Download as pdf or txt
You might also like
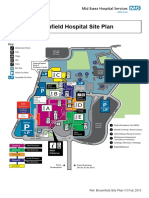
- Broomfield Hospital Site Plan: Café Shops Lifts Information PointsDocument1 pageBroomfield Hospital Site Plan: Café Shops Lifts Information Pointsady trader0% (2)
- AncientSciLife 2015 34 3 168 157163Document6 pagesAncientSciLife 2015 34 3 168 157163Cristian MuñozNo ratings yet
- Cerebral PalsyDocument9 pagesCerebral PalsysanjayNo ratings yet
- Cerebral Palsy A Clinico-Social Case ReportDocument5 pagesCerebral Palsy A Clinico-Social Case ReportNovie AstiniNo ratings yet
- A Case of Lateral Rectus Palsy by DR Sunil KannadaDocument5 pagesA Case of Lateral Rectus Palsy by DR Sunil KannadaHomoeopathic Pulse100% (1)
- 12 1021Casereport-SunithaDocument6 pages12 1021Casereport-SunithaJerry F. Abellera Jr.No ratings yet
- Paediatrica Indonesiana: Case ReportDocument9 pagesPaediatrica Indonesiana: Case ReportEHbsd WardNo ratings yet
- DR NuwanSMarasinhgacpaetyparticleDocument18 pagesDR NuwanSMarasinhgacpaetyparticleSanjanaNo ratings yet
- Prevlance of Sleep 2017Document23 pagesPrevlance of Sleep 2017mehak razzakNo ratings yet
- CSRCase StudyDocument11 pagesCSRCase StudyPNo ratings yet
- Evidence TeaDocument17 pagesEvidence TeapaulyfonoNo ratings yet
- DjhdeguweglugwelueDocument7 pagesDjhdeguweglugwelueviolaarisanti6No ratings yet
- 535 1522 1 PBDocument4 pages535 1522 1 PBSebastián Ghiso JiménezNo ratings yet
- A Clinical Study On Down Syndrome and Its Management With AyurvedaDocument4 pagesA Clinical Study On Down Syndrome and Its Management With AyurvedaEditor IJTSRDNo ratings yet
- Scalp Acupuncture Treatment For Children With Autism and AdhdDocument13 pagesScalp Acupuncture Treatment For Children With Autism and AdhdJujun100% (1)
- Ayurvedic InterventionDocument6 pagesAyurvedic InterventionNeutron ZionNo ratings yet
- Children With Autism Spectrum Disorders The Importance of Medical Investigations - Isaken 2013Document10 pagesChildren With Autism Spectrum Disorders The Importance of Medical Investigations - Isaken 2013c_mosNo ratings yet
- Our Experience With Childhood Pervasive Developmental Disorders (Autism and Asperger Syndrome) : Cure Is PossibleDocument8 pagesOur Experience With Childhood Pervasive Developmental Disorders (Autism and Asperger Syndrome) : Cure Is PossibleAamir Jalal Al-MosawiNo ratings yet
- Cognitive Development in Anemic Infants of Different PrakritiFrom EverandCognitive Development in Anemic Infants of Different PrakritiNo ratings yet
- Sertraline-Induced DiplopiaDocument3 pagesSertraline-Induced DiplopiaVikas PsNo ratings yet
- Autism Spectrum Disorder (Updated), A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandAutism Spectrum Disorder (Updated), A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- 4 PDFDocument11 pages4 PDFHrishikesh BapatNo ratings yet
- A Case Study On The Ayurvedic Management of Cerebral PalsyDocument10 pagesA Case Study On The Ayurvedic Management of Cerebral PalsyHiramandalam PatanjaliNo ratings yet
- Turnitin CASE REPORT UlilDocument33 pagesTurnitin CASE REPORT Ulilulfap1917No ratings yet
- Shashtika Shali Pinda Sweda in The Management of Cerebral Palsy A Critical ReviewDocument4 pagesShashtika Shali Pinda Sweda in The Management of Cerebral Palsy A Critical Reviewshashankns.29No ratings yet
- Management and Treatment For Cerebral Palsy in Chi PDFDocument7 pagesManagement and Treatment For Cerebral Palsy in Chi PDFSumon RahatNo ratings yet
- Scope of Panchakarma in Neuro Developmental DisordersDocument8 pagesScope of Panchakarma in Neuro Developmental DisordersNatseen100% (1)
- Oxytocin and Arginine Vasopressin - A Bridge Between Acupuncture and Autism Spectrum DisorderDocument6 pagesOxytocin and Arginine Vasopressin - A Bridge Between Acupuncture and Autism Spectrum DisordersovalaxNo ratings yet
