Download as pdf or txt
You might also like
- CS444: BIO INFORMATICS (Lab 1 - Manual) Bioinformatics Databases and Key Online ResourcesDocument2 pagesCS444: BIO INFORMATICS (Lab 1 - Manual) Bioinformatics Databases and Key Online ResourcesSUNDAS FATIMANo ratings yet
- Cancer Immunotherapy: An Update: Abul K. Abbas Ucsf Abul - Abbas@ucsf - EduDocument26 pagesCancer Immunotherapy: An Update: Abul K. Abbas Ucsf Abul - Abbas@ucsf - EduHarits AmrullohNo ratings yet
- Hematology Cell Morphology ChartDocument2 pagesHematology Cell Morphology ChartMiaoNo ratings yet
- Coronavirus Covid-19 (Sars-Cov-2) : MicrobiologyDocument17 pagesCoronavirus Covid-19 (Sars-Cov-2) : MicrobiologyRGeoNo ratings yet
- Sars-Cov-2 (Covid 19) : Ashish KumarDocument33 pagesSars-Cov-2 (Covid 19) : Ashish KumarAshishNo ratings yet
- Interim Clinical Guidance For Management of Patients With Confirmed Coronavirus Disease (COVID-19)Document11 pagesInterim Clinical Guidance For Management of Patients With Confirmed Coronavirus Disease (COVID-19)Nur Fitriana Aprilia Abong BoliNo ratings yet
- Management of Patients With Confirmed 2019-nCoV - CDCDocument9 pagesManagement of Patients With Confirmed 2019-nCoV - CDCIndah BerlianaNo ratings yet
- Guias CDCDocument15 pagesGuias CDCEliana TorresNo ratings yet
- Gandhi Et Al., NEJM Avril 2020Document9 pagesGandhi Et Al., NEJM Avril 2020carb0ne14rNo ratings yet
- Novel Coronavirus Infection (Covid-19) Basic GuideDocument9 pagesNovel Coronavirus Infection (Covid-19) Basic GuideSamanNo ratings yet
- COVID-19 Screening Prognosis and Severity Assessment With Biomarkers HORIBA MedicalDocument14 pagesCOVID-19 Screening Prognosis and Severity Assessment With Biomarkers HORIBA MedicalIrkania PasangkaNo ratings yet
- Covid 19 RadiologyDocument45 pagesCovid 19 Radiologyqayyum consultantfpscNo ratings yet
- Background of The Problem: Sarbecovirus, OrthocoronavirinaeDocument16 pagesBackground of The Problem: Sarbecovirus, Orthocoronavirinaesamiza1122No ratings yet
- 1 s2.0 S0272638620306120 ManinDocument10 pages1 s2.0 S0272638620306120 ManinrezaNo ratings yet
- Coronavirus DiseaseDocument5 pagesCoronavirus DiseaseShanice BedecirNo ratings yet
- Mild or Moderate Covid-19Document9 pagesMild or Moderate Covid-19Gabriela ArvelaezNo ratings yet
- Mild or Moderate Covid-19: Clinical PracticeDocument9 pagesMild or Moderate Covid-19: Clinical PracticeJulio MejiaNo ratings yet
- ICMR 2021 Conference PresentationDocument16 pagesICMR 2021 Conference PresentationDr Noor Muhammad KhanNo ratings yet
- 2019 Novel Coronavirus Disease (COVID-19) in Taiwan: Reports of Two Cases From Wuhan, ChinaDocument4 pages2019 Novel Coronavirus Disease (COVID-19) in Taiwan: Reports of Two Cases From Wuhan, ChinaClaav HugNo ratings yet
- Information About The New Coronavirus Disease (COVID-19) : EditorialDocument2 pagesInformation About The New Coronavirus Disease (COVID-19) : EditorialMishel PazmiñoNo ratings yet
- Coronavirus: Novel Coronavirus (COVID-19) Infection: TerminologyDocument13 pagesCoronavirus: Novel Coronavirus (COVID-19) Infection: TerminologyAMEU URGENCIASNo ratings yet
- A Case Series Describing The Epidemiology and Clinical Characteristics of COVID-19 Infection in Jilin ProvinceDocument4 pagesA Case Series Describing The Epidemiology and Clinical Characteristics of COVID-19 Infection in Jilin Provinceabeer alrofaeyNo ratings yet
- Mild or Moderate Covid-19: Clinical PracticeDocument9 pagesMild or Moderate Covid-19: Clinical PracticeLenin CarrilloNo ratings yet
- COVID-19: UM Icrob Iolog yDocument50 pagesCOVID-19: UM Icrob Iolog yJana AbdulrahimNo ratings yet
- Severe Acute Respiratory Syndrome (SARS)Document9 pagesSevere Acute Respiratory Syndrome (SARS)Elenor AbrigoNo ratings yet
- InterimGuidance ClinicalManagement NovelCoronavirus 11feb13uDocument12 pagesInterimGuidance ClinicalManagement NovelCoronavirus 11feb13uAdhiyasa PrimagupitaNo ratings yet
