
Status Epilepticus: Refractory and Super Refractory: Review Article
Status Epilepticus: Refractory and Super Refractory: Review Article
You might also like
- Misra U, Kalita J Dan Dubey D. A Study of Super Refractory Status Epilepticus From IndiaDocument10 pagesMisra U, Kalita J Dan Dubey D. A Study of Super Refractory Status Epilepticus From IndiasitialimahNo ratings yet
- Status EpilepticusDocument22 pagesStatus EpilepticusYohanes MarulituaNo ratings yet
- Intensive Care Management of Status EpilepticusDocument13 pagesIntensive Care Management of Status EpilepticusMaria DronNo ratings yet
- Oto Et Al 2011 Effect of Daily Sedative Interruption on Sleep Stages of Mechanically Ventilated Patients ReceivingDocument9 pagesOto Et Al 2011 Effect of Daily Sedative Interruption on Sleep Stages of Mechanically Ventilated Patients ReceivingSanday EngNo ratings yet
- TreatmentofStatusEpilepticus PDFDocument14 pagesTreatmentofStatusEpilepticus PDFAnonymous 7wo4ZBVaEvNo ratings yet
- Status EpilepticusDocument13 pagesStatus EpilepticusChandra EkaNo ratings yet
- 07 October 2021 Status Epilepticus Short Journal Article Stetefeld2021 - Article - IsofluraneInSuper-RefractoryStDocument9 pages07 October 2021 Status Epilepticus Short Journal Article Stetefeld2021 - Article - IsofluraneInSuper-RefractoryStMarkhum GoundenNo ratings yet
- Sleep Deprivation in Intensive Care Unit - Systematic ReviewDocument10 pagesSleep Deprivation in Intensive Care Unit - Systematic Reviewwazirsaid39No ratings yet
- Sedatives in Neurocritical Care 2019 Curr Opin Crit CareDocument8 pagesSedatives in Neurocritical Care 2019 Curr Opin Crit CareCAMILO ERNESTO DAZA PERDOMONo ratings yet
- Excessive Daytime Sleepiness and Epilepsy A SystemDocument10 pagesExcessive Daytime Sleepiness and Epilepsy A Systemkano bhavNo ratings yet
- Convulsive Status Epilepticus Management in Adults and Children: of The Working Group of The Polish Society of EpileptologyDocument8 pagesConvulsive Status Epilepticus Management in Adults and Children: of The Working Group of The Polish Society of Epileptologymoy9616No ratings yet
- Status Epilepticus in The ICU: ReviewDocument16 pagesStatus Epilepticus in The ICU: ReviewRotsen Alessandra Tapia VelazcoNo ratings yet
- Bravo 2021Document22 pagesBravo 2021Ivan MihailovicNo ratings yet
- Super Refractory Status Epilepticus in AdultsDocument7 pagesSuper Refractory Status Epilepticus in AdultsCarlos alvarezNo ratings yet
- Evaluation and Management of Seizures and Status EpilepticusDocument32 pagesEvaluation and Management of Seizures and Status Epilepticusmorena19932308No ratings yet
- Antidepressants For The Treatment of NarcolepsyDocument5 pagesAntidepressants For The Treatment of NarcolepsyMOHAMAD FAKIHNo ratings yet
- EEG Endpoints IV Treatment For RSE and SRSE 2020Document12 pagesEEG Endpoints IV Treatment For RSE and SRSE 2020luigi.pietro.carlo.undaNo ratings yet
- Efficient Epileptic Seizure Prediction Based On Deep LearningDocument10 pagesEfficient Epileptic Seizure Prediction Based On Deep LearningJoan Sebastian Betancourt AriasNo ratings yet
- Estimulador de Nervio Vago para Epilepsia Refractaria en NiñosDocument11 pagesEstimulador de Nervio Vago para Epilepsia Refractaria en NiñosArbey Aponte PuertoNo ratings yet
- Cureus 0011 00000005485Document6 pagesCureus 0011 00000005485Koko The good boyNo ratings yet