- Ethical Implications For Providers Regarding Cannabis Use in Children With Autism Spectrum DisordersDocument9 pagesEthical Implications For Providers Regarding Cannabis Use in Children With Autism Spectrum DisordersShane BalbidoNo ratings yet
- Carcinosinum in AutismDocument10 pagesCarcinosinum in AutismDarko BelevNo ratings yet
- A Case Study On MigraineDocument35 pagesA Case Study On MigraineRitu ShewaniNo ratings yet
- ADHD, Asperger Syndrome, and High-Functioning Autism: ArticleDocument4 pagesADHD, Asperger Syndrome, and High-Functioning Autism: Articlelaura2121No ratings yet
- IJCRR Nov2020 Vol12 Issue22Document9 pagesIJCRR Nov2020 Vol12 Issue22Aravind KumarNo ratings yet
- Rhizomelic Chondrodysplasia Punctata Type 1: Report of Mutations in 3 Children From IndiaDocument5 pagesRhizomelic Chondrodysplasia Punctata Type 1: Report of Mutations in 3 Children From IndiaSM SCANSNo ratings yet
- An Ayurvedic Protocol To Manage Retinitis Pigmentosa - A Case ReportDocument8 pagesAn Ayurvedic Protocol To Manage Retinitis Pigmentosa - A Case ReportAravind KumarNo ratings yet
- Ametropia in Children With Headache: Original ArticleDocument4 pagesAmetropia in Children With Headache: Original ArticlesondiNo ratings yet
- An Instrumented Assessment of Cerebral Palsy: A Systematic ReviewDocument7 pagesAn Instrumented Assessment of Cerebral Palsy: A Systematic ReviewDr Sharique AliNo ratings yet
- IJP - Volume 5 - Issue 12 - Pages 6245-6252Document8 pagesIJP - Volume 5 - Issue 12 - Pages 6245-6252Rayhand MubarakhNo ratings yet
- Autism 07april 2019Document26 pagesAutism 07april 2019هلا دلبحNo ratings yet
- 3849 PDFDocument5 pages3849 PDFAravind KumarNo ratings yet
- A432 4 FullDocument2 pagesA432 4 FullArturo ArturoNo ratings yet
- Pediatric Neurology - Essentials For General PracticeDocument352 pagesPediatric Neurology - Essentials For General Practiceashrafholail100% (1)
- Cerebral Palsy in Pakistani Children: A Hospital Based SurveyDocument8 pagesCerebral Palsy in Pakistani Children: A Hospital Based Surveyclaimstudent3515No ratings yet
- Health Sciences Major For College Occupational Therapy by SlidesgoDocument17 pagesHealth Sciences Major For College Occupational Therapy by Slidesgoulfap1917No ratings yet
- Psychogenic Non-Epileptic Seizures: Indian Pediatrics November 2004Document4 pagesPsychogenic Non-Epileptic Seizures: Indian Pediatrics November 2004Nico NicoNo ratings yet
- Clinicians Guide To AutismDocument20 pagesClinicians Guide To AutismNadia Desanti RachmatikaNo ratings yet
- Late Diagnosis of Congenital Hypothyroidism in Young Adult: Laurentius A. Pramono, Angelina YuwonoDocument3 pagesLate Diagnosis of Congenital Hypothyroidism in Young Adult: Laurentius A. Pramono, Angelina Yuwonovanilla wottledNo ratings yet
- A Case Report On Chronic Kidney DiseaseDocument4 pagesA Case Report On Chronic Kidney DiseaseEditor IJTSRDNo ratings yet
- Mama SelinDocument4 pagesMama SelinIndah LakataraNo ratings yet
- Idiopathic Short Stature Definition EpidDocument9 pagesIdiopathic Short Stature Definition Epidfrancisco perezNo ratings yet
- 1 s2.0 S0975947621001339 MainDocument5 pages1 s2.0 S0975947621001339 MainPooja TrivediNo ratings yet
- Thesis Topics in Pediatric NeurologyDocument6 pagesThesis Topics in Pediatric Neurologykarenoliverbaltimore100% (1)
- Scalp Acupuncture ASDDocument7 pagesScalp Acupuncture ASDHaryono zhuNo ratings yet
- Dif&dia&ped&gup&5 THDocument619 pagesDif&dia&ped&gup&5 THGokul Adarsh100% (1)
- Epilepsy and EEG Abnormalities in Children With Autism Spectrum DisordersDocument8 pagesEpilepsy and EEG Abnormalities in Children With Autism Spectrum DisordersBALTAZAR OTTONELLONo ratings yet
- Agbede DanielDocument18 pagesAgbede DanielDaniel AgbedeNo ratings yet
