Download as pdf or txt
You might also like
- PSYCH 505 Case Study Core FunctionsDocument8 pagesPSYCH 505 Case Study Core FunctionsHugsNo ratings yet
- Adult Infectious Disease Bulletpoints HandbookFrom EverandAdult Infectious Disease Bulletpoints HandbookRating: 4.5 out of 5 stars4.5/5 (9)
- VancomycinDocument3 pagesVancomycinGwyn Rosales100% (3)
- Genentech - Capacity PlanningDocument7 pagesGenentech - Capacity PlanningTejas MahajanNo ratings yet
- Orthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingFrom EverandOrthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingNo ratings yet
- 04.the Cleveland Clinic Intensive Review of Pediatrics 2nd EdDocument513 pages04.the Cleveland Clinic Intensive Review of Pediatrics 2nd EdSav GaNo ratings yet
- Introduction To PeriodontologyDocument33 pagesIntroduction To PeriodontologyEmine Alaaddinoglu100% (1)
- Ob Gyn AdultDocument3 pagesOb Gyn AdultHarshit RastogiNo ratings yet
- Central Nervous System InfectionsDocument9 pagesCentral Nervous System InfectionsSaddamNo ratings yet
- Empiric Treatment Guidelines Common InfectionsDocument9 pagesEmpiric Treatment Guidelines Common InfectionsShiza Batool100% (1)
- NICU ABX ChartDocument11 pagesNICU ABX ChartdrchiNo ratings yet
- Antibiotic Guidelines For BONE AND JOINT INFECTIONSDocument3 pagesAntibiotic Guidelines For BONE AND JOINT INFECTIONSKhurram NadeemNo ratings yet
- Pocket Guide June2013 PDFDocument2 pagesPocket Guide June2013 PDFSergeyGruntov100% (1)
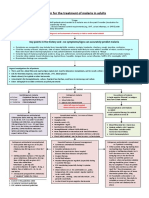
- Management of CAP in Adults - Ontario GovernmentDocument2 pagesManagement of CAP in Adults - Ontario GovernmentSukhvir AujlaNo ratings yet
- Antibiotic Guidelines For SKIN AND SOFT TISSUE INFECTIONSDocument11 pagesAntibiotic Guidelines For SKIN AND SOFT TISSUE INFECTIONSlaptopgreyNo ratings yet
- Vancomycin DRUGSTUDYDocument3 pagesVancomycin DRUGSTUDYEmagra AzilNo ratings yet
- IMG EmpAposterDocument1 pageIMG EmpAposterChiu LeoNo ratings yet
- SHC Intra Abdominal GuidelinesDocument13 pagesSHC Intra Abdominal GuidelinesNguyễn Mạnh CườngNo ratings yet
- Solid Tumor Febrile NeutropeniaDocument12 pagesSolid Tumor Febrile NeutropeniaSimonNo ratings yet
- Escalation Guide For Gram-Negative Bacteremia StanfordDocument3 pagesEscalation Guide For Gram-Negative Bacteremia StanfordLuis MedinaNo ratings yet
- Antibiotic ProtocolDocument37 pagesAntibiotic ProtocolSrinivas VadtheNo ratings yet
- Antibiotic Protocol 2018Document10 pagesAntibiotic Protocol 2018sumayyah995No ratings yet
- CNS: Ent:: Review Antibiotic Therapy Daily - Can You: Stop? Switch? Simplify? or State Duration?Document1 pageCNS: Ent:: Review Antibiotic Therapy Daily - Can You: Stop? Switch? Simplify? or State Duration?Fitri RachmadaniNo ratings yet
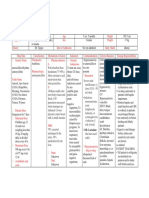
- Drug Name Mechanism of Action Indication / Contraindication Adverse Effect Nursing Responsibilities Telavancin Indications: DXDocument2 pagesDrug Name Mechanism of Action Indication / Contraindication Adverse Effect Nursing Responsibilities Telavancin Indications: DXEmilie CajaNo ratings yet
- Valgancyclovir MOA: Uses Pharmacokinetics Dosage Side Effects ContraindicationsDocument2 pagesValgancyclovir MOA: Uses Pharmacokinetics Dosage Side Effects ContraindicationsiSmayli (smyle-smayl)No ratings yet
- Bone and Joint Infections BNHFT 2010 PDFDocument3 pagesBone and Joint Infections BNHFT 2010 PDFDanissa Fidia PuteriNo ratings yet
- Classification: Cefditoren, As This Agent May CauseDocument3 pagesClassification: Cefditoren, As This Agent May CauseHavier EsparagueraNo ratings yet