- Current Treatment of Convulsive Status Epilepticus - A Therapeutic Protocol and ReviewDocument11 pagesCurrent Treatment of Convulsive Status Epilepticus - A Therapeutic Protocol and ReviewIndra Budi PutraNo ratings yet
- Dita 1Document8 pagesDita 1Jannah Miftahul JannahNo ratings yet
- Pediatric Refractory and Super Refractory ReviewDocument10 pagesPediatric Refractory and Super Refractory ReviewFlavia Angelina SatopohNo ratings yet
- Sleep Disturbance and Nonmalignant Chronic PainDocument17 pagesSleep Disturbance and Nonmalignant Chronic Painveigaarthur84No ratings yet
- Acute Disseminated Encephalomyelitis After Rabies Vaccination: One Case ReportDocument4 pagesAcute Disseminated Encephalomyelitis After Rabies Vaccination: One Case ReportIJAR JOURNALNo ratings yet
- Kwon Et Al 2023 Epicranial Headache Part 1 Primary Stabbing HeadacheDocument11 pagesKwon Et Al 2023 Epicranial Headache Part 1 Primary Stabbing HeadacheErick HernandezNo ratings yet
- Henry C Skrehot Neuro Stimulation in Focal Epilepsy ADocument10 pagesHenry C Skrehot Neuro Stimulation in Focal Epilepsy AArbey Aponte PuertoNo ratings yet
- Fernandez Gonzalo2017Document15 pagesFernandez Gonzalo2017Vlady78No ratings yet
- Neuroestimulación para EpilepsiaDocument7 pagesNeuroestimulación para EpilepsiaArbey Aponte PuertoNo ratings yet
- Medicine: Risk Factors For Drug-Resistant EpilepsyDocument12 pagesMedicine: Risk Factors For Drug-Resistant EpilepsyyutomoNo ratings yet
- Are We Prepared To Detect Subtle and Nonconvulsive Status Epilepticus in Critically Ill Patients?Document7 pagesAre We Prepared To Detect Subtle and Nonconvulsive Status Epilepticus in Critically Ill Patients?succa07No ratings yet
- Frequency and Evolution of Sleep Disorders StrokeDocument8 pagesFrequency and Evolution of Sleep Disorders Stroke170211201076No ratings yet
- Apm 22145Document12 pagesApm 22145dramaholic842No ratings yet
- Status Epileptico Anestesia 2022Document15 pagesStatus Epileptico Anestesia 2022Azucena RiosNo ratings yet
- Medi 97 E10919Document4 pagesMedi 97 E10919oktaviaNo ratings yet
- Status Epilepticus Optimal Management Recent Advances 2022Document16 pagesStatus Epilepticus Optimal Management Recent Advances 2022francklinmp.2022No ratings yet
- Fisiopatología EstatusDocument14 pagesFisiopatología EstatusDaniel LeivaNo ratings yet
- Crise Convulsiva Provocada - ManejoDocument11 pagesCrise Convulsiva Provocada - Manejorafael rocha novaesNo ratings yet
- Therapeutic Advances in Dravet Syndrome A Targeted Literature Review - CompressedDocument16 pagesTherapeutic Advances in Dravet Syndrome A Targeted Literature Review - CompressedfthaytcNo ratings yet
- 01-Van RijckevorselDocument8 pages01-Van Rijckevorseljoaojoaomendes6846No ratings yet
- Status Epilepticus: Correspondence: Hpg9v@virginia - EduDocument12 pagesStatus Epilepticus: Correspondence: Hpg9v@virginia - EduGerardo Lerma BurciagaNo ratings yet
- Seizure: Eugen Trinka, Reetta KälviäinenDocument9 pagesSeizure: Eugen Trinka, Reetta KälviäinenAaron Nureña JaraNo ratings yet
- Estatus Epileptico EmergencyDocument13 pagesEstatus Epileptico EmergencytorresjairrNo ratings yet
- Fneur 14 1175370Document10 pagesFneur 14 1175370WenSarmientoBNo ratings yet
- Fisiopatologia de MigrañaDocument25 pagesFisiopatologia de MigrañaJorge ZegarraNo ratings yet
