Download as pdf or txt
You might also like
- Module Five Wellness Plan HOPEDocument15 pagesModule Five Wellness Plan HOPEZelda Raniblanket100% (1)
- Invitation To Health Canadian 4th Edition Hales Solutions ManualDocument18 pagesInvitation To Health Canadian 4th Edition Hales Solutions ManualJosephGlasswosmr100% (15)
- Communication Skills For Pharmacists.Document153 pagesCommunication Skills For Pharmacists.SalahadinNo ratings yet
- Case Study No.8Document7 pagesCase Study No.8Tahira Zehra0% (1)
- Leukodystrophy Paper August 27thDocument7 pagesLeukodystrophy Paper August 27thZorbey TurkalpNo ratings yet
- Wolcott-Rallison Syndrome: Review Open AccessDocument13 pagesWolcott-Rallison Syndrome: Review Open AccessMazen BarhoushNo ratings yet
- Sdarticle PDFDocument9 pagesSdarticle PDFManjeev GuragainNo ratings yet
- American Academy of Neurology Key PointsDocument193 pagesAmerican Academy of Neurology Key Pointszayat13No ratings yet
- Spinocerebellar AtaxiaDocument22 pagesSpinocerebellar Ataxiatbuyinza21apNo ratings yet
- Juvenile Metachromatic Leucodystrophy A Rare Case ReportDocument2 pagesJuvenile Metachromatic Leucodystrophy A Rare Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Clinical Cases in Pediatric Peripheral NeuropathyDocument23 pagesClinical Cases in Pediatric Peripheral NeuropathyMateen ShukriNo ratings yet
- The Rare and The Unexpected Miller Fisher SyndromeDocument4 pagesThe Rare and The Unexpected Miller Fisher SyndromedoctorebrahimNo ratings yet
- Neuroradiological Findings of Trisomy 13 in A Rare Long-Term SurvivorDocument3 pagesNeuroradiological Findings of Trisomy 13 in A Rare Long-Term Survivorchristian roblesNo ratings yet
- Pascual Child Dystonias Management Review 2006Document8 pagesPascual Child Dystonias Management Review 2006leslyjanetNo ratings yet
- Camargo 2018 (Pathology, Pathophysio, Diagnosis, Symptomps, Treatment)Document6 pagesCamargo 2018 (Pathology, Pathophysio, Diagnosis, Symptomps, Treatment)Rizki Muhammad RanandaNo ratings yet
- A Case of Pervasive Developmental Disorder With Chromosomal Translocation 1-4Document14 pagesA Case of Pervasive Developmental Disorder With Chromosomal Translocation 1-4Agustia Pratiwi AhmadNo ratings yet
- MR Findings in Leigh Syndrome With COX Deficiency and SURF-1 MutationsDocument6 pagesMR Findings in Leigh Syndrome With COX Deficiency and SURF-1 MutationsDrsandy SandyNo ratings yet
- A Magnetic Resonance Approach To Metabolic Disorders in ChildhoodDocument12 pagesA Magnetic Resonance Approach To Metabolic Disorders in ChildhoodAna TelloNo ratings yet
- Johnson 1996Document11 pagesJohnson 1996Ali AmokraneNo ratings yet
- EFNS-guideline ALS PDFDocument22 pagesEFNS-guideline ALS PDFAhmad ShokryNo ratings yet
- Animal Model of EADocument13 pagesAnimal Model of EAzigurat00No ratings yet
- Senior-Loken Syndrome With Rare Manifestations: A Case ReportDocument5 pagesSenior-Loken Syndrome With Rare Manifestations: A Case ReportAndrie GunawanNo ratings yet
- A Sonographic Approach To The Prenatal Diagnosis of Skeletal DysplasiasDocument19 pagesA Sonographic Approach To The Prenatal Diagnosis of Skeletal DysplasiasminhhaiNo ratings yet
- Tolosa-Hunt Syndrome: A Rare Cause For An Isolated Ocular Nerve Palsy in An Elderly MaleDocument3 pagesTolosa-Hunt Syndrome: A Rare Cause For An Isolated Ocular Nerve Palsy in An Elderly MaleElisabeth TikalakaNo ratings yet
- BAAPSDocument147 pagesBAAPSGaurav Patodia100% (1)
