Download as pdf or txt
You might also like
- IV Therapy Skills ChecklistDocument5 pagesIV Therapy Skills ChecklistnorthweststaffingNo ratings yet
- DR PawandeepKaurSandhuDocument3 pagesDR PawandeepKaurSandhudrgrettagabriellaNo ratings yet
- Management of Edentulous Orofacial DyskinesiaDocument5 pagesManagement of Edentulous Orofacial DyskinesiarindangpaulinaNo ratings yet
- Space Regainers in Pediatric DentistryDocument6 pagesSpace Regainers in Pediatric DentistryDiba Eka DiputriNo ratings yet
- Orthodontic Management of Midline Diastema in Mixed DentitionDocument5 pagesOrthodontic Management of Midline Diastema in Mixed DentitionfatimahNo ratings yet
- Non-Syndromic Multiple Mesiodens: Two Case ReportsDocument3 pagesNon-Syndromic Multiple Mesiodens: Two Case ReportsWilliam YuwonoNo ratings yet
- Space Regainers in Pediatric Dentistry: January 2015Document6 pagesSpace Regainers in Pediatric Dentistry: January 2015Fajar Kusuma Dwi KurniawanNo ratings yet
- ContempClinDent32219 6162101 - 170701 2Document4 pagesContempClinDent32219 6162101 - 170701 2Andres CoboNo ratings yet
- Supernumerary Lateral IncisorDocument2 pagesSupernumerary Lateral IncisorNatasa StojkovicNo ratings yet
- OmyxomaDocument6 pagesOmyxomaClaret TeneNo ratings yet
- Mesiodens-A Case ReportDocument5 pagesMesiodens-A Case ReportfatimahNo ratings yet
- Jurnal KonservasiDocument5 pagesJurnal KonservasiSuciNo ratings yet
- Immediate OverdentureDocument6 pagesImmediate Overdenturerodrigo guiboneNo ratings yet
- Space Regainers in Pediatric DentistryDocument6 pagesSpace Regainers in Pediatric DentistryFayiz SäbNo ratings yet
- Multiple Supernumerary Teeth Associated With An Impacted Maxillary Central Incisor: Surgical and Orthodontic ManagementDocument4 pagesMultiple Supernumerary Teeth Associated With An Impacted Maxillary Central Incisor: Surgical and Orthodontic ManagementCalin CristianNo ratings yet
- Mesiodens A Review and Report of Two CasesDocument3 pagesMesiodens A Review and Report of Two CasesNatasa StojkovicNo ratings yet
- Altering Occlusal Vertical Dimension in FunctionalDocument8 pagesAltering Occlusal Vertical Dimension in FunctionalLorenitta PatiñoNo ratings yet
- Overdenture Abutments Under A Fixed Partial Denture: Case Report of A Preventive Prosthodontic ApproachDocument5 pagesOverdenture Abutments Under A Fixed Partial Denture: Case Report of A Preventive Prosthodontic ApproachFira RizviarNo ratings yet
- Ipdoaj MS Id 000113Document3 pagesIpdoaj MS Id 000113Ayu DamayNo ratings yet
- Orthodontic in Mixed DentitionDocument8 pagesOrthodontic in Mixed Dentitionagnesia tiaraNo ratings yet
- Dent in Al HypersensitivityDocument6 pagesDent in Al HypersensitivityTsafirra AlfarisNo ratings yet
- The Neglected Phase in Orthodontic Diagnosis and TreatmentDocument5 pagesThe Neglected Phase in Orthodontic Diagnosis and TreatmentDr.Prakher SainiNo ratings yet
- Aberrant Impaction of Mandibular Canine and LateraDocument6 pagesAberrant Impaction of Mandibular Canine and LateraGabriella SitinjakNo ratings yet
- 30113-Article Text-56487-1-10-20200530 - 4Document5 pages30113-Article Text-56487-1-10-20200530 - 4felaxis fNo ratings yet
- JurnalDocument9 pagesJurnalNisaNo ratings yet
- Full Mouth Rehabilitation Using Hobo Twin-Stage TechniqueDocument5 pagesFull Mouth Rehabilitation Using Hobo Twin-Stage TechniqueswagataNo ratings yet
- Article - 1653239529 2Document5 pagesArticle - 1653239529 2Mega AzzahraNo ratings yet
- Altering Occlusal Vertical Dimension in FunctionalDocument8 pagesAltering Occlusal Vertical Dimension in FunctionalDavid ColonNo ratings yet
- Abutment Evaluation in FPD 2Document5 pagesAbutment Evaluation in FPD 2ahmad955mlsNo ratings yet
- Vital Pulp Therapy Ies Position StatementDocument30 pagesVital Pulp Therapy Ies Position StatementshivanshaggrohiyaNo ratings yet
- palatogingivalgrooveJIOH PDFDocument6 pagespalatogingivalgrooveJIOH PDFAthulya PallipurathNo ratings yet
