Download as pdf or txt
You might also like
- Oral Pathology Mnemonics Online Course - PDF versionFrom EverandOral Pathology Mnemonics Online Course - PDF versionRating: 3.5 out of 5 stars3.5/5 (3)
- Karen - S Notes-Clinical ExaminationDocument11 pagesKaren - S Notes-Clinical ExaminationGanesh Namasivayam100% (3)
- DR Karen Short NotesDocument412 pagesDR Karen Short NotesNayantara Nair100% (2)
- Cri 188 FinalsDocument12 pagesCri 188 FinalsKaren Angel AbaoNo ratings yet
- Biochemistry Lab 2Document4 pagesBiochemistry Lab 2S. MartinezNo ratings yet
- NBDE 2012 All Remembered QsDocument54 pagesNBDE 2012 All Remembered Qschakriy9100% (6)
- CrossCore Rotational Bodyweight Training Mens Fitness ArticleDocument3 pagesCrossCore Rotational Bodyweight Training Mens Fitness Articletrt21No ratings yet
- Peter Ragnar - 3 Non Diet Secrets For Incredible VitalityDocument3 pagesPeter Ragnar - 3 Non Diet Secrets For Incredible VitalityBiljana Percinkova100% (2)
- Global Politics IB GuideDocument67 pagesGlobal Politics IB GuideMikeyJohn100% (1)
- Chinchilla SkullDocument12 pagesChinchilla Skullf.baobao28No ratings yet
- Chromosome Number Final1Document3 pagesChromosome Number Final1Janine NogueraNo ratings yet
- Tetraploidy in A 15-Month-Old GirlDocument5 pagesTetraploidy in A 15-Month-Old GirlGuy HaimNo ratings yet
- Associated DisordersDocument40 pagesAssociated DisordersSonu SonuNo ratings yet
- l3 Orthodontic Case History and Diagnosis - I 17-11-21Document57 pagesl3 Orthodontic Case History and Diagnosis - I 17-11-21Ju JuNo ratings yet
- Catatan Orthopedi AriefDocument8 pagesCatatan Orthopedi Ariefmiwer 765No ratings yet
- Orthodontic DiagnosisDocument19 pagesOrthodontic DiagnosissamNo ratings yet
- Thyroid Examination FiryaLDocument3 pagesThyroid Examination FiryaLFiryal Balushi100% (1)
- Case Seminars WorksheetDocument3 pagesCase Seminars Worksheetsnbmww5p4dNo ratings yet
- Yang2015 Pili TortiDocument3 pagesYang2015 Pili TortiErnawati HidayatNo ratings yet
- EL Husseiny's Essentials of Endocrinology 1247Document152 pagesEL Husseiny's Essentials of Endocrinology 1247حنين عاطفNo ratings yet
- Cytogenetic AbnormalitiesDocument48 pagesCytogenetic AbnormalitiesGlomelyn Rose Ortiz TañedoNo ratings yet
- Ultrasound in Obstet Gyne - 2003 - Delahaye - Prenatal Ultrasound Diagnosis of Fetal CraniosynostosisDocument7 pagesUltrasound in Obstet Gyne - 2003 - Delahaye - Prenatal Ultrasound Diagnosis of Fetal Craniosynostosisyelly puspitasariNo ratings yet
- Clinical ExaminationDocument11 pagesClinical ExaminationLaura GranadosNo ratings yet
- LMR Ent - Nose and Paransal SinusesDocument7 pagesLMR Ent - Nose and Paransal SinusesYuku BabyNo ratings yet
- Genetics Dysmorphology in Pediatrics - MedicoNotesDocument1 pageGenetics Dysmorphology in Pediatrics - MedicoNotesJ KPNo ratings yet
- ENT 1.3 Lips and Oral CavityDocument15 pagesENT 1.3 Lips and Oral CavityZazaNo ratings yet
- Clinical Examination - Karen Notes - SHIRI For BD DoctorsDocument11 pagesClinical Examination - Karen Notes - SHIRI For BD DoctorsHelp LineNo ratings yet
- Physical Examination: The Head and NeckDocument63 pagesPhysical Examination: The Head and Neckapi-19916399No ratings yet
- Goldenhar SyndromeDocument4 pagesGoldenhar Syndrometita luthfiaNo ratings yet
- GPE in ChildrenDocument4 pagesGPE in ChildrenSheera EiyraaNo ratings yet
- Diseases of Bone and JointsDocument71 pagesDiseases of Bone and JointsAMIT GUPTANo ratings yet
- Dys Morphis MDocument27 pagesDys Morphis MdrmindhackerNo ratings yet
- Bab II AaDocument7 pagesBab II AaPriskilaNo ratings yet
- Fetal Face and Neck - Student SlidesDocument35 pagesFetal Face and Neck - Student SlidessdafasdNo ratings yet
- 2 Newborn AssesmentDocument23 pages2 Newborn Assesment.No ratings yet
- Final Year Clinicals: Malocclusions and Etiology (Graber)Document31 pagesFinal Year Clinicals: Malocclusions and Etiology (Graber)Sruthy NairNo ratings yet
- Medical Terminology FixedDocument3 pagesMedical Terminology FixedBaeman KyottNo ratings yet