- LDM - Bionature 2021-06-03-32Document8 pagesLDM - Bionature 2021-06-03-32JUAN CAMILO GONZALEZ JULIONo ratings yet
- Laporan Tutorial Edit 2Document21 pagesLaporan Tutorial Edit 2Magenda BismaNo ratings yet
- 1 s2.0 S1071909198800077 MainDocument8 pages1 s2.0 S1071909198800077 MainamandaribeirouNo ratings yet
- Spinal Muscular Atrophy: Stephen J. Kolb,, John T. KisselDocument16 pagesSpinal Muscular Atrophy: Stephen J. Kolb,, John T. KisselZouhour MiladiNo ratings yet
- A Rare Case Report On Metachromatic Leukodystrophy Presenting With Regression of MilestoneDocument3 pagesA Rare Case Report On Metachromatic Leukodystrophy Presenting With Regression of MilestoneBIOMEDSCIDIRECT PUBLICATIONSNo ratings yet
- Marfan Syndrome With Atypical PresentationDocument4 pagesMarfan Syndrome With Atypical PresentationaiNo ratings yet
- Enfermedades LisosomalesDocument32 pagesEnfermedades LisosomalesJonathanOmarLaraAcevedoNo ratings yet
- Ehara 1997Document9 pagesEhara 1997jahfdfgsdjad asdhsajhajdkNo ratings yet
- Transient Idiopathic Dystonia Infancy PDF Acta Paediatrica 2011Document4 pagesTransient Idiopathic Dystonia Infancy PDF Acta Paediatrica 2011Ana SopaNo ratings yet
- Total Agenesis of The Corpus Callosum in A Patient With Childhood-Onset SchizophreniaDocument4 pagesTotal Agenesis of The Corpus Callosum in A Patient With Childhood-Onset SchizophreniaBhagyaraj JeevangiNo ratings yet
- Amyotrophic Lateral Sclerosis A.: Excellent History But Was This Copy-Pasted?Document8 pagesAmyotrophic Lateral Sclerosis A.: Excellent History But Was This Copy-Pasted?Allan CastroNo ratings yet
- Alpers' DiseaseDocument5 pagesAlpers' DiseaseDANY PAUL BABYNo ratings yet
- Primary Progressive Apraxia: A Syndrome Difficult To CategorizeDocument2 pagesPrimary Progressive Apraxia: A Syndrome Difficult To CategorizeGuilherme AméricoNo ratings yet
- CUSTODIO Y MONTESINOS 2020 Frontotemporal IMAGENDocument8 pagesCUSTODIO Y MONTESINOS 2020 Frontotemporal IMAGENMAXIMILIANO HEREDIANo ratings yet
- Clínica de La Epilepsia en Los Trastornos Del Espectro AutistaDocument7 pagesClínica de La Epilepsia en Los Trastornos Del Espectro AutistaVanesa RodriguezNo ratings yet
- Noonan Syndrome: Clinical Aspects and Molecular PathogenesisDocument25 pagesNoonan Syndrome: Clinical Aspects and Molecular PathogenesisFlavia ChNo ratings yet
- Lipofuscinosis Neuronal Ceroidea Infantil Tardía. Reporte de Un CasoDocument6 pagesLipofuscinosis Neuronal Ceroidea Infantil Tardía. Reporte de Un Casomauro3022No ratings yet
- Spinal DisDocument32 pagesSpinal DisAkmal Niam FirdausiNo ratings yet
- PDF 01litvanDocument10 pagesPDF 01litvanmartinetti2013No ratings yet
- Deficiencias Iniciales en La Enfermedad de Alzheimer: Tres Ejemplos PrácticosDocument5 pagesDeficiencias Iniciales en La Enfermedad de Alzheimer: Tres Ejemplos PrácticosBM CNo ratings yet
- Case Report: de Morsier Syndrome Associated With Periventricular Nodular HeterotopiaDocument4 pagesCase Report: de Morsier Syndrome Associated With Periventricular Nodular HeterotopiahypnonautNo ratings yet
- 3 10 20 691 PDFDocument2 pages3 10 20 691 PDFVaisnaviNo ratings yet
- Full Text 01Document8 pagesFull Text 01Zunaira AmberNo ratings yet
- Schizophrenia: Overview and Treatment OptionsDocument18 pagesSchizophrenia: Overview and Treatment OptionsMeindayaniNo ratings yet
- Neuroimaging Comparison of Primary Progressive Apraxia of Speech and Progressive Supranuclear PalsyDocument9 pagesNeuroimaging Comparison of Primary Progressive Apraxia of Speech and Progressive Supranuclear PalsyJose Alonso Aguilar ValeraNo ratings yet
