Download as pdf or txt
You might also like
- Week 3 - Code of Ethics in BusinessDocument6 pagesWeek 3 - Code of Ethics in BusinessSeverus S Potter100% (3)
- Sample HR FormDocument4 pagesSample HR FormJesstoni CaniedoNo ratings yet
- M&S - Application For EmploymentDocument4 pagesM&S - Application For EmploymentAlaghen VespanathanNo ratings yet
- QR 2.1-1-3-c Job Application FormDocument3 pagesQR 2.1-1-3-c Job Application FormMochammad Aji HutamaNo ratings yet
- HRD Form 001 Employee Application Gen - Admin v.001Document3 pagesHRD Form 001 Employee Application Gen - Admin v.001DadangNo ratings yet
- Job Application FormDocument6 pagesJob Application FormYi YiNo ratings yet
- Personal Information SheetDocument3 pagesPersonal Information SheetPaula ValerioNo ratings yet
- PSRC APPLICATION FORM With DPA Consent 2021 - Copy (Replica) (Replica)Document2 pagesPSRC APPLICATION FORM With DPA Consent 2021 - Copy (Replica) (Replica)Edcel SilvaNo ratings yet
- Information Sheet: Availability For Employment: Position Applied ForDocument8 pagesInformation Sheet: Availability For Employment: Position Applied ForMedel Cay De CastroNo ratings yet
- BIGTIME EMPIRE - Application FormDocument2 pagesBIGTIME EMPIRE - Application FormJasfer BucoNo ratings yet
- Application Form ASTON BintaroDocument3 pagesApplication Form ASTON BintaroROOMS ARTOTEL CASA CIKARANGNo ratings yet
- ContohDocument4 pagesContohhrddenpasar43No ratings yet
- Employee Profile Sheet: University of The VisayasDocument1 pageEmployee Profile Sheet: University of The VisayasTess TanNo ratings yet
- Employment Application FormDocument6 pagesEmployment Application FormAMYSOPHIANI BINTI ADENI MoeNo ratings yet
- Loan Application FormDocument2 pagesLoan Application FormDean DanaiNo ratings yet
- Sample Application For EmploymentDocument2 pagesSample Application For EmploymentBeyond the Rack PHNo ratings yet
- Welcome To Blue Cross and Blue Shield of Illinois and Fort Dearborn LifeDocument6 pagesWelcome To Blue Cross and Blue Shield of Illinois and Fort Dearborn LifeBuy BaNo ratings yet
- CIS Form BlankDocument2 pagesCIS Form Blanksst291979No ratings yet
- F-0349-15 - Information SheetDocument2 pagesF-0349-15 - Information SheetJohn Linard AninggaNo ratings yet
- Advt 19 2022 App FormDocument1 pageAdvt 19 2022 App FormVjsjjsvNo ratings yet
- Application Form V3 Jan 2022Document4 pagesApplication Form V3 Jan 2022IT Gunungmas GroupNo ratings yet
- Tcah Employment Application1-1Document5 pagesTcah Employment Application1-1api-127560226No ratings yet
- CocaCola Application FormDocument5 pagesCocaCola Application FormThanh VinhNo ratings yet
- Johnny Q - Employment Application FormDocument3 pagesJohnny Q - Employment Application Formprettyboiricky54No ratings yet
- Employee Application PacketDocument7 pagesEmployee Application PacketAlex BlancoNo ratings yet
- Filled Application FormDocument4 pagesFilled Application FormsabbysamuraNo ratings yet
- Pakistan Red Crescent Society: Employment Application FormDocument4 pagesPakistan Red Crescent Society: Employment Application FormOmar BhuttaNo ratings yet
- Employee Data (Application) FormDocument2 pagesEmployee Data (Application) FormGlaneisia MitchellNo ratings yet
- Application For EmploymentDocument3 pagesApplication For EmploymentFrankylle ArreoNo ratings yet
- Company Application Form - SRPDocument3 pagesCompany Application Form - SRPlabasr25No ratings yet
- ISSPL JoiningKitDocument13 pagesISSPL JoiningKitTempooooNo ratings yet
- BWapplicationDocument5 pagesBWapplicationTinaNo ratings yet
- Job Application Form: Section-1 Personal DetailsDocument10 pagesJob Application Form: Section-1 Personal DetailsSyed SamiNo ratings yet
- Job ApplicationDocument2 pagesJob Applicationrico.vazquezNo ratings yet
- Form 1-200 - Job Applicn FormDocument4 pagesForm 1-200 - Job Applicn Formmassa.mirabelNo ratings yet
- Lets Work Digital ApplicationDocument29 pagesLets Work Digital ApplicationLovepreet malhiNo ratings yet
- T Application FormDocument3 pagesT Application Formjoangalanvelarde.14No ratings yet