- Article WJPR 1402746141Document12 pagesArticle WJPR 1402746141Sahil MehtaNo ratings yet
- Breastfeeding Practices and Health-Seeking BehavioDocument12 pagesBreastfeeding Practices and Health-Seeking BehaviosiskaNo ratings yet
- Letters To The Editor: ReferenceDocument2 pagesLetters To The Editor: ReferenceEvelina Lestari NapitupuluNo ratings yet
- Mitsumoto ALS JAMA07Document11 pagesMitsumoto ALS JAMA07abcdefgNo ratings yet
- Prevalence of Prader-Willi Syndrome Among Infants With Hypotonia-2014Document4 pagesPrevalence of Prader-Willi Syndrome Among Infants With Hypotonia-2014nikos.alexandrNo ratings yet
- Hdat2en 4 52Document156 pagesHdat2en 4 52blahh12345689No ratings yet
- Math 8 Q3 Module 5 With Answer KeyDocument13 pagesMath 8 Q3 Module 5 With Answer KeyJimcris villamorNo ratings yet
- Wed Sept 6 GeographyDocument17 pagesWed Sept 6 Geographyapi-367886489No ratings yet
- Tel. ++39 011 9648211 - Fax ++39 011 9648222 E-Mail: Irem@irem - It - WWW - Irem.itDocument8 pagesTel. ++39 011 9648211 - Fax ++39 011 9648222 E-Mail: Irem@irem - It - WWW - Irem.itkenneth molina100% (1)
- Official Monopoly RulesDocument6 pagesOfficial Monopoly RuleswhatnotNo ratings yet
- Diff AmpDocument54 pagesDiff AmpUday GulghaneNo ratings yet
- Didactic ProductHighlights 2020 v2.6Document20 pagesDidactic ProductHighlights 2020 v2.6agus prasetioNo ratings yet
- 3.3.2.3 Lab - Configuring Rapid PVST, PortFast, and BPDU GuardDocument9 pages3.3.2.3 Lab - Configuring Rapid PVST, PortFast, and BPDU Guardsebastian ruiz100% (1)
- CT CalculationDocument2 pagesCT CalculationTheresia AndinaNo ratings yet
- The Building Blocks of Visual DesignDocument33 pagesThe Building Blocks of Visual DesignevandalismNo ratings yet
- Chapter Add On 1Document18 pagesChapter Add On 1Escada BebeyNo ratings yet
- 11.11th IPhO 1979Document11 pages11.11th IPhO 1979fienny37No ratings yet
- DS - Unit 3 - NotesDocument13 pagesDS - Unit 3 - NotesManikyarajuNo ratings yet
- Bastion Quickstart enDocument29 pagesBastion Quickstart enHalil DemirNo ratings yet
- Değişim Sınavı 2020Document29 pagesDeğişim Sınavı 2020Mustafa CinNo ratings yet
- Philippine Notices To MarinersDocument42 pagesPhilippine Notices To MarinersTaneo Prince CalebNo ratings yet
- Construct The Relational Model of The Following Scenario. (6 MARKS) System DescriptionDocument2 pagesConstruct The Relational Model of The Following Scenario. (6 MARKS) System DescriptionBushra ShahzadNo ratings yet
- Pesantren, Nahdlatul Ulama and Kiai As The Core of Santri Culture (PDFDrive)Document361 pagesPesantren, Nahdlatul Ulama and Kiai As The Core of Santri Culture (PDFDrive)fahmi azzamNo ratings yet
- History of Subcontinent NewspapersDocument1 pageHistory of Subcontinent NewspapersDaniyal Abbas Khan100% (3)
- Wandering Heroes of Ogre Gate - House of Paper ShadowsDocument97 pagesWandering Heroes of Ogre Gate - House of Paper ShadowsSamuel Smallman75% (4)
- Comnavsurfpac - Lant Inst 3840.1 Joint Surf ManualDocument72 pagesComnavsurfpac - Lant Inst 3840.1 Joint Surf ManualMontgomery BurksNo ratings yet
- Lesson Handouts ARGDocument26 pagesLesson Handouts ARGsamantha sisonNo ratings yet
- Perfect Manpower Consultancy (Invoice) of Mr. Inamullah SheikhDocument1 pagePerfect Manpower Consultancy (Invoice) of Mr. Inamullah Sheikhvikrant jaiswalNo ratings yet
- PRIsDocument11 pagesPRIsbobby choudharyNo ratings yet
- 2018 Trial 1 Biology Questions and Marking SchemeDocument11 pages2018 Trial 1 Biology Questions and Marking SchemeKodhekNo ratings yet
- BC 640Document5 pagesBC 640Miguel AngelNo ratings yet
- CBLM Smaw 1Document24 pagesCBLM Smaw 1Charis AbadNo ratings yet
- Bulletin Low Res 2Document19 pagesBulletin Low Res 2Аксана ГатауллинаNo ratings yet
- TAB Installation Instruction v1.1Document15 pagesTAB Installation Instruction v1.1vignesh. viswanathanNo ratings yet