- Ortho-Perio Relation: A Review: Deepthi PK, Arun Kumar P, Esther Nalini H, Renuka DeviDocument5 pagesOrtho-Perio Relation: A Review: Deepthi PK, Arun Kumar P, Esther Nalini H, Renuka DeviNeelash KrishnaNo ratings yet
- Immediate Denture A ReviewDocument5 pagesImmediate Denture A ReviewdrfatimahzahraaNo ratings yet
- ISSN 2347-5579: Iatrogenic Dentistry and Periodontal Disease: A Review With Two CasesDocument3 pagesISSN 2347-5579: Iatrogenic Dentistry and Periodontal Disease: A Review With Two CasesVineet ArunNo ratings yet
- Priyanka MakhijaaDocument8 pagesPriyanka MakhijaaAnwesha SamaddarNo ratings yet
- 13 Management of Traumatic Avulsed Permanent Teeth in Childrens Technique Revisited and Literature ReviewDocument10 pages13 Management of Traumatic Avulsed Permanent Teeth in Childrens Technique Revisited and Literature ReviewgeneNo ratings yet
- Orthodontic Treatment: Vital March 2011Document6 pagesOrthodontic Treatment: Vital March 2011Mohammad ArmoutiNo ratings yet
- Management and Sequelae of Intruded Anterior Primary Teeth: A Systematic ReviewDocument12 pagesManagement and Sequelae of Intruded Anterior Primary Teeth: A Systematic ReviewwaydergNo ratings yet
- 2015 DU - Consv Managment of MacrodontiaDocument4 pages2015 DU - Consv Managment of MacrodontiaGeorge JoseNo ratings yet
- Artìculo CareDocument6 pagesArtìculo CareARLET KRISTEL PAMELA REMUZGO ALVARADONo ratings yet
- IJCPDChaitanyaDocument4 pagesIJCPDChaitanyaAliyah SaraswatiNo ratings yet
- Discuss 3Document7 pagesDiscuss 3Zaid DewachiNo ratings yet
- Hemisection As An Alternative Treatment For ResorbDocument3 pagesHemisection As An Alternative Treatment For ResorbRik ChatterjeeNo ratings yet
- Treatment of Mesiondens and Malposition On Class I Malocclusion With Removable Orthodonthic ApplianceDocument3 pagesTreatment of Mesiondens and Malposition On Class I Malocclusion With Removable Orthodonthic ApplianceMega AzzahraNo ratings yet
- Crown Lengthening Vs Forced EruptionDocument4 pagesCrown Lengthening Vs Forced EruptionbarbieNo ratings yet
- Case ReportDocument5 pagesCase ReportWainaianaNo ratings yet
- Restoration of Occlusal Plane and Esthetics in Severely Worn DentitionDocument4 pagesRestoration of Occlusal Plane and Esthetics in Severely Worn DentitionUJ CommunicationNo ratings yet
- Jurnal Kasus Tambahan 3 - Khairin Yonni (12730)Document6 pagesJurnal Kasus Tambahan 3 - Khairin Yonni (12730)Khairin YonniNo ratings yet
- JCDP 19 624Document4 pagesJCDP 19 624Priyanka GandhiNo ratings yet
- Dentigerous CystDocument6 pagesDentigerous CystZahid ManzoorNo ratings yet
- 1 - 150 Ramya Raghu Clinical Operative Dentistry Principles & PracticeDocument150 pages1 - 150 Ramya Raghu Clinical Operative Dentistry Principles & PracticesamikshaNo ratings yet
- Midline Space Closure in The Mixed Dentition - A Case Report PDFDocument3 pagesMidline Space Closure in The Mixed Dentition - A Case Report PDFRirin SupriyaniNo ratings yet
- Prognosis of Teeth in Mandibular Fracture LinesDocument6 pagesPrognosis of Teeth in Mandibular Fracture Lines6hd6mnrzw2No ratings yet
- Jurnal 1Document4 pagesJurnal 1Abdul QaharNo ratings yet
- Immediate Denture A ReviewDocument5 pagesImmediate Denture A ReviewAswathi RaghuthamanNo ratings yet
- Shih 2016Document6 pagesShih 2016fatimahNo ratings yet
- Multiple Unerupted Permanent Teeth Associated With Noonan SyndromeDocument5 pagesMultiple Unerupted Permanent Teeth Associated With Noonan Syndromevighanesh kadamNo ratings yet
- Conservative Endodontics: A Truss Access Case Series: Hussain Mookhtiar, Vivek Hegde, Srilatha S and Meheriar ChopraDocument6 pagesConservative Endodontics: A Truss Access Case Series: Hussain Mookhtiar, Vivek Hegde, Srilatha S and Meheriar Chopralistyana listianaNo ratings yet
- Esthetic Oral Rehabilitation with Veneers: A Guide to Treatment Preparation and Clinical ConceptsFrom EverandEsthetic Oral Rehabilitation with Veneers: A Guide to Treatment Preparation and Clinical ConceptsRichard D. TrushkowskyNo ratings yet