- Vancomycin & Vancomycin Resistant Enterococci: Abdullah M. Kharbosh, B.SC., PharmDocument78 pagesVancomycin & Vancomycin Resistant Enterococci: Abdullah M. Kharbosh, B.SC., Pharmkharbosham100% (1)
- Antibiotic Hospital ManDocument1 pageAntibiotic Hospital Manarshiya.manasekiNo ratings yet
- Algorithm For The Treatment of Malaria in AdultsDocument1 pageAlgorithm For The Treatment of Malaria in AdultsRihab IsmaeelNo ratings yet
- Medicine RotatationbookletDocument20 pagesMedicine RotatationbookletJanelle JosephsNo ratings yet
- Candidiasis IDSA 2016Document23 pagesCandidiasis IDSA 2016Shihan HuqNo ratings yet
- DRUGSTUDYDocument8 pagesDRUGSTUDYWinnie Salazar AriolaNo ratings yet
- LevofloxacinDocument3 pagesLevofloxacinLIEZEL GRACE VELAYO100% (1)
- GNR Bacteremia De-Escalation Guide Final PDFDocument2 pagesGNR Bacteremia De-Escalation Guide Final PDFAbu Hammoud AlyazeediNo ratings yet
- 30 Glycopeptides Vancomycin and Teicoplanin 2015 Mandell Douglas and BDocument29 pages30 Glycopeptides Vancomycin and Teicoplanin 2015 Mandell Douglas and BHelen DyNo ratings yet
- NAG Sexually Transmitted InfectionsDocument24 pagesNAG Sexually Transmitted InfectionsJun JimenezNo ratings yet
- Drug Study: Adult: ChildDocument4 pagesDrug Study: Adult: ChildKristian Karl Bautista Kiw-isNo ratings yet
- Drug Study SPRDocument9 pagesDrug Study SPRKate WeyganNo ratings yet
- AmikinDocument2 pagesAmikinLIEZEL GRACE VELAYONo ratings yet
- Ampicillin DRUG STUDYDocument2 pagesAmpicillin DRUG STUDYJuliana CarpinteroNo ratings yet
- NAG Central Nervous System Infections As of Nov 2017Document9 pagesNAG Central Nervous System Infections As of Nov 2017Rhod Bernaldez EstaNo ratings yet
- Drug Study Amoxicillin PDFDocument4 pagesDrug Study Amoxicillin PDFMc SantosNo ratings yet
- 2012 Aug IMG Poster 165760a SepsisDocument1 page2012 Aug IMG Poster 165760a SepsisTeng Huei LeeNo ratings yet
- Antibiotic Pocket GuideDocument19 pagesAntibiotic Pocket GuideNaomi Liang100% (1)
- Antibiotka PicuDocument4 pagesAntibiotka Picusunu rachmat100% (1)
- AminoglycosideDocument16 pagesAminoglycosideDr. ChihiroNo ratings yet
- Gentamicin Sulfate-Drug StudyDocument3 pagesGentamicin Sulfate-Drug StudyDaisy Palisoc82% (11)
- CNS Infection GuidanceDocument2 pagesCNS Infection GuidanceGus LionsNo ratings yet
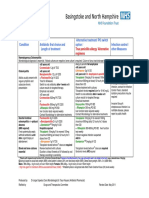
- Guidelines For First-Line Empirical Antibiotic Therapy in AdultsDocument1 pageGuidelines For First-Line Empirical Antibiotic Therapy in AdultsAnonymous s4yarxNo ratings yet
- Any Up-Dates Are To Be Completed in Different Color Ink. The Student Is Expected To Document All Meds The Client Is Currently ReceivingDocument1 pageAny Up-Dates Are To Be Completed in Different Color Ink. The Student Is Expected To Document All Meds The Client Is Currently Receivinggeorgeloto12No ratings yet
- Icu Antibiotic GuidelinesDocument4 pagesIcu Antibiotic GuidelinesTia MonitaNo ratings yet
- Severe Sepsis and Septic Shock Antibiotic Guide: Community AcquiredDocument6 pagesSevere Sepsis and Septic Shock Antibiotic Guide: Community AcquiredAnonymous G6zDTD2yNo ratings yet
- TASH Empirical Antibiotic Treatment Guidelines - 2018 Hospital and Ventilator Associated Pneumonia (HAP and VAP)Document2 pagesTASH Empirical Antibiotic Treatment Guidelines - 2018 Hospital and Ventilator Associated Pneumonia (HAP and VAP)ጉራማይሌ TubeNo ratings yet
- Pediatric Hospital-Acquired and Ventilator-Associated Pneumonia Topic DiscussionDocument5 pagesPediatric Hospital-Acquired and Ventilator-Associated Pneumonia Topic Discussionapi-602288180No ratings yet
- Acyclovir (Acycloguanosi Ne) : Systemic Administration History: AllergyDocument3 pagesAcyclovir (Acycloguanosi Ne) : Systemic Administration History: AllergyAnnahNo ratings yet