- Leighton Et Al 2001. Disordered Breathing During Sleep in Patients With MucopolysaccharidosesDocument12 pagesLeighton Et Al 2001. Disordered Breathing During Sleep in Patients With MucopolysaccharidosesBoNo ratings yet
- Multiple Sistem AtrofiDocument10 pagesMultiple Sistem AtrofiYehuda SimbiakNo ratings yet
- Ataxias EspasticasDocument12 pagesAtaxias EspasticasOsvaldo CortésNo ratings yet
- A Fatal Outcome of A Neonatal Dilated Cardiomyopathy: Evolutive Neonatal Lupus or Earlier Childhood - Onset Systemic Lupus? A Case ReportDocument14 pagesA Fatal Outcome of A Neonatal Dilated Cardiomyopathy: Evolutive Neonatal Lupus or Earlier Childhood - Onset Systemic Lupus? A Case ReportIJAR JOURNALNo ratings yet
- SCAR1Document17 pagesSCAR1ADRIANA DE FREITAS SOUSANo ratings yet
- Dapus Amok 18 PDFDocument18 pagesDapus Amok 18 PDFmuiNo ratings yet
- Cerebral Palsy Sumber AaprmDocument6 pagesCerebral Palsy Sumber AaprmBiandaNo ratings yet
- Myoclonus With DementiaDocument8 pagesMyoclonus With DementiaSantosh DashNo ratings yet
- Clorhidrato de Buspirona en El Tratamiento de La Ataxia CerebelosaDocument5 pagesClorhidrato de Buspirona en El Tratamiento de La Ataxia CerebelosaRenato Byrontt Letelier BernalNo ratings yet
- Cerebral PalsyDocument40 pagesCerebral PalsyStefan ChrisnawanNo ratings yet
- How Alcohol Damages Brain Development in ChildrenDocument14 pagesHow Alcohol Damages Brain Development in ChildrenBenjamin gutierrezNo ratings yet
- Ataxia AcutaDocument17 pagesAtaxia AcutaAlina AndreiNo ratings yet
- 5 Different Type of SyndromeDocument6 pages5 Different Type of SyndromeAdnan RezaNo ratings yet
- Teknik Pemeriksaan IodoterapiDocument8 pagesTeknik Pemeriksaan IodoterapiMike SihombingNo ratings yet
- Resistance of Haemonchus Spp. To Albendazole, Fenbendazole and Levamisole in 4 Goat Farms of Antioquia, ColombiaDocument5 pagesResistance of Haemonchus Spp. To Albendazole, Fenbendazole and Levamisole in 4 Goat Farms of Antioquia, ColombiaMike SihombingNo ratings yet
- Congenital Malformations Associated With Maternal DiabetesDocument7 pagesCongenital Malformations Associated With Maternal DiabetesMike SihombingNo ratings yet
- Aspek Neuroendokrin PubertasDocument38 pagesAspek Neuroendokrin PubertasMike SihombingNo ratings yet
- Reagen Dan Instrumen Pendukung Untuk Laboratorium Pengujian COVID-19Document14 pagesReagen Dan Instrumen Pendukung Untuk Laboratorium Pengujian COVID-19Mike SihombingNo ratings yet
- DIabetesinsipidus TB ARDocument5 pagesDIabetesinsipidus TB ARMike SihombingNo ratings yet
- Hospital Malnutrition in Pediatric Surgery at Dr. Cipto Mangunkusumo General Hospital 2015 and Its Associated FactorsDocument5 pagesHospital Malnutrition in Pediatric Surgery at Dr. Cipto Mangunkusumo General Hospital 2015 and Its Associated FactorsMike SihombingNo ratings yet
- Bedside Pediatric Early Warning SystemDocument38 pagesBedside Pediatric Early Warning SystemMike SihombingNo ratings yet
- 1.10. Follow Up: S Keluhan: BAB Hitam (-), Nyeri Ulu Hati Dan Perut Kanan Atas (-) ODocument8 pages1.10. Follow Up: S Keluhan: BAB Hitam (-), Nyeri Ulu Hati Dan Perut Kanan Atas (-) OMike SihombingNo ratings yet
- Characteristics and Prognosis in Women and Men With Type 1 Diabetes Undergoing Coronary Angiography: A Nationwide Registry ReportDocument8 pagesCharacteristics and Prognosis in Women and Men With Type 1 Diabetes Undergoing Coronary Angiography: A Nationwide Registry ReportMike SihombingNo ratings yet