- AOT (Adenomatoid Odontogenic Tumor) : Pyogenic GranulomaDocument54 pagesAOT (Adenomatoid Odontogenic Tumor) : Pyogenic GranulomaSanNo ratings yet
- Orthodontic AssessmentDocument59 pagesOrthodontic AssessmentSyaifuddin ADamNo ratings yet
- cOMMON gENETIC dISORDERSDocument11 pagescOMMON gENETIC dISORDERSChari RivoNo ratings yet
- Week 1.3Document23 pagesWeek 1.3ginny.mycookiecanNo ratings yet
- Case ReportDocument18 pagesCase Reportarief wiratamaNo ratings yet
- Syndromes: ContentsDocument5 pagesSyndromes: ContentsRoshni SinghNo ratings yet
- Head Shape Abnormalities and HydrocephalusDocument7 pagesHead Shape Abnormalities and HydrocephalusZweNo ratings yet
- Genereal Examination-Anukul SurgeryDocument4 pagesGenereal Examination-Anukul SurgeryTRASH MAILNo ratings yet
- Speaker: Dr. Shafat A Mir Department of Anaesthesia and Critical Care SKIMS, Srinagar, J&k.indiaDocument74 pagesSpeaker: Dr. Shafat A Mir Department of Anaesthesia and Critical Care SKIMS, Srinagar, J&k.indiatutorial desatuNo ratings yet
- Management of Open Bite: Dr. Madhura Jayant Pednekar Iii MdsDocument75 pagesManagement of Open Bite: Dr. Madhura Jayant Pednekar Iii MdsDrKamran MominNo ratings yet
- CraniosynostosisDocument54 pagesCraniosynostosistameemNo ratings yet
- Skin and Bones 1Document6 pagesSkin and Bones 1Joseph John HiladoNo ratings yet
- Sorge 1996Document4 pagesSorge 1996jahfdfgsdjad asdhsajhajdkNo ratings yet
- Orthopedic FinalDocument858 pagesOrthopedic Finalhashmf180% (10)
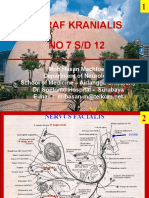
- Clerk05 Nervi KranialisDocument14 pagesClerk05 Nervi KranialisIvor Wiguna Hartanto WilopoNo ratings yet
- Mental Dental PathologyDocument19 pagesMental Dental PathologyPooja rajwarNo ratings yet
- BIMC Update PresentationDocument25 pagesBIMC Update PresentationWahyuNo ratings yet
- Congenital Malformations of The Larynx and TracheaDocument8 pagesCongenital Malformations of The Larynx and TracheaKaren EidNo ratings yet
- Head and Neck - MusclesDocument3 pagesHead and Neck - MusclesJohann Sebastian CruzNo ratings yet
- Nasal Bone Fractures: Grand Rounds Dr. Ashish GuptaDocument29 pagesNasal Bone Fractures: Grand Rounds Dr. Ashish GuptaCharan KanwalNo ratings yet
- Common SymptomsDocument72 pagesCommon SymptomsBulajyo Pangngay JolinaNo ratings yet
- Prefixes in Medical TerminologyDocument7 pagesPrefixes in Medical Terminologyalerp07100% (1)
- Crs Muthia Khanza (Isi)Document40 pagesCrs Muthia Khanza (Isi)Muthia Khanza AbuBakarNo ratings yet
- Dys MorphologyDocument62 pagesDys Morphologyamal nassarNo ratings yet
- Initial Examination Form: Jordan University of Science & Technology Faculty of Dentistry Dental Teaching CenterDocument2 pagesInitial Examination Form: Jordan University of Science & Technology Faculty of Dentistry Dental Teaching Centersadeen2249No ratings yet
- Initial Examination Form: Jordan University of Science & Technology Faculty of Dentistry Dental Teaching CenterDocument2 pagesInitial Examination Form: Jordan University of Science & Technology Faculty of Dentistry Dental Teaching Centersadeen2249No ratings yet
- Treatmant of Gummy SmileDocument33 pagesTreatmant of Gummy Smileprince wrathNo ratings yet
- Identifying A A RSK Og SyndromeDocument3 pagesIdentifying A A RSK Og SyndromeS. MartinezNo ratings yet
- PlantDerived Edible Nanoparticles and MiRNAs Emerging Frontier For Therapeutics and Targeted DrugDeliveryDocument15 pagesPlantDerived Edible Nanoparticles and MiRNAs Emerging Frontier For Therapeutics and Targeted DrugDeliveryS. MartinezNo ratings yet
- Study Design I: Experimental DesignDocument54 pagesStudy Design I: Experimental DesignS. MartinezNo ratings yet
- Determining What Analysis To Use?: - For Every Model We Will Cover You Must Ask A Series of QuestionsDocument35 pagesDetermining What Analysis To Use?: - For Every Model We Will Cover You Must Ask A Series of QuestionsS. MartinezNo ratings yet
- CHP 4: Estimating With UncertaintyDocument41 pagesCHP 4: Estimating With UncertaintyS. MartinezNo ratings yet
