Download as pdf or txt
You might also like
- Lesson Plan Breastfeeding PDFDocument13 pagesLesson Plan Breastfeeding PDFSrikutty Devu85% (20)
- SRL Diagnostics App On Your Mobile Device by Using QR Code. CALL Our Customer Care On 91115 91115Document1 pageSRL Diagnostics App On Your Mobile Device by Using QR Code. CALL Our Customer Care On 91115 91115Akhil ChawlaNo ratings yet
- F-5 Parts Catalog: Serial NoDocument96 pagesF-5 Parts Catalog: Serial Nokien100% (1)
- Rac Inspection ReportDocument13 pagesRac Inspection ReportDaniel DevineNo ratings yet
- Option QTR InfoDocument41 pagesOption QTR InfoAnwesha SatpathyNo ratings yet
- Manual PDFDocument470 pagesManual PDFDung Vo TanNo ratings yet
- Catalogo - Electro Adda FullDocument25 pagesCatalogo - Electro Adda Fulljcpp_18No ratings yet
- Technical Data of Sperre Air Compressors 50MW HFO Power PlantDocument4 pagesTechnical Data of Sperre Air Compressors 50MW HFO Power PlantAsim IbrahimNo ratings yet
- 4 - DS SATK Form - Transfer of Location 1.2Document3 pages4 - DS SATK Form - Transfer of Location 1.2Maybielyn DavidNo ratings yet
- Machinery Lubrication November December 2017 PDFDocument89 pagesMachinery Lubrication November December 2017 PDFJorge Cuadros BlasNo ratings yet
- Cat® Engine Specifications: C18 Acert Industrial EngineDocument5 pagesCat® Engine Specifications: C18 Acert Industrial EngineAsif MehmoodNo ratings yet
- Altronic V Installation Manual (FORM AV II)Document12 pagesAltronic V Installation Manual (FORM AV II)francis_mouille_iiNo ratings yet
- JGS620Document40 pagesJGS620Vik KarNo ratings yet
- Your Account Summary: Airtel Number Abb LTD MR Sandeep G ChandaliaDocument5 pagesYour Account Summary: Airtel Number Abb LTD MR Sandeep G Chandaliaskc3128No ratings yet
- Spare Parts Catalogue J Y962: Engine Number: 1422528 Module Number: 1422527Document368 pagesSpare Parts Catalogue J Y962: Engine Number: 1422528 Module Number: 1422527MD BOKTIAR KHOLZINo ratings yet
- Exhibit 2 - Agreement PDFDocument31 pagesExhibit 2 - Agreement PDFceroandoneNo ratings yet
- CLLK07 & 08 Technical Parameters BrochureDocument2 pagesCLLK07 & 08 Technical Parameters BrochureAlmario Sagun0% (1)
- Glory Parts Brazed Radiator CatalogueDocument42 pagesGlory Parts Brazed Radiator Cataloguegloryparts100% (1)
- Radiator Shop Wastes: Practical and ManualDocument20 pagesRadiator Shop Wastes: Practical and Manualvalley007No ratings yet
- PRAN-RFL Group PRAN-RFL Center, 105, Progoti Sarani, Middle Badda, Dhaka 1212, BangladeshDocument3 pagesPRAN-RFL Group PRAN-RFL Center, 105, Progoti Sarani, Middle Badda, Dhaka 1212, BangladeshSharif 087No ratings yet
- FM600-11-12-13-14 19 Spare Parts List PDFDocument2 pagesFM600-11-12-13-14 19 Spare Parts List PDFMario GallardoNo ratings yet
- Governor (Types I, II, IV, and V) - CheckDocument5 pagesGovernor (Types I, II, IV, and V) - CheckDaniel TekleNo ratings yet
- WaukeshaDocument2 pagesWaukeshacarlos angelNo ratings yet
- Valve Stem ProjectionDocument2 pagesValve Stem Projectionjose luis rattiaNo ratings yet
- RABiTAH Vendor Training ManualDocument53 pagesRABiTAH Vendor Training ManualAbu MajdNo ratings yet
- Manual Engine DrivenDocument81 pagesManual Engine DrivenAmit AryaNo ratings yet
- Upes Fee Invoice PDFDocument1 pageUpes Fee Invoice PDFJai SingalNo ratings yet
- Spare Parts D2866 E (5685935 000001)Document104 pagesSpare Parts D2866 E (5685935 000001)saginarseniyNo ratings yet
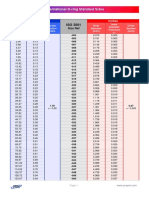
- O-Ring Standar Sizes PDFDocument14 pagesO-Ring Standar Sizes PDFJoseJSanchezNo ratings yet
- Cummins AEB 24.20 Iss 2004-02, Hoses and ConnectionsDocument35 pagesCummins AEB 24.20 Iss 2004-02, Hoses and ConnectionsKrzysztof OkrajekNo ratings yet
- Arrow Product OverviewDocument13 pagesArrow Product OverviewRafael Zurita100% (1)
- Document ListDocument64 pagesDocument ListBALACHITRANo ratings yet