- HHS Public Access: Impact of Sleep Disturbances On Neurodegeneration: Insight From Studies in Animal ModelsDocument25 pagesHHS Public Access: Impact of Sleep Disturbances On Neurodegeneration: Insight From Studies in Animal ModelsPawan MishraNo ratings yet
- Hingray 2016Document7 pagesHingray 2016syrieuxNo ratings yet
- Sleep Architectural Dysfunction and Undiagnosed Obstructive SleepDocument9 pagesSleep Architectural Dysfunction and Undiagnosed Obstructive Sleepluigi.pietro.carlo.undaNo ratings yet
- Epilepsia - 2018 - Hocker - Anesthetic Drugs For The Treatment of Status EpilepticusDocument5 pagesEpilepsia - 2018 - Hocker - Anesthetic Drugs For The Treatment of Status EpilepticusKikie Rizky HeningNo ratings yet
- Physiotherapy Interventions For A Traumatic Brain Injury Patient: A Case StudyDocument5 pagesPhysiotherapy Interventions For A Traumatic Brain Injury Patient: A Case StudymunaazizahNo ratings yet
- 30 Years of Vagus NerveDocument5 pages30 Years of Vagus NerveErnesto Ochoa MonroyNo ratings yet
- Diagnostic Procedureand Therapeutic Approachesin Nonconvulsive Status Epilepticus NCSEDocument6 pagesDiagnostic Procedureand Therapeutic Approachesin Nonconvulsive Status Epilepticus NCSEIvan MihailovicNo ratings yet
- Sedation in The Intensive Care Unit: Katherine Rowe MBCHB MRCP Frca Simon Fletcher Mbbs Frca FrcpeDocument6 pagesSedation in The Intensive Care Unit: Katherine Rowe MBCHB MRCP Frca Simon Fletcher Mbbs Frca FrcpeMohammed IrfanNo ratings yet
- Kelompok 2Document23 pagesKelompok 2lutfiah nabilahNo ratings yet
- Diagnosing Patients With Acute-Onset Persistent DizzinessDocument7 pagesDiagnosing Patients With Acute-Onset Persistent DizzinessMuhammed ElgasimNo ratings yet
- RCCM 200204-270ccDocument5 pagesRCCM 200204-270ccJunior BarretoNo ratings yet
- Pain Practice - 2010 - Van Eijs - 16 Complex Regional Pain SyndromeDocument18 pagesPain Practice - 2010 - Van Eijs - 16 Complex Regional Pain SyndromeZuraidaNo ratings yet
- 2021 Posterior Reversible Encephalopathy Syndrome (PRES) Diagnosis and ManagementDocument9 pages2021 Posterior Reversible Encephalopathy Syndrome (PRES) Diagnosis and ManagementSafitri MuhlisaNo ratings yet
- So 2010Document10 pagesSo 2010Pablo Sebastián SaezNo ratings yet
- Cme Invite PDFDocument1 pageCme Invite PDFsandeep reddyNo ratings yet
- ReportDocument1 pageReportsandeep reddyNo ratings yet
- BSE Limited Code: 532321: Dhaval Narendra SoniDocument3 pagesBSE Limited Code: 532321: Dhaval Narendra Sonisandeep reddyNo ratings yet
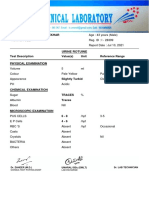
- Urine Rotuine: Test Description Value(s) Unit Reference Range Physical ExaminationDocument5 pagesUrine Rotuine: Test Description Value(s) Unit Reference Range Physical Examinationsandeep reddyNo ratings yet
- Nihal Reddy CAHW-0000298026 M / 8M 23D Dr. Otclab - OeDocument25 pagesNihal Reddy CAHW-0000298026 M / 8M 23D Dr. Otclab - Oesandeep reddyNo ratings yet
- Are Atropic.: Ref. by Dr. R. Rajeshwari Abdomino - Pelvic ScanDocument2 pagesAre Atropic.: Ref. by Dr. R. Rajeshwari Abdomino - Pelvic Scansandeep reddyNo ratings yet
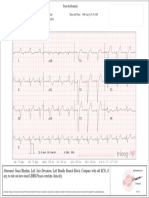
- Ecg Report of MagalammaDocument3 pagesEcg Report of Magalammasandeep reddyNo ratings yet
- Approach To SeizuresDocument60 pagesApproach To SeizuresHerrera MiguelNo ratings yet
- Nejmoa 2008663Document10 pagesNejmoa 2008663emmyNo ratings yet