- Study DesignsDocument24 pagesStudy DesignsJasmen Sabroso PasiaNo ratings yet
- Nursing Management in Cancer CareDocument27 pagesNursing Management in Cancer CareFev BanataoNo ratings yet
- HOBERMAN 2005 Testosterone Dreams PDFDocument390 pagesHOBERMAN 2005 Testosterone Dreams PDFLucasTramontanoNo ratings yet
- Enter and Leave The Workplace Using Proper RoutesDocument2 pagesEnter and Leave The Workplace Using Proper RoutesAubz Almelia NavarroNo ratings yet
- Pharmacokinetic Models NotesDocument32 pagesPharmacokinetic Models Notes슬기.No ratings yet
- Journal Club 3: Systematic ReviewsDocument4 pagesJournal Club 3: Systematic ReviewsSpeech & Language Therapy in PracticeNo ratings yet
- The Abbey Pain Scale For Assessment of Pain in Patients Who Cannot Verbalise I.E. Patients With Dementia or Communication DifficultiesDocument3 pagesThe Abbey Pain Scale For Assessment of Pain in Patients Who Cannot Verbalise I.E. Patients With Dementia or Communication DifficultiesTas JadeNo ratings yet
- Individual Canine Retraction Using Modified Segmental MechanicsDocument4 pagesIndividual Canine Retraction Using Modified Segmental MechanicsAkhil SinghNo ratings yet
- "The Tao of Rejuvenation" Interview With Angelo DrudaDocument9 pages"The Tao of Rejuvenation" Interview With Angelo DrudagaryscottmorrowNo ratings yet
- Public Health Education For Medical StudentsDocument20 pagesPublic Health Education For Medical StudentsOm AbdalrahmanNo ratings yet
- Action Taken Report PHC - KALLUMARRIDocument2 pagesAction Taken Report PHC - KALLUMARRIphc kallumarriNo ratings yet
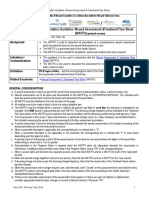
- Documentation Guideline: Wound Assessment &treatment Flow Sheet (Watfs)Document4 pagesDocumentation Guideline: Wound Assessment &treatment Flow Sheet (Watfs)eva arna abrarNo ratings yet
- Procedures CompilationDocument51 pagesProcedures CompilationNiña Jean Tormis Aldaba100% (1)
- Assignment Systems For StaffingDocument10 pagesAssignment Systems For StaffingfatmaabedNo ratings yet
- Vaccination Complete CertDocument1 pageVaccination Complete CertGiri BabuNo ratings yet
- Tuberculosis VaccineDocument15 pagesTuberculosis Vaccinesatheeshpharma6No ratings yet
- Philippine Health Insurance Corporation: Citystatc Centre. 709 Shaw Boulevard, Pasig City /n/w.philhcalth.e.m .PHDocument72 pagesPhilippine Health Insurance Corporation: Citystatc Centre. 709 Shaw Boulevard, Pasig City /n/w.philhcalth.e.m .PHToche DoceNo ratings yet
- What You MUST Know About PlacentaDocument2 pagesWhat You MUST Know About Placenta林雯No ratings yet
- Clonazepam AJPDocument4 pagesClonazepam AJPDian GbligNo ratings yet
- POINTERSDocument49 pagesPOINTERSJonas Marvin AnaqueNo ratings yet
- Medication Deferral ListDocument2 pagesMedication Deferral ListKwiila KaoNo ratings yet
- Clinical GoalsDocument13 pagesClinical GoalsHycient PaulNo ratings yet
- Blue and Green Self-Quarantine Guidelines Coronavirus PosterDocument1 pageBlue and Green Self-Quarantine Guidelines Coronavirus Postersara cadavid jimenezNo ratings yet
- A Novel Clinical Grading Scale To Guide The Management of Crusted ScabiesDocument6 pagesA Novel Clinical Grading Scale To Guide The Management of Crusted ScabiesFelisiana KasmanNo ratings yet
- Ineffective Health Management Related To Mrs. Gama: Provide The Client Enough Knowledge About The ProblemDocument5 pagesIneffective Health Management Related To Mrs. Gama: Provide The Client Enough Knowledge About The ProblemAndrea Albester GarinoNo ratings yet
- Universidad Puerto Rico Manual 1415Document161 pagesUniversidad Puerto Rico Manual 1415Roberto RamosNo ratings yet
- Summary - Ocular Manifestations of HIVDocument1 pageSummary - Ocular Manifestations of HIVRyan HumeNo ratings yet
- Threatened AbortionDocument1 pageThreatened AbortionTrisha SuazoNo ratings yet
- Announcement Chest 2019Document4 pagesAnnouncement Chest 2019febyan yohanesNo ratings yet