- Employee Application / Personal Data Form: For Office Use OnlyDocument6 pagesEmployee Application / Personal Data Form: For Office Use OnlyRayvathy ParamatemaNo ratings yet
- Employmentapp - Mel 1Document3 pagesEmploymentapp - Mel 1Danielle TibbsNo ratings yet
- TugasDocument4 pagesTugasbimawiguna16No ratings yet
- Bachelor of Management With Honours: Matriculation No: Identity Card No.: Telephone No.: E-Mail: Learning CentreDocument6 pagesBachelor of Management With Honours: Matriculation No: Identity Card No.: Telephone No.: E-Mail: Learning CentreNurul AminNo ratings yet
- Personal Data Form (Experis IT Pvt. LTD.) - NewDocument3 pagesPersonal Data Form (Experis IT Pvt. LTD.) - NewDNYANESHWAR PAWARNo ratings yet
- Checkers Job ApplicationlDocument2 pagesCheckers Job ApplicationlshanecordeNo ratings yet
- TylerDocument3 pagesTylerwdj721986No ratings yet
- Application Form-MDCIVDI Ao 17jun2020Document2 pagesApplication Form-MDCIVDI Ao 17jun2020Justine ColesNo ratings yet
- VBAgreementDocument21 pagesVBAgreementapi-3827739No ratings yet
- Stpi 3ApplicationTvm1Document2 pagesStpi 3ApplicationTvm1Chetan SehgalNo ratings yet
- Cornerstone Academy Day Center 2720 Arlington Drive Alexandria, Va 22306 (703) 768-9355 (703) 768-9355 FaxDocument2 pagesCornerstone Academy Day Center 2720 Arlington Drive Alexandria, Va 22306 (703) 768-9355 (703) 768-9355 FaxDimple PatelNo ratings yet
- K Inetic Engineering LimitedDocument6 pagesK Inetic Engineering Limitedatul_raj4No ratings yet
- Volunteer Registration Form Updated June 2021Document4 pagesVolunteer Registration Form Updated June 2021keamomalebe1No ratings yet
- AEP Form Region IVDocument1 pageAEP Form Region IVAllan YdiaNo ratings yet
- ATS Joining KitDocument25 pagesATS Joining Kitmukeshkushwah01031993No ratings yet
- Professional Data SheetDocument6 pagesProfessional Data SheetMLBoBo GAMINGNo ratings yet
- Employee Salary Loan (Esl) Application Form: Borrower InformationDocument4 pagesEmployee Salary Loan (Esl) Application Form: Borrower Information813 cafeNo ratings yet
- New Employee Information TemplateDocument3 pagesNew Employee Information Templateyudha.aditia76No ratings yet
- Minconsult - Job Application FormDocument5 pagesMinconsult - Job Application FormPoi HHNo ratings yet
- House Job Application FormDocument2 pagesHouse Job Application FormRahem AhsanNo ratings yet
- HERITAGEapplicationform 1Document8 pagesHERITAGEapplicationform 1rapheal jamesNo ratings yet
- Yoga Fit Interview FormsDocument3 pagesYoga Fit Interview FormsshintaNo ratings yet
- Sweet Success: Knowledge and Quick-Skills in Thirty MinutesFrom EverandSweet Success: Knowledge and Quick-Skills in Thirty MinutesNo ratings yet
- VS UserGuideDocument47 pagesVS UserGuideJanine CanlasNo ratings yet
- Department of Education: General Class Program For Kindergarten and Grade 1 (First Sem)Document15 pagesDepartment of Education: General Class Program For Kindergarten and Grade 1 (First Sem)Janine CanlasNo ratings yet
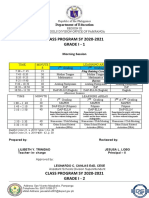
- CLASS PROGRAM SY 2020-2021 Grade I - 1: Department of EducationDocument3 pagesCLASS PROGRAM SY 2020-2021 Grade I - 1: Department of EducationJanine CanlasNo ratings yet
- Statement of Account 96 07 Mar 20 To 06 Apr 20 845383606 (45) 3015917Document2 pagesStatement of Account 96 07 Mar 20 To 06 Apr 20 845383606 (45) 3015917Janine CanlasNo ratings yet
- Department of Education: Minutes of The Meeting (April 7, 2020)Document5 pagesDepartment of Education: Minutes of The Meeting (April 7, 2020)Janine CanlasNo ratings yet
- Brigada Eskwela Form 7 School Accomplishment ReportDocument7 pagesBrigada Eskwela Form 7 School Accomplishment ReportJanine CanlasNo ratings yet
- JOINT 2020 BRIGADA ESKWELA AND OPLAN BALIK ESKWELA. Enrollment ProceduresDocument48 pagesJOINT 2020 BRIGADA ESKWELA AND OPLAN BALIK ESKWELA. Enrollment ProceduresJanine CanlasNo ratings yet
- Brigada Eskwela Form 3 Resource Mobilization FormDocument3 pagesBrigada Eskwela Form 3 Resource Mobilization FormJanine CanlasNo ratings yet
- Noted: - School Head DateDocument2 pagesNoted: - School Head DateJanine CanlasNo ratings yet
