Download as docx, pdf, or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- ABFAS Study GuideDocument368 pagesABFAS Study GuideMohammed FarhanNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Active Release TechniquesDocument15 pagesActive Release TechniquesPhysiotherapist Ali100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Self Massage Therapy PDFDocument26 pagesSelf Massage Therapy PDFMatthewNo ratings yet
- 5 Red-Hot Sex Tips From Real Women PDFDocument9 pages5 Red-Hot Sex Tips From Real Women PDFlaxepobime100% (1)
- Excel 2003 Shortcut Keys: Keys For Moving and Scrolling On WorksheetsDocument3 pagesExcel 2003 Shortcut Keys: Keys For Moving and Scrolling On WorksheetsPhysiotherapist AliNo ratings yet
- Abscess (US) : Mode Frequency Time IntensityDocument14 pagesAbscess (US) : Mode Frequency Time IntensityPhysiotherapist AliNo ratings yet
- IELTS Notes by Syed Ali HussainDocument11 pagesIELTS Notes by Syed Ali HussainPhysiotherapist AliNo ratings yet
- Coccygeal ManipulationDocument4 pagesCoccygeal ManipulationPhysiotherapist AliNo ratings yet
- Sample Emg/Ncv Report - Normal StudyDocument5 pagesSample Emg/Ncv Report - Normal StudyPhysiotherapist AliNo ratings yet
- Acupuncture Contraindications: Related Online Courses OnDocument14 pagesAcupuncture Contraindications: Related Online Courses OnPhysiotherapist Ali100% (1)
- Achilles RuptureDocument23 pagesAchilles RupturePhysiotherapist AliNo ratings yet
- Achilles Tendinopathy Toolkit Appendix BDocument86 pagesAchilles Tendinopathy Toolkit Appendix BPhysiotherapist AliNo ratings yet
- Achilles Tendinopathy Toolkit Summary of InterventionsDocument33 pagesAchilles Tendinopathy Toolkit Summary of InterventionsPhysiotherapist AliNo ratings yet
- Acetabulum FractureDocument32 pagesAcetabulum FracturePhysiotherapist AliNo ratings yet
- Accessory Navicular BoneDocument29 pagesAccessory Navicular BonePhysiotherapist AliNo ratings yet
- Above Knee Amputee Amputee Case StudyDocument4 pagesAbove Knee Amputee Amputee Case StudyPhysiotherapist AliNo ratings yet
- 10-Week Physical Activity Program For A Hypertensive Obese AdultDocument19 pages10-Week Physical Activity Program For A Hypertensive Obese AdultPhysiotherapist AliNo ratings yet
- Abbreviations in PhysiotherapyDocument53 pagesAbbreviations in PhysiotherapyPhysiotherapist AliNo ratings yet
- Abbey Pain Scale: Rethinking Pain Education Dysfunctional Breathing Neck Pain Assessment Case StudyDocument11 pagesAbbey Pain Scale: Rethinking Pain Education Dysfunctional Breathing Neck Pain Assessment Case StudyPhysiotherapist AliNo ratings yet
- Zongshen RX3 Owners Manual PDFDocument80 pagesZongshen RX3 Owners Manual PDFPhysiotherapist AliNo ratings yet
- Onsite & Remote Training: Clinical Application SpecialistDocument1 pageOnsite & Remote Training: Clinical Application SpecialistPhysiotherapist AliNo ratings yet
- The Effect of The Gastrocnemius On The Plantar Fascia: Javier Pascual HuertaDocument18 pagesThe Effect of The Gastrocnemius On The Plantar Fascia: Javier Pascual HuertamarcelonorisNo ratings yet
- Injury Prevention For RunnersDocument12 pagesInjury Prevention For RunnersMulaNo ratings yet