- Epilepsy IN Children: Presented by DR - Meera Pramil Department of KaumarabhrityaDocument60 pagesEpilepsy IN Children: Presented by DR - Meera Pramil Department of KaumarabhrityaAnil DasNo ratings yet
- MS - NeuroDocument10 pagesMS - Neuroknowamai567No ratings yet
- Product and Regulatory Guide, Limited Warranty & AgreementDocument88 pagesProduct and Regulatory Guide, Limited Warranty & AgreementJosé Roberto onichanNo ratings yet
- Civ Vi Exp Online Manual EngDocument42 pagesCiv Vi Exp Online Manual Englollo.cerasa778No ratings yet
- Epilepsy in SportsDocument43 pagesEpilepsy in SportsMpt SportsNo ratings yet
- Manual GTR2Document39 pagesManual GTR2Four UnlimitedNo ratings yet
- NCP - Risk For InjuryDocument3 pagesNCP - Risk For InjuryMatty JolbitadoNo ratings yet
- National Epilepsy Consensus Guideline Society of Neurologists of Bangladesh 1Document130 pagesNational Epilepsy Consensus Guideline Society of Neurologists of Bangladesh 1Kutu MiaNo ratings yet
- The Ukfpo Clinical Assessment Examination Guide by Sarishka Singh Plab ResourcesDocument112 pagesThe Ukfpo Clinical Assessment Examination Guide by Sarishka Singh Plab ResourcesWonjoo LeeNo ratings yet
- Seizures in Children PiR2020Document29 pagesSeizures in Children PiR2020Majo EscobarNo ratings yet
- Status Triphasicus Vs Status EpilepticusDocument8 pagesStatus Triphasicus Vs Status EpilepticusZaida RojasNo ratings yet
- What Is A Physical Disability?: Spinal Cord Injury (SCI)Document14 pagesWhat Is A Physical Disability?: Spinal Cord Injury (SCI)XIARESSE DELA CRUZNo ratings yet
- SONY PSP - Instruction ManualDocument268 pagesSONY PSP - Instruction ManualKelvin KoNo ratings yet
- Local Media2948704747634099528Document99 pagesLocal Media2948704747634099528Sufina Ann GalitNo ratings yet
- Tim Burtons The Nightmare Before Christmas - Oogies Revenge - Manual - XBXDocument11 pagesTim Burtons The Nightmare Before Christmas - Oogies Revenge - Manual - XBXSergio MariNo ratings yet
- Epilepsy SyndromesDocument13 pagesEpilepsy SyndromestoyyibNo ratings yet
- ASM Pharmacology and Clinical Efficacy 2021 PDFDocument29 pagesASM Pharmacology and Clinical Efficacy 2021 PDFIchrak GhachemNo ratings yet
- Randomized Trial of Three Anticonvulsant Medications For Status EpilepticusDocument18 pagesRandomized Trial of Three Anticonvulsant Medications For Status EpilepticusBaiq Widaning Dwi AnjaniNo ratings yet
- World of Tanks Game Manual en Eu Web 9 0 1Document95 pagesWorld of Tanks Game Manual en Eu Web 9 0 1Catarig IoanNo ratings yet
- Roxiva RX1 User GuideDocument17 pagesRoxiva RX1 User GuideYaself BeatsNo ratings yet
- Wessex Neuro ICU GuidelinesDocument200 pagesWessex Neuro ICU GuidelinesJVSP Servicos Medicos LTDANo ratings yet
- Medical Surgical Nursing ReviewDocument97 pagesMedical Surgical Nursing ReviewBernadeth Josefa BorelaNo ratings yet
- Helen's Story EBookFINALDocument19 pagesHelen's Story EBookFINALGMDMNo ratings yet
- Dita 1Document8 pagesDita 1Jannah Miftahul JannahNo ratings yet
- CHCDIS007 STUDENT WORKBOOK (WORD) - C4A.v1.1Document86 pagesCHCDIS007 STUDENT WORKBOOK (WORD) - C4A.v1.1shrestha31dristi100% (2)
- War and Peace - Manual - PCDocument21 pagesWar and Peace - Manual - PCmab58No ratings yet
- Fasting Article Health Benefits 21dayDocument12 pagesFasting Article Health Benefits 21dayJosh BassNo ratings yet
