Download as pdf or txt
You might also like
- TLDR Anticoag Cheat Sheet v1.1Document3 pagesTLDR Anticoag Cheat Sheet v1.1nitishavenkat100% (9)
- Medication: Expected Pharmacological Action Therapeutic UseDocument1 pageMedication: Expected Pharmacological Action Therapeutic UseMarina Wasem NetzlaffNo ratings yet
- Daftar Tarif Klinik Utama BPRC (Benar) RevDocument3 pagesDaftar Tarif Klinik Utama BPRC (Benar) RevYulvinna BirahmatikaNo ratings yet
- ONE Compartment Open ModelDocument29 pagesONE Compartment Open ModelNOORUDDINNo ratings yet
- Chapter 3. One-Compartment Open Model Intravenous Bolus AdministrationDocument23 pagesChapter 3. One-Compartment Open Model Intravenous Bolus AdministrationbencleeseNo ratings yet
- Psychopharmacology LectureDocument29 pagesPsychopharmacology LectureTarek Qawasmeh100% (3)
- Pharmacokinetics Explained ClearlyDocument59 pagesPharmacokinetics Explained Clearlyirrelevant100% (1)
- Clin PK 1-4Document105 pagesClin PK 1-4Klye SahagunNo ratings yet
- Chapter 11 Multiple Dosage RegimenDocument35 pagesChapter 11 Multiple Dosage RegimenYuli Irvaransiah DIatun NIkmah100% (2)
- Pharamcokinetics: Course In-Charge: Nimra Waheed Course Name: Biopharmaceutics and Pharmacokinetics Course Code: 613-TDocument21 pagesPharamcokinetics: Course In-Charge: Nimra Waheed Course Name: Biopharmaceutics and Pharmacokinetics Course Code: 613-TNeha GulfamNo ratings yet
- Introduction To BiopharmaceuticsDocument34 pagesIntroduction To BiopharmaceuticsMd. Yasir Galib 1721609649100% (1)
- Nonlinear Pharmacokinetics 1Document34 pagesNonlinear Pharmacokinetics 1donndisaster100% (1)
- Clinical PharmacokineticsDocument31 pagesClinical PharmacokineticsArdiyanti Puspitasari100% (2)
- 1important DefinitionsDocument3 pages1important DefinitionsBest VideoNo ratings yet
- Chapter 7. Pharmacokinetics of Oral AbsorptionDocument28 pagesChapter 7. Pharmacokinetics of Oral AbsorptionbencleeseNo ratings yet
- Factors Influencing Drug Absorption Though Git PDFDocument59 pagesFactors Influencing Drug Absorption Though Git PDFRamakant JoshiNo ratings yet
- A Basic Overview On Transdermal Drug Delivery SystemDocument9 pagesA Basic Overview On Transdermal Drug Delivery SystemEditor IJTSRDNo ratings yet
- Application of PK in Clinical SitutionDocument42 pagesApplication of PK in Clinical Situtionsafia mehmood100% (1)
- Introduction To PharmacologyDocument28 pagesIntroduction To Pharmacologynadar shahNo ratings yet
- Drug Absorption and DistributionDocument30 pagesDrug Absorption and DistributionaelmowafyNo ratings yet
- Compartment ModellingDocument46 pagesCompartment ModellingBio DataNo ratings yet
- Controlled Drug Delivery Systems - 1 PDFDocument6 pagesControlled Drug Delivery Systems - 1 PDFVikash Kushwaha100% (1)
- Prof Henny Lucida PHD Apt Calculation of DosespptDocument27 pagesProf Henny Lucida PHD Apt Calculation of DosespptWella CitraersyaNo ratings yet
- Oral Controlled Release Drug Delivery SystemDocument59 pagesOral Controlled Release Drug Delivery SystemYanulia HandayaniNo ratings yet
- Important Questions BPPK 3rd Year 2nd SemDocument3 pagesImportant Questions BPPK 3rd Year 2nd Semsupraja.bommala100% (1)
- Implantable Drug Delivery SystemDocument25 pagesImplantable Drug Delivery SystemsrikanthgaliNo ratings yet
- Miscellaneous Determination & Tests: By: Dr. Shumaila ShafiqueDocument28 pagesMiscellaneous Determination & Tests: By: Dr. Shumaila ShafiqueShoaib Muhammad100% (1)
- Dr. Ruth NamyaloDocument62 pagesDr. Ruth NamyaloHarun MohamedNo ratings yet
- Laboratory Manual of Biopharmaceutics and Pharmacokinetics PDFDocument168 pagesLaboratory Manual of Biopharmaceutics and Pharmacokinetics PDFNiraj GuptaNo ratings yet
- Compartmental ModelDocument5 pagesCompartmental ModelIlyax KahnNo ratings yet
- Pharmaceutics Chapter 7 Novel Drug Delivery System NotesDocument10 pagesPharmaceutics Chapter 7 Novel Drug Delivery System NotesBhuvnesh ChandraNo ratings yet