- Quo Chest Freezer SupplierDocument2 pagesQuo Chest Freezer SupplierMOHAMED FAHMIE SYAFIQ BIN AHMAD BAKRI (LKIM)No ratings yet
- 723 Generator Control For Wärtsilä NSD Application & Hardware ManualDocument92 pages723 Generator Control For Wärtsilä NSD Application & Hardware ManualMussardNo ratings yet
- Cetane Number: University of Karbala College of Engineering Third StageDocument7 pagesCetane Number: University of Karbala College of Engineering Third StageMohamed ModerNo ratings yet
- Installation and Operation Manual: Booster ServomotorDocument32 pagesInstallation and Operation Manual: Booster ServomotorDiego Rosas100% (1)
- Altronic EPC 110-120 Operating Manual (FORM EPC-110/120 OM)Document55 pagesAltronic EPC 110-120 Operating Manual (FORM EPC-110/120 OM)francis_mouille_iiNo ratings yet
- MC 10127081 9999Document4 pagesMC 10127081 9999Jose yanezNo ratings yet
- 275GL Series 12V 275GL+: Gas Engine With ESM 2Document2 pages275GL Series 12V 275GL+: Gas Engine With ESM 2Jaadi 786100% (1)
- Copeland ZR125KC-TF5-950 Scroll Compressor - Carrier HVACDocument3 pagesCopeland ZR125KC-TF5-950 Scroll Compressor - Carrier HVACjacc42No ratings yet
- DSE7000 Configuration Suite ManualDocument117 pagesDSE7000 Configuration Suite ManualrodybarriosNo ratings yet
- PG M-Iii L2131 PDFDocument488 pagesPG M-Iii L2131 PDFnavy4No ratings yet
- Produktdatenblatt Ecofluid A Plus enDocument1 pageProduktdatenblatt Ecofluid A Plus enAbhishek kumarNo ratings yet
- Generador 250kwDocument15 pagesGenerador 250kwmax_velasquezNo ratings yet
- Installation - Operation - Maintenance: S70-101 IOM/JAN 2000Document66 pagesInstallation - Operation - Maintenance: S70-101 IOM/JAN 2000arielfernandomaxNo ratings yet
- Triumph Tr7 Tr8 Fuel Injection HandbookDocument82 pagesTriumph Tr7 Tr8 Fuel Injection Handbookjorge Angel LopeNo ratings yet
- Technical Circular: 2 ExchangeDocument16 pagesTechnical Circular: 2 Exchangepayman baharehNo ratings yet
- DG SetDocument3 pagesDG SetMaintenance Circle100% (2)
- BPCL Training ReportDocument34 pagesBPCL Training ReportVishalVaishNo ratings yet
- RSLinx Classic - 4.20.00 (Released 9 - 2020)Document7 pagesRSLinx Classic - 4.20.00 (Released 9 - 2020)MADMR MADMRNo ratings yet
- Product Guide o e w46dfDocument202 pagesProduct Guide o e w46dfИгорьNo ratings yet
- 628Document4 pages628sdiamanNo ratings yet
- KTA50 - Connecting RodDocument8 pagesKTA50 - Connecting RodSebastian Nicușor PărăoanuNo ratings yet
- Rapid Field Appraisal of Decentralization: Region 9Document40 pagesRapid Field Appraisal of Decentralization: Region 9Josh SchultzNo ratings yet
- Calculating ARIEL Lube RatesDocument2 pagesCalculating ARIEL Lube RateszhangjieNo ratings yet
- DB 40-20 PDFDocument22 pagesDB 40-20 PDFMahendra Asawale100% (1)
- Air Compressor (V Type)Document19 pagesAir Compressor (V Type)Anindya ChakrabortyNo ratings yet
- Ariel Compressor Balance SheetDocument130 pagesAriel Compressor Balance Sheetariel.garayNo ratings yet
- Cuckoo FormDocument1 pageCuckoo FormHaslindaNo ratings yet
- BBS Cable - Work OrderDocument16 pagesBBS Cable - Work OrderAntora HoqueNo ratings yet
- Decoder New 2013Document13 pagesDecoder New 2013viraj patelNo ratings yet
- Engine DataSheetDocument4 pagesEngine DataSheetLinda ApriyantiNo ratings yet
- Cigna Global Claim FormDocument3 pagesCigna Global Claim Formrsiabs marketingNo ratings yet
- Advisory Circular AC 66-08 v1.0: Part 66 Aircraft Engineer Licences - PrivilegesDocument54 pagesAdvisory Circular AC 66-08 v1.0: Part 66 Aircraft Engineer Licences - PrivilegesTGNo ratings yet
- Privacy Management PlanDocument16 pagesPrivacy Management PlanTGNo ratings yet
- Comparison Summary: Top HospitalDocument4 pagesComparison Summary: Top HospitalTGNo ratings yet
- Sunsuper Product Update: July 2021Document7 pagesSunsuper Product Update: July 2021TGNo ratings yet