- First Aid (Loss of Consciouness and Seizure) : Presentor: Nomer M. FerrerDocument7 pagesFirst Aid (Loss of Consciouness and Seizure) : Presentor: Nomer M. FerrerLuna CapitNo ratings yet


























































































Download as pdf or txt
You might also like
- Misra U, Kalita J Dan Dubey D. A Study of Super Refractory Status Epilepticus From IndiaDocument10 pagesMisra U, Kalita J Dan Dubey D. A Study of Super Refractory Status Epilepticus From IndiasitialimahNo ratings yet
- Status EpilepticusDocument22 pagesStatus EpilepticusYohanes MarulituaNo ratings yet
- Intensive Care Management of Status EpilepticusDocument13 pagesIntensive Care Management of Status EpilepticusMaria DronNo ratings yet
- Oto Et Al 2011 Effect of Daily Sedative Interruption on Sleep Stages of Mechanically Ventilated Patients ReceivingDocument9 pagesOto Et Al 2011 Effect of Daily Sedative Interruption on Sleep Stages of Mechanically Ventilated Patients ReceivingSanday EngNo ratings yet
- TreatmentofStatusEpilepticus PDFDocument14 pagesTreatmentofStatusEpilepticus PDFAnonymous 7wo4ZBVaEvNo ratings yet
- Status EpilepticusDocument13 pagesStatus EpilepticusChandra EkaNo ratings yet
- 07 October 2021 Status Epilepticus Short Journal Article Stetefeld2021 - Article - IsofluraneInSuper-RefractoryStDocument9 pages07 October 2021 Status Epilepticus Short Journal Article Stetefeld2021 - Article - IsofluraneInSuper-RefractoryStMarkhum GoundenNo ratings yet
- Sleep Deprivation in Intensive Care Unit - Systematic ReviewDocument10 pagesSleep Deprivation in Intensive Care Unit - Systematic Reviewwazirsaid39No ratings yet
- Sedatives in Neurocritical Care 2019 Curr Opin Crit CareDocument8 pagesSedatives in Neurocritical Care 2019 Curr Opin Crit CareCAMILO ERNESTO DAZA PERDOMONo ratings yet
- Excessive Daytime Sleepiness and Epilepsy A SystemDocument10 pagesExcessive Daytime Sleepiness and Epilepsy A Systemkano bhavNo ratings yet
- Convulsive Status Epilepticus Management in Adults and Children: of The Working Group of The Polish Society of EpileptologyDocument8 pagesConvulsive Status Epilepticus Management in Adults and Children: of The Working Group of The Polish Society of Epileptologymoy9616No ratings yet
- Status Epilepticus in The ICU: ReviewDocument16 pagesStatus Epilepticus in The ICU: ReviewRotsen Alessandra Tapia VelazcoNo ratings yet
- Bravo 2021Document22 pagesBravo 2021Ivan MihailovicNo ratings yet
- Super Refractory Status Epilepticus in AdultsDocument7 pagesSuper Refractory Status Epilepticus in AdultsCarlos alvarezNo ratings yet
- Evaluation and Management of Seizures and Status EpilepticusDocument32 pagesEvaluation and Management of Seizures and Status Epilepticusmorena19932308No ratings yet
- Antidepressants For The Treatment of NarcolepsyDocument5 pagesAntidepressants For The Treatment of NarcolepsyMOHAMAD FAKIHNo ratings yet
- EEG Endpoints IV Treatment For RSE and SRSE 2020Document12 pagesEEG Endpoints IV Treatment For RSE and SRSE 2020luigi.pietro.carlo.undaNo ratings yet
- Efficient Epileptic Seizure Prediction Based On Deep LearningDocument10 pagesEfficient Epileptic Seizure Prediction Based On Deep LearningJoan Sebastian Betancourt AriasNo ratings yet
- Estimulador de Nervio Vago para Epilepsia Refractaria en NiñosDocument11 pagesEstimulador de Nervio Vago para Epilepsia Refractaria en NiñosArbey Aponte PuertoNo ratings yet
- Cureus 0011 00000005485Document6 pagesCureus 0011 00000005485Koko The good boyNo ratings yet
