Gland Wala Nahuman PoDocument15 pagesl8 Cc2 Lab Hypothalamus and Pituitary Gland Wala Nahuman PoAlyanaNo ratings yet
- Histologi Organ EndokrinDocument32 pagesHistologi Organ EndokrinJasselia FeiNo ratings yet
- Posterior Pituitary Gland Presentation - paraDocument40 pagesPosterior Pituitary Gland Presentation - parahamidNo ratings yet
- CHEMICAL CONTROL & COORDINATION Question Bank Chapter Name MeghaDocument10 pagesCHEMICAL CONTROL & COORDINATION Question Bank Chapter Name Meghajayanthidungavath7032No ratings yet
- Endocrine System ReviewerDocument23 pagesEndocrine System ReviewerKimberly Joy GregorioNo ratings yet
- ParturitionDocument33 pagesParturitionNumbi HerizasiwiNo ratings yet
















































































Download as pdf or txt
You might also like
- Endocrine SystemDocument20 pagesEndocrine SystemSheena Pasion100% (2)
- The Endocrine SystemDocument14 pagesThe Endocrine SystemSairee AbianNo ratings yet
- Body System II 7 Endo 1Document27 pagesBody System II 7 Endo 1rrq8cwk2gnNo ratings yet
- Endocrine System (Finals)Document36 pagesEndocrine System (Finals)hjygcaingodNo ratings yet
- Chapter 2. Structure and Functions of Important Endocrine GlandsDocument17 pagesChapter 2. Structure and Functions of Important Endocrine GlandsAmit SharmaNo ratings yet
- Histology Lec-11 EndocrineDocument10 pagesHistology Lec-11 EndocrineKevin C. AguilarNo ratings yet
- Describe and Explained Organs Belong To Endocrine SystemDocument4 pagesDescribe and Explained Organs Belong To Endocrine SystemnilaahanifahNo ratings yet
- Endocrine GlandDocument14 pagesEndocrine Glandعلي عبدالله حسين سلمانNo ratings yet
- Pituitary Gland (Hypophysis)Document28 pagesPituitary Gland (Hypophysis)Nastase Daniela EcaterinaNo ratings yet
- 1st SCT Part 4Document63 pages1st SCT Part 4teeboyakegbesolaNo ratings yet
- Endocrine System Group 9Document77 pagesEndocrine System Group 9Jei SanNo ratings yet
- Endocrinal PathologyDocument81 pagesEndocrinal PathologyshehlaNo ratings yet
- Endo 1 2005Document53 pagesEndo 1 2005api-3698357No ratings yet
- A&P II Lab 1 Endocrine SystemDocument7 pagesA&P II Lab 1 Endocrine SystemWilliam DelphNo ratings yet
- Histology of Endocrine SystemMKDocument54 pagesHistology of Endocrine SystemMKDo Ra EmonNo ratings yet
- ENDODocument18 pagesENDOJoezer Gumangan VeranoNo ratings yet
- Physio RespiDocument17 pagesPhysio RespiJenica SorianoNo ratings yet
- Pituitary GlandDocument22 pagesPituitary GlandSara Musavi100% (2)
- Histology of Endocrine SystemMKDocument54 pagesHistology of Endocrine SystemMKDo Ra EmonNo ratings yet
- DR Zainuri Kuliahanatomi EndocrineDocument57 pagesDR Zainuri Kuliahanatomi EndocrinetomyhardiantoNo ratings yet
- Chemical Control and CoordinationDocument19 pagesChemical Control and CoordinationShubhamNo ratings yet
- Chap 3 Reproductive Hormones of Female AnimalsDocument80 pagesChap 3 Reproductive Hormones of Female Animalsyabsiradaniel930No ratings yet
- BiologyDocument21 pagesBiologynitesh.th15005No ratings yet
- Endocrine SystemDocument3 pagesEndocrine SystemFadhil Hussam AhmedNo ratings yet
- Pituitary Gland Anatomy: Embryologic DevelopmentDocument9 pagesPituitary Gland Anatomy: Embryologic DevelopmentRafaelPetitNo ratings yet
- Hypothalamus and PituitaryDocument13 pagesHypothalamus and PituitaryविपिनNo ratings yet
- Histology of Endocrine SystemDocument35 pagesHistology of Endocrine SystemX And ZNo ratings yet