- Multiple Choice Questions of Microsoft ExcelDocument3 pagesMultiple Choice Questions of Microsoft ExcelJanine CanlasNo ratings yet
- Melgar National High School Action Plan in Lis/Ebeis School Year 2019-2020Document1 pageMelgar National High School Action Plan in Lis/Ebeis School Year 2019-2020Janine CanlasNo ratings yet
- Mathematics: The Training and Use of ICT in Teaching Perceptions of Melilla's (Spain) Mathematics TeachersDocument20 pagesMathematics: The Training and Use of ICT in Teaching Perceptions of Melilla's (Spain) Mathematics TeachersJanine CanlasNo ratings yet
- Quarter 4 Summative Test No. 1 Mga Layunin Code Bahagda N Bilang NG Aytem Kinalalagyan NG BilangDocument4 pagesQuarter 4 Summative Test No. 1 Mga Layunin Code Bahagda N Bilang NG Aytem Kinalalagyan NG BilangJanine Canlas100% (4)
- SESSION 11 Allocating Retail Space To ProductsDocument27 pagesSESSION 11 Allocating Retail Space To ProductsAmisha SinghNo ratings yet
- Product Slate ExportDocument123 pagesProduct Slate ExportVegeta SaiyanNo ratings yet
- UK #1 Used Office Furniture SupplierDocument2 pagesUK #1 Used Office Furniture SupplierSecond hand Office furnitureNo ratings yet
- Statement of Account: Date Narration Chq./Ref - No. Value DT Withdrawal Amt. Deposit Amt. Closing BalanceDocument2 pagesStatement of Account: Date Narration Chq./Ref - No. Value DT Withdrawal Amt. Deposit Amt. Closing BalancePriyanka SangleNo ratings yet
- PDI Manual0327 (Final)Document77 pagesPDI Manual0327 (Final)Amine KhadirNo ratings yet
- Ray-Ban Final Marketing Plan: June 13, 2019 MKTG 464 Ayaka Fuwa, Chloe George, Diane Hoang, & Kazutaka TakeuchiDocument25 pagesRay-Ban Final Marketing Plan: June 13, 2019 MKTG 464 Ayaka Fuwa, Chloe George, Diane Hoang, & Kazutaka TakeuchiГоліаф ГоліафNo ratings yet
- ISO 9001 - Quality Management Standard: ISO 9001 - What Is It?Document6 pagesISO 9001 - Quality Management Standard: ISO 9001 - What Is It?Harshit MistryNo ratings yet
- Jovana ObućinaDocument2 pagesJovana Obućinajovanao91No ratings yet
- Managerial Accounting 2nd Edition Braun Test BankDocument24 pagesManagerial Accounting 2nd Edition Braun Test BankAnthonyWeaveracey100% (50)
- Bayyaram Pay BillsDocument6 pagesBayyaram Pay BillsMatta Madhu Sudhana RaoNo ratings yet
- Musik Paper11Document22 pagesMusik Paper11vinal.sharmaNo ratings yet
- OD429419745237938100Document2 pagesOD429419745237938100jd2saiNo ratings yet
- Pengaruh Profitabilitas, Kebijakan Dividen, PertumbuhanDocument20 pagesPengaruh Profitabilitas, Kebijakan Dividen, PertumbuhanFairuzeta YoganandaNo ratings yet
- Aced 23 Module 2-3Document14 pagesAced 23 Module 2-3JessaNo ratings yet
- Derivative Chapter Test: Reading 45: Derivative Markets & InstrumentsDocument9 pagesDerivative Chapter Test: Reading 45: Derivative Markets & InstrumentsNistha SinghNo ratings yet
- Bartender Resume ObjectiveDocument5 pagesBartender Resume Objectiveafaocsazx100% (2)
- Nop 180Document2 pagesNop 180tanaNo ratings yet
- Ias/Pas 34: Interim Financial ReportingDocument29 pagesIas/Pas 34: Interim Financial ReportingFranz NayangaNo ratings yet
- Characteristics of A PartnershipDocument3 pagesCharacteristics of A Partnershipskilled legilimenceNo ratings yet
- Sony Corporation Mission StatementDocument3 pagesSony Corporation Mission StatementvampireweekendNo ratings yet
- Company Law 2 NotesDocument17 pagesCompany Law 2 NotesRidhima BansalNo ratings yet
- Learning Packet 4 EditedDocument7 pagesLearning Packet 4 EditedNatalie SerranoNo ratings yet
- Spergeon Aaiclas ReportDocument36 pagesSpergeon Aaiclas ReportspergeonNo ratings yet
- Strength Based DevelopmentDocument17 pagesStrength Based DevelopmentRajadhi RajaNo ratings yet
- 520 987 3 PBDocument6 pages520 987 3 PBnasonex91No ratings yet
- 15.05.2023 Cause List C - IiDocument6 pages15.05.2023 Cause List C - IiPranay ChauguleNo ratings yet
- NSTP Module - Lesson 5Document5 pagesNSTP Module - Lesson 5Maira Garcia C.No ratings yet
- Lee Vs Simando DIGESTDocument2 pagesLee Vs Simando DIGESTLenneo SorianoNo ratings yet
- SLT Ar 2012Document204 pagesSLT Ar 2012sriramrangaNo ratings yet