- Current Treatment of Convulsive Status Epilepticus - A Therapeutic Protocol and ReviewDocument11 pagesCurrent Treatment of Convulsive Status Epilepticus - A Therapeutic Protocol and ReviewIndra Budi PutraNo ratings yet
- Dita 1Document8 pagesDita 1Jannah Miftahul JannahNo ratings yet
- Pediatric Refractory and Super Refractory ReviewDocument10 pagesPediatric Refractory and Super Refractory ReviewFlavia Angelina SatopohNo ratings yet
- Sleep Disturbance and Nonmalignant Chronic PainDocument17 pagesSleep Disturbance and Nonmalignant Chronic Painveigaarthur84No ratings yet
- Acute Disseminated Encephalomyelitis After Rabies Vaccination: One Case ReportDocument4 pagesAcute Disseminated Encephalomyelitis After Rabies Vaccination: One Case ReportIJAR JOURNALNo ratings yet
- Kwon Et Al 2023 Epicranial Headache Part 1 Primary Stabbing HeadacheDocument11 pagesKwon Et Al 2023 Epicranial Headache Part 1 Primary Stabbing HeadacheErick HernandezNo ratings yet
- Henry C Skrehot Neuro Stimulation in Focal Epilepsy ADocument10 pagesHenry C Skrehot Neuro Stimulation in Focal Epilepsy AArbey Aponte PuertoNo ratings yet
- Fernandez Gonzalo2017Document15 pagesFernandez Gonzalo2017Vlady78No ratings yet
- Neuroestimulación para EpilepsiaDocument7 pagesNeuroestimulación para EpilepsiaArbey Aponte PuertoNo ratings yet
- Medicine: Risk Factors For Drug-Resistant EpilepsyDocument12 pagesMedicine: Risk Factors For Drug-Resistant EpilepsyyutomoNo ratings yet
- Are We Prepared To Detect Subtle and Nonconvulsive Status Epilepticus in Critically Ill Patients?Document7 pagesAre We Prepared To Detect Subtle and Nonconvulsive Status Epilepticus in Critically Ill Patients?succa07No ratings yet
- Frequency and Evolution of Sleep Disorders StrokeDocument8 pagesFrequency and Evolution of Sleep Disorders Stroke170211201076No ratings yet
- Apm 22145Document12 pagesApm 22145dramaholic842No ratings yet
- Status Epileptico Anestesia 2022Document15 pagesStatus Epileptico Anestesia 2022Azucena RiosNo ratings yet
- Medi 97 E10919Document4 pagesMedi 97 E10919oktaviaNo ratings yet
- Status Epilepticus Optimal Management Recent Advances 2022Document16 pagesStatus Epilepticus Optimal Management Recent Advances 2022francklinmp.2022No ratings yet
- Fisiopatología EstatusDocument14 pagesFisiopatología EstatusDaniel LeivaNo ratings yet
- Crise Convulsiva Provocada - ManejoDocument11 pagesCrise Convulsiva Provocada - Manejorafael rocha novaesNo ratings yet
- Therapeutic Advances in Dravet Syndrome A Targeted Literature Review - CompressedDocument16 pagesTherapeutic Advances in Dravet Syndrome A Targeted Literature Review - CompressedfthaytcNo ratings yet
- 01-Van RijckevorselDocument8 pages01-Van Rijckevorseljoaojoaomendes6846No ratings yet
- Status Epilepticus: Correspondence: Hpg9v@virginia - EduDocument12 pagesStatus Epilepticus: Correspondence: Hpg9v@virginia - EduGerardo Lerma BurciagaNo ratings yet
- Seizure: Eugen Trinka, Reetta KälviäinenDocument9 pagesSeizure: Eugen Trinka, Reetta KälviäinenAaron Nureña JaraNo ratings yet
- Estatus Epileptico EmergencyDocument13 pagesEstatus Epileptico EmergencytorresjairrNo ratings yet
- Fneur 14 1175370Document10 pagesFneur 14 1175370WenSarmientoBNo ratings yet
- Fisiopatologia de MigrañaDocument25 pagesFisiopatologia de MigrañaJorge ZegarraNo ratings yet