- Practice ProblemsDocument2 pagesPractice ProblemsShemaj GurchumaNo ratings yet
- Principles of Pharmacology Chapter 1Document37 pagesPrinciples of Pharmacology Chapter 1Muhammad ZakriaNo ratings yet
- 2.one Compartment Open ModelDocument90 pages2.one Compartment Open ModelBLESSY SARA KURIANNo ratings yet
- Controlled Release Oral Drug Delivery Systems 9Document46 pagesControlled Release Oral Drug Delivery Systems 9Rahul Nair50% (2)
- S02 Dispensing CalculationDocument15 pagesS02 Dispensing CalculationJoe BlackNo ratings yet
- Controlled Drug DeliveryDocument23 pagesControlled Drug DeliveryAnburaj JamesNo ratings yet
- 07 Dosage RegimenDocument44 pages07 Dosage Regimenzetttttttttt100% (3)
- Therapeutic Drug Monitoring: RVS Chaitanya KoppalaDocument33 pagesTherapeutic Drug Monitoring: RVS Chaitanya KoppalaDr. Raghavendra Kumar Gunda100% (1)
- Amity Institute of Pharmacy-NddsDocument5 pagesAmity Institute of Pharmacy-NddsTanujaNo ratings yet
- 4-Pharmacokinetics IDocument88 pages4-Pharmacokinetics IMarc Imhotep Cray, M.D.No ratings yet
- Introduction To BiopharmaceuticsDocument27 pagesIntroduction To BiopharmaceuticsAmina Akther Mim 1821179649No ratings yet
- Dose Adjustment in Renal and Hepatic FailureDocument27 pagesDose Adjustment in Renal and Hepatic Failurevanita100% (1)
- Elimination: G. SrikarDocument23 pagesElimination: G. SrikarSowjanya NekuriNo ratings yet
- RoD and BioavailibilityDocument37 pagesRoD and BioavailibilityDzil FikriNo ratings yet
- Controlled Release Drug Formulation in Pharmaceuticals: A Study On Their Application and PropertiesDocument17 pagesControlled Release Drug Formulation in Pharmaceuticals: A Study On Their Application and PropertiesintanNo ratings yet
- Multiple Dosage RegimenDocument27 pagesMultiple Dosage Regimenpradeep kumar88% (16)
- Sustained Controlled ReleaseDocument43 pagesSustained Controlled Releasesukanya100% (1)
- Non Linear PharmacokineticsDocument12 pagesNon Linear PharmacokineticsTeena Mano JoiceNo ratings yet
- ToxicokineticsDocument17 pagesToxicokineticsAshwin Ben JamesNo ratings yet
- Biopharmacy Full Text PDFDocument173 pagesBiopharmacy Full Text PDFEimy NaomyNo ratings yet
- General PharmacologyDocument101 pagesGeneral PharmacologyAditya RathoreNo ratings yet
- Solid Dosage FormsDocument4 pagesSolid Dosage Formscofodike1No ratings yet
- Hepatic ClearanceDocument14 pagesHepatic ClearanceMohamed MarzoukNo ratings yet
- Biopharmaceutics Note 7th SemDocument38 pagesBiopharmaceutics Note 7th Semmj.vinoth@gmail.comNo ratings yet
- Physiologic Pharmacokinetic ModelDocument20 pagesPhysiologic Pharmacokinetic ModelKamrun Nesa100% (1)
- Chapter 5. Intravenous InfusionDocument22 pagesChapter 5. Intravenous InfusionbencleeseNo ratings yet
- Bioavailability and First Pass MetabolismDocument37 pagesBioavailability and First Pass MetabolismFitrye Yhana Rayyi KurniawanNo ratings yet
- Drug Interactions of Digoxin - P-GlycoproteinDocument2 pagesDrug Interactions of Digoxin - P-GlycoproteinPharmazell100% (1)
- Protein BindingDocument22 pagesProtein BindingDeepakNo ratings yet
- Drug Extraction RatioDocument8 pagesDrug Extraction RatioHeru Fajar SyaputraNo ratings yet
- 9 Mô hình hai ngăn, Không tuyến tính, PKPDDocument45 pages9 Mô hình hai ngăn, Không tuyến tính, PKPDthuong nguyen thiNo ratings yet
- Classification of Biopharmaceutics SystemDocument19 pagesClassification of Biopharmaceutics SystemMoganaa LakshmiNo ratings yet
- MR Drug DeliveryDocument56 pagesMR Drug DeliveryMoganaa LakshmiNo ratings yet
- 03.transdermal Drug Delivery SystemsDocument56 pages03.transdermal Drug Delivery SystemsMoganaa LakshmiNo ratings yet
- Nomenclature of Polymer XXDocument14 pagesNomenclature of Polymer XXMoganaa LakshmiNo ratings yet
- Type of Polymer (Classification) : Pharmaceutical Chemistry Unit School of Pharmacy Management & Science UniversityDocument20 pagesType of Polymer (Classification) : Pharmaceutical Chemistry Unit School of Pharmacy Management & Science UniversityMoganaa LakshmiNo ratings yet
