Download as docx, pdf, or txt
You might also like
- USMLE Step 1 ChecklistDocument16 pagesUSMLE Step 1 Checklistmariana PeraltaNo ratings yet
- Path DumpsDocument44 pagesPath DumpsAndleeb ImranNo ratings yet
- NSAIDDocument1 pageNSAIDShubhangiNo ratings yet
- Tufts Med ListDocument5 pagesTufts Med ListMarisa Deana Pontrelli100% (1)
- Pharmacology Mnemonics PDFDocument140 pagesPharmacology Mnemonics PDFHelene AlawamiNo ratings yet
- Pharmacology Notes (Chapter 20 and 21)Document2 pagesPharmacology Notes (Chapter 20 and 21)graycorypNo ratings yet
- Migraine LeafletDocument6 pagesMigraine LeafletEliza Sitinjak100% (1)
- Pharmacology Mnemonics: SinduDocument14 pagesPharmacology Mnemonics: SinduSindu SaiNo ratings yet
- Pharmacology Drug ChartDocument50 pagesPharmacology Drug ChartEssentialForLivingNo ratings yet
- First Aid of Psychiatry (PDFDrive)Document223 pagesFirst Aid of Psychiatry (PDFDrive)Bakir JaberNo ratings yet
- Prefix Suffix MnemonicsDocument5 pagesPrefix Suffix MnemonicsPj MontecilloNo ratings yet
- Pharmacology A - NSAIDSDocument14 pagesPharmacology A - NSAIDSselflessdoctorNo ratings yet
- Kaplan Notes. ExamenSO IMPORTANTDocument145 pagesKaplan Notes. ExamenSO IMPORTANTLisaNo ratings yet
- 3 Treatment of HypertensionDocument7 pages3 Treatment of HypertensiontiaraNo ratings yet
- Path Concept MapsDocument113 pagesPath Concept MapsAndleeb ImranNo ratings yet
- Antibiotic GuideDocument6 pagesAntibiotic GuideAnnTran100% (1)
- A New Way of Mnemonics - Hypertension-cough-asthma-NSAID - WMDocument26 pagesA New Way of Mnemonics - Hypertension-cough-asthma-NSAID - WMKartik Mendiratta100% (1)
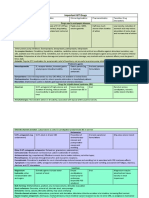
- Important GIT DrugsDocument3 pagesImportant GIT DrugsAndleeb ImranNo ratings yet
- Pharm C Exam 10 Drug ListDocument2 pagesPharm C Exam 10 Drug ListVokdadaNo ratings yet
- Cancer Drugs Drugs Indication Adverse Effects Interaction and ContraindicationDocument5 pagesCancer Drugs Drugs Indication Adverse Effects Interaction and ContraindicationOndari gisemba OSINDENo ratings yet
- Bipolar Disorder Background: Hypomania Has The Same Symptoms of Mania Without Psychotic SymptomsDocument2 pagesBipolar Disorder Background: Hypomania Has The Same Symptoms of Mania Without Psychotic SymptomshumdingerNo ratings yet
- Drug-Drug InteractionDocument9 pagesDrug-Drug InteractionHo Shi XianNo ratings yet
- Drug Interactions: What Is An Interaction?Document4 pagesDrug Interactions: What Is An Interaction?Leyla MajundaNo ratings yet
- Goljan - Integrated Pathology Notes PDFDocument60 pagesGoljan - Integrated Pathology Notes PDFIsaac JacksNo ratings yet
- NERVOUS MnemonicsDocument4 pagesNERVOUS MnemonicsHimNo ratings yet
- Gout DrugsDocument1 pageGout DrugsMichael BrownNo ratings yet
- Pharmacology TableDocument9 pagesPharmacology TableMaryam KhushbakhatNo ratings yet
- Mechanism of Action For Each Class of AntiDocument146 pagesMechanism of Action For Each Class of AntiReynaldo RiveraNo ratings yet
- Pharm TableDocument35 pagesPharm TableHannah BaldwinNo ratings yet
- Mu 002Document10 pagesMu 002chandanNo ratings yet
- Step 1 DrugsDocument46 pagesStep 1 DrugsZebram ZeeNo ratings yet
- Ultimate Pharm GuideDocument41 pagesUltimate Pharm GuideeanguyenNo ratings yet
- Characterstic Drug ToxicitiesDocument3 pagesCharacterstic Drug ToxicitiesJorge PalazzoloNo ratings yet
- Antihistamines - AMBOSS PDFDocument5 pagesAntihistamines - AMBOSS PDFOpio IsaacNo ratings yet
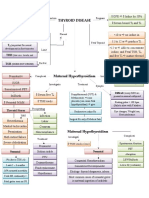
- Thyroid DiseaseDocument1 pageThyroid DiseaseZiyadNo ratings yet
- Pharmacology FirecrackerDocument37 pagesPharmacology FirecrackerRehan Usman100% (1)
