Download as docx, pdf, or txt
You might also like
- Gray File HAADDocument67 pagesGray File HAADali khanNo ratings yet
- Pharmacology For Nurses by Diane Pacitti Blaine T. SmithDocument570 pagesPharmacology For Nurses by Diane Pacitti Blaine T. SmithJessica Anis0% (1)
- Steroids Rating ChartDocument2 pagesSteroids Rating Chartthe bungalowvideotapes0% (1)
- Test Bank For Pharmacotherapeutics For Advanced Practice 3rd Edition Virginia Poole ArcangeloDocument7 pagesTest Bank For Pharmacotherapeutics For Advanced Practice 3rd Edition Virginia Poole ArcangeloShelly Duggan100% (42)
- Krok - Base PharmacologyDocument149 pagesKrok - Base PharmacologyHemant GargNo ratings yet
- CYP3A Inhibitors Inducers DDIDocument4 pagesCYP3A Inhibitors Inducers DDIAmr MuhammedNo ratings yet
- Clinically Significant Drug Interactions - AAFPDocument19 pagesClinically Significant Drug Interactions - AAFPAbchoNo ratings yet
- Clinically Significant Drug InteractionsDocument18 pagesClinically Significant Drug Interactionsmagus davilaNo ratings yet
- Warfarin INR Antibx InteractionDocument3 pagesWarfarin INR Antibx InteractionSheila UlinaNo ratings yet
- Supply Chain and Inventory ControlDocument11 pagesSupply Chain and Inventory Controlharshit1509dNo ratings yet
- Chapter 3 Hospital Pharmacy Notes Complete Notes by Noteskarts Acc To ER20Document25 pagesChapter 3 Hospital Pharmacy Notes Complete Notes by Noteskarts Acc To ER20Shamant TNo ratings yet
- Antimicrobial Drug Interactionstable220716 PDFDocument4 pagesAntimicrobial Drug Interactionstable220716 PDFBhavin DesaiNo ratings yet
- Diphos Dihydroartemisinin+Piperaquine PhosphateDocument1 pageDiphos Dihydroartemisinin+Piperaquine PhosphateMuhammad Azhar SattarNo ratings yet
- Interaksi Obat Hematologi (DR - Wati) 22-12-15 PDFDocument5 pagesInteraksi Obat Hematologi (DR - Wati) 22-12-15 PDFFiqrotul UmamNo ratings yet
- Liver Cirrhosis Drug StudyDocument3 pagesLiver Cirrhosis Drug StudyRachel QuionNo ratings yet
- Antimicrobial Dosage Adjustments in Renal Impairment For FormularyDocument20 pagesAntimicrobial Dosage Adjustments in Renal Impairment For Formularyangkatanjuli2019No ratings yet
- Generic Name: Fluconazole Brand Name: Diflucan Dosage: Classification: IndicationDocument1 pageGeneric Name: Fluconazole Brand Name: Diflucan Dosage: Classification: IndicationCen Janber CabrillosNo ratings yet
- Pharmaceutical Assessment Plan and Follow Up Sheet DVT 2Document5 pagesPharmaceutical Assessment Plan and Follow Up Sheet DVT 2Turkish DizilerNo ratings yet
- MedicationDocument4 pagesMedicationkayalNo ratings yet
- AntikoagulanDocument70 pagesAntikoagulanFian AldyNo ratings yet
- New Oral New Oral Anticoagulants G: RB H TT MD Rebecca Hanratty, MD Denver Health April 12, 2011Document55 pagesNew Oral New Oral Anticoagulants G: RB H TT MD Rebecca Hanratty, MD Denver Health April 12, 2011andresrgomezNo ratings yet
- Rivaroxaban PresentationDocument13 pagesRivaroxaban PresentationReem El-HusseinyNo ratings yet
- Anticoagulant: Mechanism and ReverseDocument22 pagesAnticoagulant: Mechanism and ReverseNovi Riyadhah Ma'sumNo ratings yet
- Information For Pharmacists On Managing Warfarin Drug InteractionsDocument4 pagesInformation For Pharmacists On Managing Warfarin Drug InteractionsBelladonna Perdana PutraNo ratings yet
- PhentermineDocument1 pagePhentermineCarolina Leiva FioreNo ratings yet
- Anti-Coagulant (Vte in Obstetrics) - Madam LiewDocument10 pagesAnti-Coagulant (Vte in Obstetrics) - Madam LiewNana YunusNo ratings yet
- Anticoagulants and The Perioper - 2006 - Continuing Education in Anaesthesia CriDocument4 pagesAnticoagulants and The Perioper - 2006 - Continuing Education in Anaesthesia Crironaldquezada038No ratings yet
- 1 - DopamineDocument1 page1 - DopaminedianneangelaNo ratings yet