- HHS Public Access: Impact of Sleep Disturbances On Neurodegeneration: Insight From Studies in Animal ModelsDocument25 pagesHHS Public Access: Impact of Sleep Disturbances On Neurodegeneration: Insight From Studies in Animal ModelsPawan MishraNo ratings yet
- Hingray 2016Document7 pagesHingray 2016syrieuxNo ratings yet
- Sleep Architectural Dysfunction and Undiagnosed Obstructive SleepDocument9 pagesSleep Architectural Dysfunction and Undiagnosed Obstructive Sleepluigi.pietro.carlo.undaNo ratings yet
- Epilepsia - 2018 - Hocker - Anesthetic Drugs For The Treatment of Status EpilepticusDocument5 pagesEpilepsia - 2018 - Hocker - Anesthetic Drugs For The Treatment of Status EpilepticusKikie Rizky HeningNo ratings yet
- Physiotherapy Interventions For A Traumatic Brain Injury Patient: A Case StudyDocument5 pagesPhysiotherapy Interventions For A Traumatic Brain Injury Patient: A Case StudymunaazizahNo ratings yet
- 30 Years of Vagus NerveDocument5 pages30 Years of Vagus NerveErnesto Ochoa MonroyNo ratings yet
- Diagnostic Procedureand Therapeutic Approachesin Nonconvulsive Status Epilepticus NCSEDocument6 pagesDiagnostic Procedureand Therapeutic Approachesin Nonconvulsive Status Epilepticus NCSEIvan MihailovicNo ratings yet
- Sedation in The Intensive Care Unit: Katherine Rowe MBCHB MRCP Frca Simon Fletcher Mbbs Frca FrcpeDocument6 pagesSedation in The Intensive Care Unit: Katherine Rowe MBCHB MRCP Frca Simon Fletcher Mbbs Frca FrcpeMohammed IrfanNo ratings yet
- Kelompok 2Document23 pagesKelompok 2lutfiah nabilahNo ratings yet
- Diagnosing Patients With Acute-Onset Persistent DizzinessDocument7 pagesDiagnosing Patients With Acute-Onset Persistent DizzinessMuhammed ElgasimNo ratings yet
- RCCM 200204-270ccDocument5 pagesRCCM 200204-270ccJunior BarretoNo ratings yet
- Pain Practice - 2010 - Van Eijs - 16 Complex Regional Pain SyndromeDocument18 pagesPain Practice - 2010 - Van Eijs - 16 Complex Regional Pain SyndromeZuraidaNo ratings yet
- 2021 Posterior Reversible Encephalopathy Syndrome (PRES) Diagnosis and ManagementDocument9 pages2021 Posterior Reversible Encephalopathy Syndrome (PRES) Diagnosis and ManagementSafitri MuhlisaNo ratings yet
- So 2010Document10 pagesSo 2010Pablo Sebastián SaezNo ratings yet
- Cme Invite PDFDocument1 pageCme Invite PDFsandeep reddyNo ratings yet
- ReportDocument1 pageReportsandeep reddyNo ratings yet
- BSE Limited Code: 532321: Dhaval Narendra SoniDocument3 pagesBSE Limited Code: 532321: Dhaval Narendra Sonisandeep reddyNo ratings yet
- Urine Rotuine: Test Description Value(s) Unit Reference Range Physical ExaminationDocument5 pagesUrine Rotuine: Test Description Value(s) Unit Reference Range Physical Examinationsandeep reddyNo ratings yet
- Nihal Reddy CAHW-0000298026 M / 8M 23D Dr. Otclab - OeDocument25 pagesNihal Reddy CAHW-0000298026 M / 8M 23D Dr. Otclab - Oesandeep reddyNo ratings yet
- Are Atropic.: Ref. by Dr. R. Rajeshwari Abdomino - Pelvic ScanDocument2 pagesAre Atropic.: Ref. by Dr. R. Rajeshwari Abdomino - Pelvic Scansandeep reddyNo ratings yet
- Ecg Report of MagalammaDocument3 pagesEcg Report of Magalammasandeep reddyNo ratings yet
- Approach To SeizuresDocument60 pagesApproach To SeizuresHerrera MiguelNo ratings yet
- Nejmoa 2008663Document10 pagesNejmoa 2008663emmyNo ratings yet
- Epilepsy IN Children: Presented by DR - Meera Pramil Department of KaumarabhrityaDocument60 pagesEpilepsy IN Children: Presented by DR - Meera Pramil Department of KaumarabhrityaAnil DasNo ratings yet