- Introduction of PolymerDocument29 pagesIntroduction of PolymerMoganaa LakshmiNo ratings yet
- Gastrostomy, Duodenostomy and Jejunostomy Nursing ResponsibilitiesDocument5 pagesGastrostomy, Duodenostomy and Jejunostomy Nursing ResponsibilitiesRocco WalksNo ratings yet
- Steps To A Successful Patient CounsellingDocument4 pagesSteps To A Successful Patient CounsellingRoselyn DawongNo ratings yet
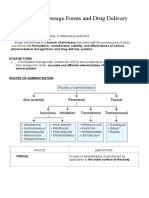
- Introduction To Dosage Forms and Drug Delivery Systems: PharmaceuticsDocument20 pagesIntroduction To Dosage Forms and Drug Delivery Systems: PharmaceuticsJelight Faith Salero GachoNo ratings yet
- MCQ PharmacologyDocument140 pagesMCQ PharmacologyVazeerNo ratings yet
- Doxorubicin and Ifosfamide Sarcoma Protocol V1.0Document8 pagesDoxorubicin and Ifosfamide Sarcoma Protocol V1.0Joseph TrevinoNo ratings yet
- Immunotherapy in Bladder Cancer: Present and Future: Inmunoterapia en Cáncer Vesical. Presente y FuturoDocument19 pagesImmunotherapy in Bladder Cancer: Present and Future: Inmunoterapia en Cáncer Vesical. Presente y FuturoIrvin SantiagoNo ratings yet
- Gastro Recommendation DCGI SecDocument3 pagesGastro Recommendation DCGI SecDipan KadiaNo ratings yet
- General Pharmacology 1Document59 pagesGeneral Pharmacology 1Ramadi PrameelaNo ratings yet
- New Drugs and Clinical Trials Rules, 2019 - A Regulatory Overview - India Corporate LawDocument7 pagesNew Drugs and Clinical Trials Rules, 2019 - A Regulatory Overview - India Corporate LawMeghna SinghNo ratings yet
- DR Tommy - Cancer PainDocument60 pagesDR Tommy - Cancer Painrisalbalu100% (1)
- Water-Versus Land-Based Exercise Effects On Physical Fitness in Older WomenDocument8 pagesWater-Versus Land-Based Exercise Effects On Physical Fitness in Older WomenHONGJY100% (1)
- Indonesia Pharmaceutical Industry Directory 2013sDocument237 pagesIndonesia Pharmaceutical Industry Directory 2013sMutiaraTitaniNo ratings yet
- 2014-Brochure LeaderflexDocument2 pages2014-Brochure LeaderflexRaji VeeramalluNo ratings yet
- Clarification Billing by CGHS Empanelled Hospitals 10 Nov 22Document3 pagesClarification Billing by CGHS Empanelled Hospitals 10 Nov 22Nilesh SethNo ratings yet
- Study of Antidiabetic Drug GlyburideDocument19 pagesStudy of Antidiabetic Drug GlyburideRaviNo ratings yet
- Pharmacology in Rehabilitation 4th EditionDocument682 pagesPharmacology in Rehabilitation 4th EditionSarah JaneNo ratings yet
- Pharmaceutics-Ii (2131) Theory: 75 Hours (3 Hours/week), Practical: 75 Hours (Total 6 Hours/Week, 3 Hours/Week Per Batch)Document21 pagesPharmaceutics-Ii (2131) Theory: 75 Hours (3 Hours/week), Practical: 75 Hours (Total 6 Hours/Week, 3 Hours/Week Per Batch)Harshal DodkeNo ratings yet
- Metod Farmakologiya Mediko Profilakticheskoe Delo-001Document91 pagesMetod Farmakologiya Mediko Profilakticheskoe Delo-001pvrzhm3No ratings yet
- AntidepressantsDocument31 pagesAntidepressantsIzhaan AkmalNo ratings yet
- Weaning From Mechanical VentilationDocument3 pagesWeaning From Mechanical VentilationAliaskar HasaniNo ratings yet
- TG Chapter15Document12 pagesTG Chapter15ibrahim muashiNo ratings yet
- Nnebulizer Drugs PDFDocument3 pagesNnebulizer Drugs PDFDianaNo ratings yet
- 3 - RN3 Networks AugustDocument200 pages3 - RN3 Networks AugustSereenaNo ratings yet
- Medisiddh Pharma Private Limited 971A/6, Thirumal Nagar, Near K.R Arts College-Nh7, Kovilpatti-628503 LICENSE NO: 490/25DDocument2 pagesMedisiddh Pharma Private Limited 971A/6, Thirumal Nagar, Near K.R Arts College-Nh7, Kovilpatti-628503 LICENSE NO: 490/25Dhk_scribdNo ratings yet
- Platelet Function After Intramuscular Diclofenac: PagesDocument4 pagesPlatelet Function After Intramuscular Diclofenac: PagesTeguh D. WicaksonoNo ratings yet
- SsDocument260 pagesSsSanju VisuNo ratings yet