- Physiology Clinical Diagnosis Treatment: TSI AntibodiesDocument10 pagesPhysiology Clinical Diagnosis Treatment: TSI Antibodies85robertNo ratings yet
- Pharmacology Mechanisms - Flash CardsDocument41 pagesPharmacology Mechanisms - Flash CardsrapstarphNo ratings yet
- STEP 1 ChecklistDocument11 pagesSTEP 1 ChecklistHasan Khan RoudbaryNo ratings yet
- Reference: Chapter 47. Basic and Clinical Pharmacology - 13th Edition. Katzung and Trevor. Lec GuideDocument8 pagesReference: Chapter 47. Basic and Clinical Pharmacology - 13th Edition. Katzung and Trevor. Lec GuideselflessdoctorNo ratings yet
- NHS Antibiotice PDFDocument2 pagesNHS Antibiotice PDFHoratiu OanaNo ratings yet
- Diabetes Treatment: PancreatitisDocument2 pagesDiabetes Treatment: PancreatitisSafiya JamesNo ratings yet
- (CV2) Pharmacology of AnticoagulantsDocument6 pages(CV2) Pharmacology of AnticoagulantsHanifa Shereen B. AliNo ratings yet
- Drug Recommendation GuideDocument6 pagesDrug Recommendation GuideGenNo ratings yet
- Prescription Regulation Summary Chart (Summary of Laws)Document2 pagesPrescription Regulation Summary Chart (Summary of Laws)roxiemannNo ratings yet
- Antihypotensive Drugs: Roger Joseph Ii Ramos Jecino, RN, M.DDocument28 pagesAntihypotensive Drugs: Roger Joseph Ii Ramos Jecino, RN, M.DFranz Earl Niño AlbesaNo ratings yet
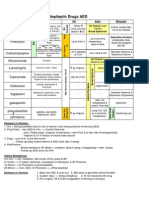
- Antiepileptic Drugs AED: D' DI Disadv SE AdvDocument1 pageAntiepileptic Drugs AED: D' DI Disadv SE Advrayooona88No ratings yet
- AntiemeticsDocument25 pagesAntiemeticsPridho GaziansyahNo ratings yet
- Antifungal Agents: EchinocandinsDocument2 pagesAntifungal Agents: EchinocandinsCourtney TownsendNo ratings yet
- Micro Chart #3 - Italics OnlyDocument27 pagesMicro Chart #3 - Italics Onlyapi-26938624100% (1)
- Ebr Hy CluesDocument16 pagesEbr Hy CluesStaporn KasemsripitakNo ratings yet
- Common Drugs AntidotesDocument3 pagesCommon Drugs AntidotesJhix JadraqueNo ratings yet
- Classification of Drugs PDFDocument15 pagesClassification of Drugs PDFmuhammad ihtisham ul hassanNo ratings yet
- Medicine Epidemiology (MedicalBooksVN - Com)Document34 pagesMedicine Epidemiology (MedicalBooksVN - Com)Jonathan AiresNo ratings yet
- Immunosuppressants - AMBOSS PDFDocument7 pagesImmunosuppressants - AMBOSS PDFOpio IsaacNo ratings yet
- AntimicrobialsDocument1 pageAntimicrobialsRomaine Barrett100% (1)
- ChemotherapyDocument11 pagesChemotherapyNedaAbdullahNo ratings yet
- Klasifikasi Dan Mekanisme ABDocument8 pagesKlasifikasi Dan Mekanisme ABDeboyjackNo ratings yet
- Pharmacology Notes: By: Khurram AbbasDocument48 pagesPharmacology Notes: By: Khurram AbbasAsma AnjumNo ratings yet
- (Pha) Le 5Document19 pages(Pha) Le 5Gabby TanNo ratings yet
- Path Concept MapsDocument113 pagesPath Concept MapsAndleeb ImranNo ratings yet
- PATH All TA Reviews Answers and Notes11Document718 pagesPATH All TA Reviews Answers and Notes11Andleeb Imran100% (1)
- Important GIT DrugsDocument3 pagesImportant GIT DrugsAndleeb ImranNo ratings yet
- PATH 1 ALL Lectures Final1Document2,054 pagesPATH 1 ALL Lectures Final1Andleeb Imran100% (1)
- Cystic Fibrosis Article - RCCADocument9 pagesCystic Fibrosis Article - RCCAAndleeb ImranNo ratings yet
- Path Quizzes and DocsDocument248 pagesPath Quizzes and DocsAndleeb Imran100% (1)
- Hematology - BNBDocument4 pagesHematology - BNBAndleeb ImranNo ratings yet
- Drugs Used in The Treatment of Malaria.: Drug Uses Adverse Effects ChloroquineDocument4 pagesDrugs Used in The Treatment of Malaria.: Drug Uses Adverse Effects ChloroquineAndleeb ImranNo ratings yet
- Money in The Bank HistoDocument16 pagesMoney in The Bank HistoAndleeb ImranNo ratings yet