- MS - NeuroDocument10 pagesMS - Neuroknowamai567No ratings yet
- Product and Regulatory Guide, Limited Warranty & AgreementDocument88 pagesProduct and Regulatory Guide, Limited Warranty & AgreementJosé Roberto onichanNo ratings yet
- Civ Vi Exp Online Manual EngDocument42 pagesCiv Vi Exp Online Manual Englollo.cerasa778No ratings yet
- Epilepsy in SportsDocument43 pagesEpilepsy in SportsMpt SportsNo ratings yet
- Manual GTR2Document39 pagesManual GTR2Four UnlimitedNo ratings yet
- NCP - Risk For InjuryDocument3 pagesNCP - Risk For InjuryMatty JolbitadoNo ratings yet
- National Epilepsy Consensus Guideline Society of Neurologists of Bangladesh 1Document130 pagesNational Epilepsy Consensus Guideline Society of Neurologists of Bangladesh 1Kutu MiaNo ratings yet
- The Ukfpo Clinical Assessment Examination Guide by Sarishka Singh Plab ResourcesDocument112 pagesThe Ukfpo Clinical Assessment Examination Guide by Sarishka Singh Plab ResourcesWonjoo LeeNo ratings yet
- Seizures in Children PiR2020Document29 pagesSeizures in Children PiR2020Majo EscobarNo ratings yet
- Status Triphasicus Vs Status EpilepticusDocument8 pagesStatus Triphasicus Vs Status EpilepticusZaida RojasNo ratings yet
- What Is A Physical Disability?: Spinal Cord Injury (SCI)Document14 pagesWhat Is A Physical Disability?: Spinal Cord Injury (SCI)XIARESSE DELA CRUZNo ratings yet
- SONY PSP - Instruction ManualDocument268 pagesSONY PSP - Instruction ManualKelvin KoNo ratings yet
- Local Media2948704747634099528Document99 pagesLocal Media2948704747634099528Sufina Ann GalitNo ratings yet
- Tim Burtons The Nightmare Before Christmas - Oogies Revenge - Manual - XBXDocument11 pagesTim Burtons The Nightmare Before Christmas - Oogies Revenge - Manual - XBXSergio MariNo ratings yet
- Epilepsy SyndromesDocument13 pagesEpilepsy SyndromestoyyibNo ratings yet
- ASM Pharmacology and Clinical Efficacy 2021 PDFDocument29 pagesASM Pharmacology and Clinical Efficacy 2021 PDFIchrak GhachemNo ratings yet
- Randomized Trial of Three Anticonvulsant Medications For Status EpilepticusDocument18 pagesRandomized Trial of Three Anticonvulsant Medications For Status EpilepticusBaiq Widaning Dwi AnjaniNo ratings yet
- World of Tanks Game Manual en Eu Web 9 0 1Document95 pagesWorld of Tanks Game Manual en Eu Web 9 0 1Catarig IoanNo ratings yet
- Roxiva RX1 User GuideDocument17 pagesRoxiva RX1 User GuideYaself BeatsNo ratings yet
- Wessex Neuro ICU GuidelinesDocument200 pagesWessex Neuro ICU GuidelinesJVSP Servicos Medicos LTDANo ratings yet
- Medical Surgical Nursing ReviewDocument97 pagesMedical Surgical Nursing ReviewBernadeth Josefa BorelaNo ratings yet
- Helen's Story EBookFINALDocument19 pagesHelen's Story EBookFINALGMDMNo ratings yet
- Dita 1Document8 pagesDita 1Jannah Miftahul JannahNo ratings yet
- CHCDIS007 STUDENT WORKBOOK (WORD) - C4A.v1.1Document86 pagesCHCDIS007 STUDENT WORKBOOK (WORD) - C4A.v1.1shrestha31dristi100% (2)
- War and Peace - Manual - PCDocument21 pagesWar and Peace - Manual - PCmab58No ratings yet
- Fasting Article Health Benefits 21dayDocument12 pagesFasting Article Health Benefits 21dayJosh BassNo ratings yet
- First Aid (Loss of Consciouness and Seizure) : Presentor: Nomer M. FerrerDocument7 pagesFirst Aid (Loss of Consciouness and Seizure) : Presentor: Nomer M. FerrerLuna CapitNo ratings yet