- Achilles Tendon Rupture Management - Mar18Document12 pagesAchilles Tendon Rupture Management - Mar18Leahu AgnesaNo ratings yet
- Pinky - Plantar FasciitisDocument34 pagesPinky - Plantar FasciitisRavindra choudharyNo ratings yet
- Functional TrainingDocument17 pagesFunctional TrainingNorthsideMMA100% (4)
- Black S Medical Dictionary PDFDocument2,413 pagesBlack S Medical Dictionary PDFAlexandr Trotsky100% (1)
- ABFAS - Trauma Section Flashcards - QuizletDocument21 pagesABFAS - Trauma Section Flashcards - Quizletpjanu86No ratings yet
- VisibleBody Knee Flexion EbookDocument13 pagesVisibleBody Knee Flexion EbookdophuNo ratings yet
- Feet and FootwearDocument383 pagesFeet and Footwearketilikaci100% (4)
- Shockwave Therapy Plus Eccentric Exercises Versus Isolated Eccentric Exercisesfor Achilles Insertional TendinopathyDocument8 pagesShockwave Therapy Plus Eccentric Exercises Versus Isolated Eccentric Exercisesfor Achilles Insertional TendinopathySergi ArnauNo ratings yet
- Anatomy Trains 3rd Edition Emag 1Document62 pagesAnatomy Trains 3rd Edition Emag 1Dibyendu BanerjeeNo ratings yet
- Ankle and Foot Examination PDFDocument16 pagesAnkle and Foot Examination PDFainizatiNo ratings yet
- Willits Accellerated Achilles RehabDocument2 pagesWillits Accellerated Achilles RehabattilabajusNo ratings yet
- 5105 - Achilles TendonDocument30 pages5105 - Achilles Tendonalbertina tebayNo ratings yet
- GB Seminar NotesDocument3 pagesGB Seminar Notesjosh100% (1)
- Achilles Tendon Rupture Metatarsal RuptureDocument26 pagesAchilles Tendon Rupture Metatarsal RuptureStar CruiseNo ratings yet
- Differential Diagnosis IIDocument32 pagesDifferential Diagnosis IIRaymondNo ratings yet
- Foot and Ankle Injuries Kylee Phillips - 0Document74 pagesFoot and Ankle Injuries Kylee Phillips - 0Charlez OhanuNo ratings yet
- Ankle and Foot Orthopedic TestsDocument9 pagesAnkle and Foot Orthopedic TestsVishal PatleNo ratings yet
- Achilles Tendonitis PresentationDocument22 pagesAchilles Tendonitis PresentationClaire HanniffyNo ratings yet
- Grade 11 Physical Education Module - Topic - AEROBIC EXERCISE - Mr. Neil Lloyd A. Pulan - Final - 02212019Document13 pagesGrade 11 Physical Education Module - Topic - AEROBIC EXERCISE - Mr. Neil Lloyd A. Pulan - Final - 02212019EDWARD JOSEPH D. MACOSENo ratings yet
- Q2 Nail Care Services 9 Module 3 W3 4 PDFDocument20 pagesQ2 Nail Care Services 9 Module 3 W3 4 PDFkrinessa erika m. de chavezNo ratings yet
- Study Guide: Workbook 1Document70 pagesStudy Guide: Workbook 1theron25No ratings yet
- Achilles Tendon Injuries: Signs and SymptomsDocument23 pagesAchilles Tendon Injuries: Signs and SymptomsahmadNo ratings yet
- Rehab Individual (Achilles Tendon Injury) - Raihan Naqibah Binti Mohamed (2021515847)Document21 pagesRehab Individual (Achilles Tendon Injury) - Raihan Naqibah Binti Mohamed (2021515847)Jalal NasirNo ratings yet
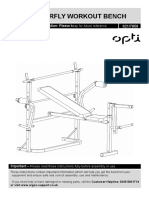
- Opti Butterfly Workout Bench: Assembly & User Instruction 621/7859Document27 pagesOpti Butterfly Workout Bench: Assembly & User Instruction 621/7859TunaNo ratings yet
- Medication Guide Floxin (Flox In) (Ofloxacin) : Reference ID: 2910767Document7 pagesMedication Guide Floxin (Flox In) (Ofloxacin) : Reference ID: 2910767Eko YuliantoNo ratings yet