- M E R S C (Mers-C V) : Iddle Astern Espiratory Yndrome Oronavirus ODocument35 pagesM E R S C (Mers-C V) : Iddle Astern Espiratory Yndrome Oronavirus OAhmad Riski Putra SibodakNo ratings yet
- A Review of Sars-Cov-2 and The Ongoing Clinical Trials: Molecular SciencesDocument19 pagesA Review of Sars-Cov-2 and The Ongoing Clinical Trials: Molecular SciencesJoseGarciaNo ratings yet
- JGRH 23 001Document11 pagesJGRH 23 001yakalapunagarajuNo ratings yet
- Elsevier Order Sets: COVID-19 - Ward (3.0)Document36 pagesElsevier Order Sets: COVID-19 - Ward (3.0)LyleChristineNo ratings yet
- Covid 19Document16 pagesCovid 19aliaaNo ratings yet
- Aditi 03 SPPDocument8 pagesAditi 03 SPPAbhishekNo ratings yet
- Elsevier Order Sets: COVID-19 - Ward (2.2)Document36 pagesElsevier Order Sets: COVID-19 - Ward (2.2)Bryam PradoNo ratings yet
- Management Booklet Coronavirus Disease MOHP - 2019 - 28marchDocument22 pagesManagement Booklet Coronavirus Disease MOHP - 2019 - 28marchSanaa SbdelghanyNo ratings yet
- Novel CoronavirusDocument7 pagesNovel CoronavirusMustafa KhudhairNo ratings yet
- Management of Patients With Confirmed 2019-NCoV - CDCDocument6 pagesManagement of Patients With Confirmed 2019-NCoV - CDCadrianbyeNo ratings yet
- Nejmcp 2009249Document10 pagesNejmcp 2009249carb0ne14rNo ratings yet
- Absence SarsDocument15 pagesAbsence SarsJames LindonNo ratings yet
- Cip On CovidDocument40 pagesCip On CovidLorenz L. Llamas IIINo ratings yet
- Preliminary Study To Identify Severe From Moderate Cases of COVID-19 Using Combined Hematology ParametersDocument15 pagesPreliminary Study To Identify Severe From Moderate Cases of COVID-19 Using Combined Hematology Parameterstrisna amijayaNo ratings yet
- Ahora EsteDocument6 pagesAhora EsteJhosua MendezNo ratings yet
- Radiologic Diagnosis of Patients With COVID-19: Serie: Radiology AND COVID-19Document18 pagesRadiologic Diagnosis of Patients With COVID-19: Serie: Radiology AND COVID-19zzooooeeeeeeNo ratings yet
- Radiologic Diagnosis of Patients With COVID-19Document19 pagesRadiologic Diagnosis of Patients With COVID-19Muhammad ImamHanafiNo ratings yet
- Journal Pre-Proof: Journal of Cardiothoracic and Vascular AnesthesiaDocument21 pagesJournal Pre-Proof: Journal of Cardiothoracic and Vascular AnesthesiaJuan Esteban Paez MolinaNo ratings yet
- Coronavirus: Novel Coronavirus (COVID-19) Infection: TerminologyDocument12 pagesCoronavirus: Novel Coronavirus (COVID-19) Infection: TerminologyvgmanjunathNo ratings yet
- PIIS0002961020302221Document4 pagesPIIS0002961020302221kuncoroNo ratings yet
- The Management of Coronavirus Disease 2019 (COVID 19) : Jialin Liu - Siru LiuDocument7 pagesThe Management of Coronavirus Disease 2019 (COVID 19) : Jialin Liu - Siru LiuFina RepitiyanaNo ratings yet
- Mild or Moderate Covid-19: Clinical PracticeDocument10 pagesMild or Moderate Covid-19: Clinical PracticeRanda NorayNo ratings yet
- Reporting About SARSDocument2 pagesReporting About SARSJames TadeoNo ratings yet
- COVID - Topic SummaryDocument2 pagesCOVID - Topic SummaryJihad U. ShariefNo ratings yet
- Clinico-Radiological Profile in Covid - 19 PatientsDocument6 pagesClinico-Radiological Profile in Covid - 19 PatientsInternational Journal of Innovative Science and Research Technology100% (1)
- Covid 19: Dennis N. Muñoz, RN, RM, LPTDocument103 pagesCovid 19: Dennis N. Muñoz, RN, RM, LPTDennis Nabor Muñoz, RN,RMNo ratings yet
- Novel Coronavirus Pneumonia Diagnosis TreatmentDocument10 pagesNovel Coronavirus Pneumonia Diagnosis TreatmentDodi Samartino100% (4)
- Investigating COVID-19: By: Hadeel Abdulrhman Alrehily ID: 4051552Document12 pagesInvestigating COVID-19: By: Hadeel Abdulrhman Alrehily ID: 4051552hade elNo ratings yet
- Covid 19: Rajni SharmaDocument33 pagesCovid 19: Rajni SharmaJuan CruzNo ratings yet
- Articulo Por TraducirDocument4 pagesArticulo Por TraducirAntonio Zumaque CarrascalNo ratings yet