- Drugs Interactions With WarfarinDocument7 pagesDrugs Interactions With WarfarinAsmaa RadwanNo ratings yet
- Heparin Vs Warfarin (Coumadin)Document5 pagesHeparin Vs Warfarin (Coumadin)blankNo ratings yet
- 1388 Cardiovascular Drugs: Interactions Units Adverse Effects, Treatment, and PrecautionsDocument2 pages1388 Cardiovascular Drugs: Interactions Units Adverse Effects, Treatment, and PrecautionsPopov VictorNo ratings yet
- Oncology Cheat Sheets - 1Document5 pagesOncology Cheat Sheets - 1abdallahmaurice94No ratings yet
- Newer Oral Anticoagulants: Dabigatran Etexilate Is An Inactive Pro-DrugDocument5 pagesNewer Oral Anticoagulants: Dabigatran Etexilate Is An Inactive Pro-DrugLouiseNo ratings yet
- Treatment of MalariaDocument49 pagesTreatment of MalariaShanza AmaanNo ratings yet
- Antibiotic Pharmacokinetics & Pharmacodynamics: Bacteriostatic BactericidalDocument4 pagesAntibiotic Pharmacokinetics & Pharmacodynamics: Bacteriostatic BactericidalMd NoumanNo ratings yet
- Drug StudyDocument9 pagesDrug StudyAysaaa DCNo ratings yet
- Low Molecular Weight Heparins Summary Prescribing Guide Version 1.3Document14 pagesLow Molecular Weight Heparins Summary Prescribing Guide Version 1.3sharief145No ratings yet
- Table 15-5 - High-Risk Medications For Potential Drug-Drug IntDocument2 pagesTable 15-5 - High-Risk Medications For Potential Drug-Drug IntDragutin PetrićNo ratings yet
- ErythromycinDocument2 pagesErythromycinEurielle MioleNo ratings yet
- Chapter 8 Malignant DiseaseDocument6 pagesChapter 8 Malignant DiseaseAjmalNo ratings yet
- List of Top Ten Drug Interactions in Long-Term CareDocument8 pagesList of Top Ten Drug Interactions in Long-Term Careanon_511980284No ratings yet
- Phenytoin TDMDocument29 pagesPhenytoin TDMft84nzzc92No ratings yet
- L8 Anti Coagulant DrugsDocument10 pagesL8 Anti Coagulant DrugsamanabduwahabNo ratings yet
- Anti Coagulants & FibrinolyticsDocument54 pagesAnti Coagulants & FibrinolyticsSunanda mohanNo ratings yet
- Nejmra1200894 AppendixDocument14 pagesNejmra1200894 AppendixStephan CanoNo ratings yet
- Folfiri+cetu Gi Col PDocument12 pagesFolfiri+cetu Gi Col PJayelle2No ratings yet
- Low Molecular Weigh Heparins Summary Prescribing Guide Version 14Document15 pagesLow Molecular Weigh Heparins Summary Prescribing Guide Version 14alexandr zinchenkoNo ratings yet
- Pizotifen MalateDocument2 pagesPizotifen MalatesadafNo ratings yet
- Antimarial Agents - Olaleye's Handout: Blood Schizonticide Both inDocument4 pagesAntimarial Agents - Olaleye's Handout: Blood Schizonticide Both inhoa1212No ratings yet
- Heparin and WarfarinDocument3 pagesHeparin and WarfarinannieNo ratings yet
- RX Cheat Sheet Pharmacy CrackDocument1 pageRX Cheat Sheet Pharmacy Crackramesh kumar100% (1)
- Drug Study UtiDocument4 pagesDrug Study UtiClaire MachicaNo ratings yet
- Generic Name: Classification: Indication:: Candida InfectionsDocument1 pageGeneric Name: Classification: Indication:: Candida Infectionscen janber cabrillos0% (1)
- Malaria Managment Algorithm 202208Document1 pageMalaria Managment Algorithm 202208Marianne Joy PontigonNo ratings yet
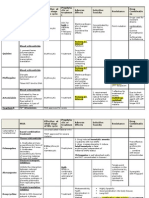
- Drug Classification Dosage/ Frequency /route Mechanism of Action Indication Contra-Indication Adverse Effects Nursing ResponsibilitiesDocument2 pagesDrug Classification Dosage/ Frequency /route Mechanism of Action Indication Contra-Indication Adverse Effects Nursing ResponsibilitiesLouisse Angeli AbucejoNo ratings yet
- Drug Study Batmc GeriaDocument3 pagesDrug Study Batmc GeriaLeslee Amor EspirituNo ratings yet
- NPS Antibiotic Use in UTIs (May 2002)Document2 pagesNPS Antibiotic Use in UTIs (May 2002)miloano8989No ratings yet