- Biometry Lecture 2 Part 2 PostedDocument41 pagesBiometry Lecture 2 Part 2 PostedS. MartinezNo ratings yet
- Biometry Lecture 1Document59 pagesBiometry Lecture 1S. MartinezNo ratings yet
- An Introduction To Statistical AnalysisDocument20 pagesAn Introduction To Statistical AnalysisS. MartinezNo ratings yet
- Biometry Lecture 3 PostedDocument47 pagesBiometry Lecture 3 PostedS. MartinezNo ratings yet
- Biometry Lecture 6 PostedDocument81 pagesBiometry Lecture 6 PostedS. MartinezNo ratings yet
- Liposomal Drug DeliveryDocument1 pageLiposomal Drug DeliveryS. MartinezNo ratings yet
- The Suitability of Liposomes For The Delivery of Hydrophobic Drugs - A Case Study With CurcuminDocument1 pageThe Suitability of Liposomes For The Delivery of Hydrophobic Drugs - A Case Study With CurcuminS. MartinezNo ratings yet
- Index: SL.# Description HeadingsDocument2 pagesIndex: SL.# Description HeadingsmadanhseNo ratings yet
- DOH Memo For Local Health Departments 12.3.21Document5 pagesDOH Memo For Local Health Departments 12.3.21News10NBCNo ratings yet
- Foxtail MilletDocument11 pagesFoxtail Milletbhavi kapadiaNo ratings yet
- Medical EthicsDocument25 pagesMedical Ethicsswarajudugade100% (1)
- Retirement Community ResearchDocument5 pagesRetirement Community ResearchMary Jane CabidesNo ratings yet
- Fake News, Phishing, and Fraud: A Call For Research On Digital Media Literacy Education Beyond The ClassroomDocument8 pagesFake News, Phishing, and Fraud: A Call For Research On Digital Media Literacy Education Beyond The ClassroomqwertzNo ratings yet
- NLE DIAGNOSTIC W FREE LECTUREDocument3 pagesNLE DIAGNOSTIC W FREE LECTURETrip Ni TeryoNo ratings yet
- Material Safety Data Sheet: Product IdentificationDocument4 pagesMaterial Safety Data Sheet: Product Identificationمحمد عزتNo ratings yet
- How Do You Feel About Your BodyDocument21 pagesHow Do You Feel About Your BodyFabio VanuzziNo ratings yet
- Coping Skills HandoutsDocument7 pagesCoping Skills HandoutsaharbisonNo ratings yet
- Calculating The Time Weighted Average TWA Noise Level and Noise Dose Levels PDFDocument1 pageCalculating The Time Weighted Average TWA Noise Level and Noise Dose Levels PDFananthu.uNo ratings yet
- Ligamentizacion HT Grafts After ACLDocument10 pagesLigamentizacion HT Grafts After ACLLuisa MendozaNo ratings yet
- Appendix eDocument17 pagesAppendix eTheonee LambiquitNo ratings yet
- Bilingual Reporter, Tanzania JDDocument3 pagesBilingual Reporter, Tanzania JDEng Msofe JamesNo ratings yet
- Common Application Transfer EssayDocument9 pagesCommon Application Transfer Essayafibyrirmfogiz100% (2)
- Massage Professional Ebook, 2nd EditionDocument188 pagesMassage Professional Ebook, 2nd EditionAnh Nguyễn33% (3)
- UNICEF 2016 IECDD Guidance PDFDocument60 pagesUNICEF 2016 IECDD Guidance PDFmcpaulina98No ratings yet
- Changing Faces: A Case-Based Review of Acromegaly: Special Care DentistryDocument5 pagesChanging Faces: A Case-Based Review of Acromegaly: Special Care DentistryZainab HajiNo ratings yet
- Discharge Plan, Conclusion, RecommendationDocument3 pagesDischarge Plan, Conclusion, RecommendationMenesio IlaganNo ratings yet
- ObjectiveDocument3 pagesObjectiveHazel Mae MaestradoNo ratings yet
- Murray Secretion Scale and Fiberoptic Endoscopic Evaluation of Swallowing FEESDocument7 pagesMurray Secretion Scale and Fiberoptic Endoscopic Evaluation of Swallowing FEESjmunozsilvaNo ratings yet
- Flower RemedyDocument39 pagesFlower RemedyJayant Bodhe75% (4)
- ARS - 1909CT - FAHIM MD AZMAN RAHMAN (TP057341) - Individual AssignmentDocument3 pagesARS - 1909CT - FAHIM MD AZMAN RAHMAN (TP057341) - Individual AssignmentFahim AzmanNo ratings yet
- Atls Notes and ScoresDocument2 pagesAtls Notes and ScoresElias SaeedNo ratings yet
- Indo Petroleum Nurse Grade II AdvertisementDocument4 pagesIndo Petroleum Nurse Grade II AdvertisementjaideepsdNo ratings yet
- Attwood MeltdownsDocument50 pagesAttwood MeltdownsGyorgyi Boros100% (1)