- WHF COVID19 PresentationDocument41 pagesWHF COVID19 PresentationWallyNo ratings yet
- EBM Case Write Up - To Rule Out MERS COVDocument5 pagesEBM Case Write Up - To Rule Out MERS COVFaiz TaqiuNo ratings yet
- Covid-19 AddendumDocument10 pagesCovid-19 AddendumPrecious Bardon-MempinNo ratings yet
- DR Sudhir Bhandari Final Presentation 12-4-2021 NewDocument67 pagesDR Sudhir Bhandari Final Presentation 12-4-2021 NewsurruNo ratings yet
- COVID-19 and Multi-Organ ResponseDocument31 pagesCOVID-19 and Multi-Organ ResponseArbaz SultanNo ratings yet
- NICE Way to Cure COVID -19From EverandNICE Way to Cure COVID -19Rating: 4.5 out of 5 stars4.5/5 (8)
- Enzyme RegulationDocument1 pageEnzyme RegulationVea AngelesNo ratings yet
- Cultivationofvirus2 171125163046Document8 pagesCultivationofvirus2 171125163046Ilyas MathakiyaNo ratings yet
- HIV and AIDS Myths, Facts, and The FutureDocument6 pagesHIV and AIDS Myths, Facts, and The FuturehendoramuNo ratings yet
- Lesson 8 Activity - Ma. Bernadeth LanozaDocument7 pagesLesson 8 Activity - Ma. Bernadeth LanozaEmily Despabiladeras DulpinaNo ratings yet
- Thesis Topic in Blood BankingDocument6 pagesThesis Topic in Blood Bankingashleygomezalbuquerque100% (2)
- Biology 500 Questions PDF Compressed 1557665526 36Document48 pagesBiology 500 Questions PDF Compressed 1557665526 36santu surendra50% (2)
- MCB 301 Monoclonal AntibodiesDocument10 pagesMCB 301 Monoclonal AntibodiesUsman SurajNo ratings yet
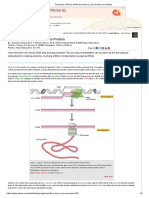
- Translation Dna To Mrna To ProteinDocument5 pagesTranslation Dna To Mrna To ProteinAna MarianaNo ratings yet
- Etextbook 978 0323319676 Andrews Diseases of The Skin Clinical DermatologyDocument61 pagesEtextbook 978 0323319676 Andrews Diseases of The Skin Clinical Dermatologyeric.chandler298100% (60)
- Protection From Vaxx Shedding - Top Medical Experts Share Proven ProtocolsDocument19 pagesProtection From Vaxx Shedding - Top Medical Experts Share Proven ProtocolsShankar RNo ratings yet
- MedSCi Midterm Practice Biomembranes MCQDocument5 pagesMedSCi Midterm Practice Biomembranes MCQPat FerrerNo ratings yet
- Blood & HematologyDocument6 pagesBlood & HematologyAymen OmerNo ratings yet
- Causes and Symptoms of Mental RetardationDocument3 pagesCauses and Symptoms of Mental RetardationCh. Asad NisarNo ratings yet
- Solution Manual For Biological Science 5th Edition 032174361x 9780321743619Document8 pagesSolution Manual For Biological Science 5th Edition 032174361x 9780321743619JamesNewmanjxag100% (39)
- Chemo TrophsDocument3 pagesChemo Trophslei sandovalNo ratings yet
- The Immune SystemDocument29 pagesThe Immune SystemLalajimNo ratings yet
- Collection of Blood From DonorsDocument7 pagesCollection of Blood From DonorsBernardoHernandezNo ratings yet
- BioFire RP2 1 RP2 1plus Control Panel M441Document4 pagesBioFire RP2 1 RP2 1plus Control Panel M441Cecil James BuguisNo ratings yet
- A Cysteine: Well Done, You Have Selected The Right AnswerDocument56 pagesA Cysteine: Well Done, You Have Selected The Right AnswerHardiTariqHammaNo ratings yet
- Cell Structure and FunctionDocument8 pagesCell Structure and FunctionTshibambeNo ratings yet
- General Biology 1: Disorders and Diseases: Cell Cycle Learning Activity 1: Mistakes in Cell DivisionDocument1 pageGeneral Biology 1: Disorders and Diseases: Cell Cycle Learning Activity 1: Mistakes in Cell DivisionArianne AtilasNo ratings yet
- Protein Subunits VaccineDocument14 pagesProtein Subunits Vaccineahmed 9No ratings yet
- Immune System Notes IB HL BioDocument6 pagesImmune System Notes IB HL BioJordan SuttonNo ratings yet
- The Emergence and Persistence of C Auris in Western New YorkDocument4 pagesThe Emergence and Persistence of C Auris in Western New YorkLilia JouNo ratings yet
- Dna PolymorphismDocument25 pagesDna Polymorphismwajiha_mppl558992% (13)
- Oral Comm - W4 - Answer SheetDocument3 pagesOral Comm - W4 - Answer SheetKrista. meters100% (1)
- HADocument29 pagesHAobai abed100% (2)