- Drug StudyDocument1 pageDrug StudyBtob meloNo ratings yet
- Febrile Neutropenia Care GuidelineDocument2 pagesFebrile Neutropenia Care GuidelinedenokayuMRNo ratings yet
- Shivani PDFDocument3 pagesShivani PDFdeepukumarNo ratings yet
- VancomycinDocument1 pageVancomycinJUSTINE ALLYSA MAY CASTILLONo ratings yet
- Monkeypox, Diagnosis and TreatmentDocument55 pagesMonkeypox, Diagnosis and TreatmentsamiNo ratings yet
- Pneumonia ADULTDocument6 pagesPneumonia ADULTSebastian TjuwatjaNo ratings yet
- Concise Guide to Clinical Dentistry: Common Prescriptions In Clinical DentistryFrom EverandConcise Guide to Clinical Dentistry: Common Prescriptions In Clinical DentistryNo ratings yet
- Opioid Equianalgesic ChartDocument1 pageOpioid Equianalgesic Chartdamondouglas100% (7)
- Why Black Women With Ovarian Cancer Require Greater FocusDocument1 pageWhy Black Women With Ovarian Cancer Require Greater FocusMicheleFontanaNo ratings yet
- Perry Chapter 7,8,9,10,11,12,14 Case Study & DefinitionsDocument15 pagesPerry Chapter 7,8,9,10,11,12,14 Case Study & Definitionstriddle1969100% (1)
- A Lens To Understand Sanitation Workers and Their Health Status in IndiaDocument3 pagesA Lens To Understand Sanitation Workers and Their Health Status in IndiaRejesh BoseNo ratings yet
- Abnormal Eye PositionDocument30 pagesAbnormal Eye PositionNimas Prita100% (1)
- Example of Health Technology Assessment (HTA) of A Therapy For The Reduction of Alcohol ConsumptionDocument18 pagesExample of Health Technology Assessment (HTA) of A Therapy For The Reduction of Alcohol ConsumptiontantanwyNo ratings yet
- FITE Primer 2021Document3 pagesFITE Primer 2021iya gerzonNo ratings yet
- Asphyxia in Forensic AspectDocument31 pagesAsphyxia in Forensic AspectSita SilastutiNo ratings yet
- Gestational Weight GainDocument3 pagesGestational Weight GainainindyaNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument2 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- Chorea Approach PDFDocument1 pageChorea Approach PDFdrsushmakNo ratings yet
- Tuffey ResumeDocument3 pagesTuffey Resumeapi-317208513No ratings yet
- Acute EkaDocument25 pagesAcute EkaranggaNo ratings yet
- Placenta Previa: View Media GalleryDocument7 pagesPlacenta Previa: View Media GalleryMargaret AssilasNo ratings yet
- Mock Exam 1 - 50Document9 pagesMock Exam 1 - 50charlotte macairan67% (3)
- Allergic Rhinitis: Dr. Fauziah Henny, SP - THT-KLDocument14 pagesAllergic Rhinitis: Dr. Fauziah Henny, SP - THT-KLIsra AbdiNo ratings yet
- Liver Abscess of Patient: Case Report and Review of The LiteratureDocument4 pagesLiver Abscess of Patient: Case Report and Review of The LiteratureReinhar RusliNo ratings yet
- Su Jok, Twist Therapy AND Smile MeditationDocument7 pagesSu Jok, Twist Therapy AND Smile MeditationprateekNo ratings yet
- Bài tập tiếng anh unit 2Document31 pagesBài tập tiếng anh unit 2Nok NokNo ratings yet
- Personal Injury Ire FormDocument2 pagesPersonal Injury Ire FormBioVeda Health and Wellness CentersNo ratings yet
- Zephrex-D National Launch News ReleaseDocument3 pagesZephrex-D National Launch News ReleaseSam LevinNo ratings yet
- Supersizeme WorksheetDocument5 pagesSupersizeme WorksheetPaola SoledadNo ratings yet
- Q-NCOV-01D STANDARD Q COVID-19 IgM-IgG Duo Test INSERTODocument2 pagesQ-NCOV-01D STANDARD Q COVID-19 IgM-IgG Duo Test INSERTOechegarayNo ratings yet
- Asia-Pacific Glaucoma Guidelines PDFDocument118 pagesAsia-Pacific Glaucoma Guidelines PDFAvilla Ane LukitoNo ratings yet
- What Is AphasiaDocument4 pagesWhat Is AphasiaValentina DubNo ratings yet
- Germany Health Benefits SummaryDocument6 pagesGermany Health Benefits Summarytracy leeNo ratings yet