- Chapter 35. Headache, Self-Assessment QuestionsDocument5 pagesChapter 35. Headache, Self-Assessment Questionstsegaab yosephNo ratings yet
- E Book Ayurvision 2010Document61 pagesE Book Ayurvision 2010ayurveda_kmc50% (2)
- LEARNING MODULE IN NCM 106 Final Peroid 2Document30 pagesLEARNING MODULE IN NCM 106 Final Peroid 2Threcia RotaNo ratings yet
- Pelzer Et Al 2023 Neurological and Psychiatric Comorbidities of Migraine Concepts and Future PerspectivesDocument15 pagesPelzer Et Al 2023 Neurological and Psychiatric Comorbidities of Migraine Concepts and Future Perspectivespaulo gutierrezNo ratings yet
- Migrain Guidelines by MedscapeDocument18 pagesMigrain Guidelines by MedscapeAlfionita HardaniNo ratings yet
- Amine Autacoids: Histamine & 5-HydroxytryptamineDocument25 pagesAmine Autacoids: Histamine & 5-HydroxytryptamineJames PerianayagamNo ratings yet
- Thesis Statement Heart DiseaseDocument7 pagesThesis Statement Heart Diseasexgkeiiygg100% (2)
- Headaches Clinical Case PDFDocument38 pagesHeadaches Clinical Case PDFGholam AdeliNo ratings yet
- Drug Interactions-Principles Examples and ClinicalDocument13 pagesDrug Interactions-Principles Examples and ClinicalRaudhatul JannahNo ratings yet
- FavotriptanDocument12 pagesFavotriptansandyriaaaNo ratings yet
- A Study of Migraine Characteristics in Joint Hypermobility Syndrome A.K.A. Ehlers-Danlos Syndrome, Hypermobility TypeDocument11 pagesA Study of Migraine Characteristics in Joint Hypermobility Syndrome A.K.A. Ehlers-Danlos Syndrome, Hypermobility TypeAndrea MorenoNo ratings yet
- gl0087 PDFDocument58 pagesgl0087 PDFNurul HikmahNo ratings yet
- Relert Tablets: 1. Qualitative and Quantitative CompositionDocument9 pagesRelert Tablets: 1. Qualitative and Quantitative Compositionddandan_2No ratings yet
- Zolmitraptan Nasal Spray - PPTDocument21 pagesZolmitraptan Nasal Spray - PPTNARESH JANDIALNo ratings yet
- Basil and MigrainesDocument9 pagesBasil and MigrainesEstefania BatemanNo ratings yet
- What Is A Migraine Headache?Document18 pagesWhat Is A Migraine Headache?mrsarojnayak8840No ratings yet
- Migraine - A Comprehensive GuideDocument29 pagesMigraine - A Comprehensive GuideNatalie MbonjaniNo ratings yet
- BotoxDocument3 pagesBotoxapi-455226234No ratings yet
- Instructions For Use of Disposable Sumatriptan Injection (Autoinjector)Document6 pagesInstructions For Use of Disposable Sumatriptan Injection (Autoinjector)Lina BuitragoNo ratings yet
- Combined Analgesics in (Headache) Pain Therapy: Shotgun Approach or Precise Multi-Target Therapeutics?Document15 pagesCombined Analgesics in (Headache) Pain Therapy: Shotgun Approach or Precise Multi-Target Therapeutics?NirmalaNo ratings yet
- Revell 2014Document6 pagesRevell 2014kemoNo ratings yet
- SDL 21 Headaches BMS16091064Document8 pagesSDL 21 Headaches BMS16091064Jonathan YeohNo ratings yet
- Migraine. e BookDocument532 pagesMigraine. e BookfaisalNo ratings yet
- Migraine & Cluster HeadachesDocument12 pagesMigraine & Cluster HeadachesBigabwa BernardNo ratings yet
- The Use of Cannabis For Headache DisordersDocument11 pagesThe Use of Cannabis For Headache DisordersNazmi ZegarraNo ratings yet
- AutacoidDocument28 pagesAutacoidPKay RecordsNo ratings yet
- Acute Management of Pediatric Cyclic Vomiting Syndrome A Systematic ReviewDocument11 pagesAcute Management of Pediatric Cyclic Vomiting Syndrome A Systematic ReviewNanda WibowoNo ratings yet
- IMITREX (Sumatriptan Succinate) InjectionDocument22 pagesIMITREX (Sumatriptan Succinate) InjectionmulkideepakNo ratings yet
- Neuro Passmedicin 2020Document1,102 pagesNeuro Passmedicin 2020Vikrant100% (1)