- LM Unit IIDocument12 pagesLM Unit IImba departmentNo ratings yet
- Surgical Techniques CorpectomyDocument18 pagesSurgical Techniques CorpectomyJulian VargasNo ratings yet
- Donevan2017 PDFDocument25 pagesDonevan2017 PDFsmansa123No ratings yet
- CE Courses Accredited: CE Department Celebrated Science.01Document8 pagesCE Courses Accredited: CE Department Celebrated Science.01kiwipangNo ratings yet
- Questionnaire On Employee Welfare Activities at CELLO LTDDocument4 pagesQuestionnaire On Employee Welfare Activities at CELLO LTDhemantpahwa572No ratings yet
- Gamification-Based 3d Puzzle As An Effort To Improve Knowledge and Skills in Early Agencying Dental HealthMaintenance at Widuri Kindergarten, SemarangDocument4 pagesGamification-Based 3d Puzzle As An Effort To Improve Knowledge and Skills in Early Agencying Dental HealthMaintenance at Widuri Kindergarten, SemarangInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Circ15 2012 PDFDocument7 pagesCirc15 2012 PDFJanice Villaroya Jarales-YusonNo ratings yet
- Tugas PTB - Fahrie Febriyandi Taufan - 081911733053Document5 pagesTugas PTB - Fahrie Febriyandi Taufan - 081911733053fahrie febrianttNo ratings yet
- My Purpose of Study at Institute of Health and Nursing Australia (IHNA) Statement of Purpose (SOP)Document4 pagesMy Purpose of Study at Institute of Health and Nursing Australia (IHNA) Statement of Purpose (SOP)amir tamangNo ratings yet
- MIS 107 - Literature Review - by Dr. AbdullahDocument3 pagesMIS 107 - Literature Review - by Dr. AbdullahMunjir Abdullah 2112217030No ratings yet
- Principles of Internal and External FixationDocument111 pagesPrinciples of Internal and External FixationTrần KínhNo ratings yet
- Men's Health Australia - April 2016Document152 pagesMen's Health Australia - April 2016Robert FarrellNo ratings yet
- Stress Management Assignment NewDocument6 pagesStress Management Assignment NewRahul SahuNo ratings yet
- As ISO 10993.8-2003 Biological Evaluation of Medical Devices Selection and Qualification of Reference MateriaDocument8 pagesAs ISO 10993.8-2003 Biological Evaluation of Medical Devices Selection and Qualification of Reference MateriaSAI Global - APACNo ratings yet
- Angol AlapfokDocument5 pagesAngol AlapfokViktor Szaszkó100% (1)
- Altro - Vitamina C PureWay - C - WEBDocument2 pagesAltro - Vitamina C PureWay - C - WEBluigi cardanoNo ratings yet
- The ABO Blood Group System Revisited A Review and UpdateDocument12 pagesThe ABO Blood Group System Revisited A Review and UpdateAlifa Hasya Nadhira100% (2)
- View PublicationDocument16 pagesView PublicationpmilyNo ratings yet
- Corporate Reputation Management: Best Market Research Company India - Penn Schoen BerlandDocument5 pagesCorporate Reputation Management: Best Market Research Company India - Penn Schoen Berlandpsbsrch123No ratings yet
- T.burhan Fadillah (1812000072) TOEFL Preparation 2Document3 pagesT.burhan Fadillah (1812000072) TOEFL Preparation 2T.burhan FadillahNo ratings yet
- Co2 Gas MSDSDocument7 pagesCo2 Gas MSDSK SubramaniNo ratings yet
- Declaration of Erin EllisDocument4 pagesDeclaration of Erin EllisElizabeth Nolan BrownNo ratings yet
- Animal Teeth vs. Human Teeth PPT (Teacher Version)Document14 pagesAnimal Teeth vs. Human Teeth PPT (Teacher Version)Allison LeCoqNo ratings yet
- Harris Hematoxylin IrritanDocument7 pagesHarris Hematoxylin IrritanermaNo ratings yet
- Lecture Notes On NORMAL GAIT by DR M N SiddiquiDocument7 pagesLecture Notes On NORMAL GAIT by DR M N SiddiquiChandni P100% (1)
- Lions Young Leaders in Service Awards: Serve The CommunityDocument2 pagesLions Young Leaders in Service Awards: Serve The Communitykhaiwern98No ratings yet
- Cafcass Pathway Private Law - FinalDocument2 pagesCafcass Pathway Private Law - FinalMyGTMOAngel2009No ratings yet