- Muslimah D. Diangca - Activity 4Document4 pagesMuslimah D. Diangca - Activity 4Baby Corner MarawiNo ratings yet
- Note 30 Sep 2022Document96 pagesNote 30 Sep 2022ahmedagoz444No ratings yet
- Pouch and Will Develop Into The Anterior Pituitary orDocument130 pagesPouch and Will Develop Into The Anterior Pituitary orAnirudh AcharyaNo ratings yet
- 12 - Endocrine SystemDocument20 pages12 - Endocrine SystemNovie Roycell Fernandez RueloNo ratings yet
- Endocrine - HistoworldDocument12 pagesEndocrine - HistoworldKarl Torres Uganiza RmtNo ratings yet
- Endocrine SystemDocument25 pagesEndocrine SystemLits KhoNo ratings yet
- Endocrine Histology NotesDocument5 pagesEndocrine Histology NotesJulie TranNo ratings yet
- HISTOLOGY 4 - Endocrine SystemDocument9 pagesHISTOLOGY 4 - Endocrine SystemGauri SulekhaNo ratings yet
- Human Anatomy & Physiology: Autonomic Nervous SystemDocument8 pagesHuman Anatomy & Physiology: Autonomic Nervous SystemBeth EchavezNo ratings yet
- Hypothalamus, Pituitary, Thyroid & Parathyroid Glands-3Document70 pagesHypothalamus, Pituitary, Thyroid & Parathyroid Glands-3Benard NyaumaNo ratings yet
- Endocrine SystemDocument6 pagesEndocrine Systemrk749vbsk6No ratings yet
- HypothalamusDocument9 pagesHypothalamussnowNo ratings yet
- Endocrine System: Deference Between Hormone and EnzymeDocument9 pagesEndocrine System: Deference Between Hormone and EnzymeCurex QANo ratings yet
- Topic - Endocrine SystemDocument10 pagesTopic - Endocrine SystemAG05 Caperiña, Marcy Joy T.No ratings yet
- Introduction To EndocrinologyDocument15 pagesIntroduction To Endocrinologykazim786ahmedNo ratings yet
- Endocrine System - MedDocument124 pagesEndocrine System - Medrediet shimekachNo ratings yet
- The Endocrine SystemDocument37 pagesThe Endocrine SystemM Shafique SadiqeeNo ratings yet
- Histology of Endocrine GlandsDocument36 pagesHistology of Endocrine GlandsDaiva ŠiaulienėNo ratings yet
- Endocrine ResonanceDocument51 pagesEndocrine ResonanceEkta ManglaniNo ratings yet
- Hesto 1Document46 pagesHesto 1zsf8m52ky4No ratings yet
- Human Anatomy and Physiology - The Endocrine SystemDocument5 pagesHuman Anatomy and Physiology - The Endocrine SystemKraig Andre RellegueNo ratings yet
- The Endocrine SystemDocument101 pagesThe Endocrine SystemLeônidas ZazelisNo ratings yet
- Hypothlamic-Pituitary Physiology: Mona Abou Chebl MD. METABOLISM-2017 Lectures 1-2 March 20 2018Document197 pagesHypothlamic-Pituitary Physiology: Mona Abou Chebl MD. METABOLISM-2017 Lectures 1-2 March 20 2018rachid09No ratings yet
- (HISTOLOGY) Endocrine SystemDocument11 pages(HISTOLOGY) Endocrine Systemwipi112No ratings yet
- ANATOMY Endocrine TranscribedDocument9 pagesANATOMY Endocrine TranscribedYanyan PanesNo ratings yet
- Basic Human Anatomy: Lesson 10: Endocrine SystemDocument11 pagesBasic Human Anatomy: Lesson 10: Endocrine SystemIshita SinghNo ratings yet
- Lab Act 3 HistologyDocument15 pagesLab Act 3 HistologydiithandariNo ratings yet
- Role of Thalamus and HypothalamusDocument4 pagesRole of Thalamus and HypothalamusNishtha GuptaNo ratings yet
- EXCI360 Ch75 IntroductionDocument19 pagesEXCI360 Ch75 Introduction5xfz6hjkpgNo ratings yet
- EXCI360 Ch75 IntroductionDocument21 pagesEXCI360 Ch75 Introduction5xfz6hjkpgNo ratings yet
- 0405 Histo LectureDocument98 pages0405 Histo LectureJoe JNo ratings yet
- Endocrine System: Definition & BackgroundDocument11 pagesEndocrine System: Definition & Backgroundعبدالرحمن عدي عبدالفتاحNo ratings yet
- Endocrine System ReviewerDocument23 pagesEndocrine System ReviewerKimberly Joy GregorioNo ratings yet