- SMPC Co Arinate Adult JNa.2018.03Document6 pagesSMPC Co Arinate Adult JNa.2018.03kelinaphiri01No ratings yet
- General Indications: AnticoagulantsDocument15 pagesGeneral Indications: AnticoagulantswahidNo ratings yet
- Anticoagulants May BeDocument5 pagesAnticoagulants May BeAmmar magdyNo ratings yet
- Clinical Practice Guide On Antithrombotic Drug Dosing and Management of Antithrombotic Drug-Associated Bleeding Complications in AdultsDocument8 pagesClinical Practice Guide On Antithrombotic Drug Dosing and Management of Antithrombotic Drug-Associated Bleeding Complications in AdultsdarekshepardNo ratings yet
- DRUG SUMMARY TABLE - Anticoagulantes y AntiagregantesDocument3 pagesDRUG SUMMARY TABLE - Anticoagulantes y AntiagregantesManuel BetancurNo ratings yet
- Alfuzosin + Dutasteride Alfusin-D Medication Patient InformationDocument21 pagesAlfuzosin + Dutasteride Alfusin-D Medication Patient Informationgarciamaratin54No ratings yet
- Medication: Emersonhurley Oxytocics orDocument1 pageMedication: Emersonhurley Oxytocics orEmerson HurleyNo ratings yet
- Critical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsNo ratings yet
- PFSA - S Pharmaceuticals ListDocument80 pagesPFSA - S Pharmaceuticals ListDNo ratings yet
- Opioids A ReviewDocument19 pagesOpioids A ReviewAlan padilla sesma100% (1)
- 383817KZDocument13 pages383817KZSreya SanilNo ratings yet
- Final XylazineDocument4 pagesFinal XylazineJessica A. BotelhoNo ratings yet
- Pembuatan tablet159103-ID-pengaruh-ac-di-sol-terhadap-karakteristiDocument9 pagesPembuatan tablet159103-ID-pengaruh-ac-di-sol-terhadap-karakteristiAhmad MujadidNo ratings yet
- Daftar Harga 2017 Pt. Antarmitra SembadaDocument49 pagesDaftar Harga 2017 Pt. Antarmitra SembadaAyu RiskaNo ratings yet
- Marcas Importadas 2022Document3 pagesMarcas Importadas 2022Luan GabrielNo ratings yet
- 保健中心藥品清單Document2 pages保健中心藥品清單台大家醫部總醫師No ratings yet
- Lista Proselca 01-06-2021Document24 pagesLista Proselca 01-06-2021Patty Yois B. LarriegaNo ratings yet
- Week 8.2Document74 pagesWeek 8.2ginny.mycookiecanNo ratings yet
- JNM 25 006Document9 pagesJNM 25 006sahama2508No ratings yet
- Aac 02167-19Document17 pagesAac 02167-19leokadiobarroso.rjNo ratings yet
- PrescriptionDocument2 pagesPrescriptionBiswaranjanPanigrahiNo ratings yet
- Daftar Obat EthicalDocument11 pagesDaftar Obat EthicalhusnulNo ratings yet
- Nursing Pharmacology - Rollant, Paulette D Hill, Karen, RN - 1996 - St. Louis, MO - Mosby-Year BookDocument404 pagesNursing Pharmacology - Rollant, Paulette D Hill, Karen, RN - 1996 - St. Louis, MO - Mosby-Year BookaltalunedemiNo ratings yet
- D Pharma PaperDocument5 pagesD Pharma Paperved bhaskerNo ratings yet
- APPENDIX A B GlossaryDocument15 pagesAPPENDIX A B GlossaryaddiramonaNo ratings yet
- Medcard Warfarin (Coumadin)Document3 pagesMedcard Warfarin (Coumadin)Tricia SicbaldiNo ratings yet
- Mental Health Nursing 6Th Edition Fontaine Test Bank Full Chapter PDFDocument17 pagesMental Health Nursing 6Th Edition Fontaine Test Bank Full Chapter PDFkhuyentryphenakj1100% (13)
- Biopharmaceutical Brochure (ENG)Document19 pagesBiopharmaceutical Brochure (ENG)Edson BritoNo ratings yet
- TEST BANK For Focus On Nursing Pharmacology 8th Edition by Amy KarchDocument8 pagesTEST BANK For Focus On Nursing Pharmacology 8th Edition by Amy KarchYassine HaddadeNo ratings yet
- What Are DrugsDocument7 pagesWhat Are DrugsMelvin Jay Reyes BaluranNo ratings yet
- Table 3. Vulvovaginal Candidiasis Treatment Options: Fluconazole 150mg PO Stat (1B)Document2 pagesTable 3. Vulvovaginal Candidiasis Treatment Options: Fluconazole 150mg PO Stat (1B)neleaNo ratings yet
- Stock 27 Sept 23Document16 pagesStock 27 Sept 23hadiprayitno.agustusNo ratings yet
- DILIrank-DILIscore ListDocument48 pagesDILIrank-DILIscore ListA94-WONG JING TONGNo ratings yet