- Pendekatan Farmakogenomik Dalam Pengembangan Obat Baru: April 2005Document12 pagesPendekatan Farmakogenomik Dalam Pengembangan Obat Baru: April 2005Mike SihombingNo ratings yet
- SFT WFH Girls P 2 5Document4 pagesSFT WFH Girls P 2 5Mike SihombingNo ratings yet
- Occupational English Test Listening Test - 2Document6 pagesOccupational English Test Listening Test - 2Jojelyn Yanez BaliliNo ratings yet
- Mono Bilberry - Oral EnglishDocument5 pagesMono Bilberry - Oral EnglishTom DelongeNo ratings yet
- PPE-25-Case Report of Aquagenic UrticariaDocument2 pagesPPE-25-Case Report of Aquagenic UrticariaSajin AlexanderNo ratings yet
- Canine OA Recognition and ManagementDocument10 pagesCanine OA Recognition and ManagementAngeles MerinoNo ratings yet
- Complications of Orthognathic SurgeryDocument39 pagesComplications of Orthognathic SurgeryAME DENTAL COLLEGE RAICHUR, KARNATAKANo ratings yet
- Case 2Document155 pagesCase 2Jade HemmingsNo ratings yet
- Cilia 2018Document1 pageCilia 2018Anna Beatriz Silva EspindolaNo ratings yet
- DNB Final Theory Papers Ophthalmology 2011 2020Document160 pagesDNB Final Theory Papers Ophthalmology 2011 2020Rekha JakharNo ratings yet
- Eli LillyDocument11 pagesEli LillyvemaNo ratings yet
- From The AcademyDocument13 pagesFrom The AcademySrinivas PingaliNo ratings yet
- Facility-Onset Infections(s) Device-Or Care-Related: Clostridioides DifficileDocument2 pagesFacility-Onset Infections(s) Device-Or Care-Related: Clostridioides DifficileHeba HanyNo ratings yet
- Pathology Chanting 230711 104344Document35 pagesPathology Chanting 230711 104344Smile forever100% (1)
- Product and Company Identification: SIFCO Process Solution Cadmium LHEDocument7 pagesProduct and Company Identification: SIFCO Process Solution Cadmium LHEshaotao guoNo ratings yet
- 7.stool Examination - Morphology of Eggs, Cysts, LarvaeDocument9 pages7.stool Examination - Morphology of Eggs, Cysts, LarvaeKowshik AvulaNo ratings yet
- Safety and Operating Instructions: Trench CompactorDocument40 pagesSafety and Operating Instructions: Trench CompactoralmirNo ratings yet
- Vitiligo A Review 2020 PDFDocument22 pagesVitiligo A Review 2020 PDFhannah khumairahNo ratings yet
- VV 1222 02Document5 pagesVV 1222 02Vy CaoNo ratings yet
- Roxana M. Culcer, M.D., FRACP - Aproach To A Collapsed NeonateDocument32 pagesRoxana M. Culcer, M.D., FRACP - Aproach To A Collapsed Neonatenicu 2021No ratings yet
- Periodontitis y Enfermedad CardiovascularDocument8 pagesPeriodontitis y Enfermedad CardiovascularDafne MendozaNo ratings yet
- Yellow Perils and Hate CrimesDocument21 pagesYellow Perils and Hate CrimesBach ĐứcNo ratings yet
- The World Health Organization A History: April 2019Document25 pagesThe World Health Organization A History: April 2019gkoutzioNo ratings yet
- Nosocomial Infections: Causes, Controls, Preventions and Future ChallengesDocument11 pagesNosocomial Infections: Causes, Controls, Preventions and Future ChallengesAy GlassesNo ratings yet
- Holographic Memory ResolutionDocument4 pagesHolographic Memory ResolutionDarnellNo ratings yet
- Rapidly Establishing A Hospital Based Convalescent Plasma Col - 2021 - AcademicDocument6 pagesRapidly Establishing A Hospital Based Convalescent Plasma Col - 2021 - AcademicdanielwongtsNo ratings yet
- HDU AuditDocument3 pagesHDU AuditAsdf DgfhgNo ratings yet
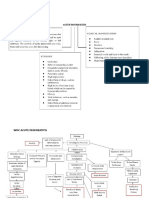
- Woc Acute Pancreatitis EngDocument10 pagesWoc Acute Pancreatitis EngMuhammad Alvin Fuzail IyazNo ratings yet