- Deciphering nCoV19, Quest for Cure, Prophylaxis, and VaccineFrom EverandDeciphering nCoV19, Quest for Cure, Prophylaxis, and VaccineNo ratings yet
- Pituitary GlandDocument15 pagesPituitary GlandVincent Lau Bi ShengNo ratings yet
- Histology of Endocrine GlandsDocument36 pagesHistology of Endocrine GlandsDaiva ŠiaulienėNo ratings yet
- The Hypothalamus and Pituitary GlandDocument44 pagesThe Hypothalamus and Pituitary GlandRujha Haniena Ahmad RidzuanNo ratings yet
- HAP Practical PDFDocument44 pagesHAP Practical PDFVaishnavi SinghNo ratings yet
- Di and SiadhDocument15 pagesDi and SiadhSandra Martini SimmonsNo ratings yet
- Human Hypothalamus - Basic and Clinical Aspects, Part 2Document588 pagesHuman Hypothalamus - Basic and Clinical Aspects, Part 2Rodrigo Dumas DinizNo ratings yet
- The Endocrine Glands & Their HormonesDocument35 pagesThe Endocrine Glands & Their HormonesEtta Sagita Leonora100% (1)
- XII Zoology PC ReasoningDocument6 pagesXII Zoology PC ReasoningAmrah ShahNo ratings yet
- Science 10 A2.2 Pituitary and Hypothalamus The Bodys Control CentersDocument40 pagesScience 10 A2.2 Pituitary and Hypothalamus The Bodys Control CentersKhobie PabilicoNo ratings yet
- Endocrine Histology NotesDocument5 pagesEndocrine Histology NotesJulie TranNo ratings yet
- Chemical Coordination and IntegrationDocument17 pagesChemical Coordination and IntegrationHemant KumarNo ratings yet
- Endocrine System TransDocument21 pagesEndocrine System TransMa. Mil Adrianne PamaNo ratings yet
- Endocrine System Group 9Document77 pagesEndocrine System Group 9Jei SanNo ratings yet
- Sem 4 MCQ Week 4 Jan 2014 CTL McqsDocument15 pagesSem 4 MCQ Week 4 Jan 2014 CTL McqsFlowerNo ratings yet
- Endocrine System - MedDocument124 pagesEndocrine System - Medrediet shimekachNo ratings yet
- SGD Physiology Endocrine and MetabolismDocument7 pagesSGD Physiology Endocrine and MetabolismTinesh RajahNo ratings yet
- Posterior Pituitary Disorder RomeoDocument19 pagesPosterior Pituitary Disorder RomeoSavin PetersNo ratings yet
- Coordination and Control (Ch#12) (1) .PDF FinalDocument19 pagesCoordination and Control (Ch#12) (1) .PDF FinalUmme AbdullahNo ratings yet
- EndocrineDocument144 pagesEndocrinedaffodilrachagNo ratings yet
- Module 1: The Endocrine System: Learning ObjectivesDocument1 pageModule 1: The Endocrine System: Learning ObjectivesZeina SharkasNo ratings yet
- Histology Finals ReviewerDocument14 pagesHistology Finals ReviewerRYABELLE JESUSA SANCHEZNo ratings yet
- Hypophysis CerebriDocument21 pagesHypophysis CerebriAli Akand AsifNo ratings yet
- Pituitary Gland Anatomy: Embryologic DevelopmentDocument9 pagesPituitary Gland Anatomy: Embryologic DevelopmentRafaelPetitNo ratings yet
- l8 Cc2 Lab Hypothalamus and Pituitary Gland Wala Nahuman PoDocument15 pagesl8 Cc2 Lab Hypothalamus and Pituitary Gland Wala Nahuman PoAlyanaNo ratings yet
- Histologi Organ EndokrinDocument32 pagesHistologi Organ EndokrinJasselia FeiNo ratings yet
- Posterior Pituitary Gland Presentation - paraDocument40 pagesPosterior Pituitary Gland Presentation - parahamidNo ratings yet
- CHEMICAL CONTROL & COORDINATION Question Bank Chapter Name MeghaDocument10 pagesCHEMICAL CONTROL & COORDINATION Question Bank Chapter Name Meghajayanthidungavath7032No ratings yet
- Endocrine System ReviewerDocument23 pagesEndocrine System ReviewerKimberly Joy GregorioNo ratings yet
- ParturitionDocument33 pagesParturitionNumbi HerizasiwiNo ratings yet