Download as docx, pdf, or txt
You might also like
- Communicable Disease Nursing Ca1 July 2018 5 PDFDocument461 pagesCommunicable Disease Nursing Ca1 July 2018 5 PDFJordz Placi100% (3)
- Definition of InfectionDocument27 pagesDefinition of InfectionRenit AntoNo ratings yet
- Lecture 1 Infectious DiseasesDocument18 pagesLecture 1 Infectious DiseasesabdulrazaqNo ratings yet
- Infection Prevention (Including Hiv), Standard Precaution, Bio Waste ManagementDocument125 pagesInfection Prevention (Including Hiv), Standard Precaution, Bio Waste ManagementZhu Chen ChuanNo ratings yet
- Infection Prevention (Including Hiv), Standard Precaution, Bio Waste ManagementDocument125 pagesInfection Prevention (Including Hiv), Standard Precaution, Bio Waste ManagementZhu Chen ChuanNo ratings yet
- Icppt 170504055144 PDFDocument125 pagesIcppt 170504055144 PDFZhu Chen ChuanNo ratings yet
- Seminar ON: Infection Prevention (Including Hiv) and Standard Safety Measures, Bio - Medical Waste ManagementDocument24 pagesSeminar ON: Infection Prevention (Including Hiv) and Standard Safety Measures, Bio - Medical Waste ManagementTHONDYNALUNo ratings yet
- Communicable Diseases 2Document8 pagesCommunicable Diseases 2martinaNo ratings yet
- Infection Control in Health Care SettingsDocument27 pagesInfection Control in Health Care SettingsSondre Sverd Rekdal100% (1)
- Mechanisms of Transmission of Pathogenic Organisms in The Health Care Setting and Strategies For Prevention and ControlDocument45 pagesMechanisms of Transmission of Pathogenic Organisms in The Health Care Setting and Strategies For Prevention and Controlbenq35No ratings yet
- Infection Control - Classroom TeachingDocument16 pagesInfection Control - Classroom TeachingRDi JNo ratings yet
- Infection PreventionDocument38 pagesInfection PreventionAmanda ScarletNo ratings yet
- 4 Communicable Disease NursingDocument44 pages4 Communicable Disease NursingDaryl Emmanuel ChuaNo ratings yet
- Communicable and Non-Communicable DiseaseDocument44 pagesCommunicable and Non-Communicable DiseaseSajida Bibi NoonariNo ratings yet
- CD2 NDDocument51 pagesCD2 NDNhelia Santos BañagaNo ratings yet
- Infectious DiseasesDocument10 pagesInfectious DiseasesAgnes Marie RendonNo ratings yet
- Infection ControlDocument111 pagesInfection ControlCristyn BMNo ratings yet
- 1 Lect Surgery Infection Controle-Adobe PDFDocument56 pages1 Lect Surgery Infection Controle-Adobe PDFNadeem AlawashrehNo ratings yet
- Introduction To Epidemiology of Infection Diseases PDFDocument17 pagesIntroduction To Epidemiology of Infection Diseases PDFRovaidKhanNo ratings yet
- Conceptualize Infection and ImmunityDocument5 pagesConceptualize Infection and Immunityالمثنى العمريNo ratings yet
- Chapter 13Document32 pagesChapter 13Kat KatNo ratings yet
- CHN Final TopicsDocument52 pagesCHN Final TopicsMary Ann SacramentoNo ratings yet
- AsepsisDocument7 pagesAsepsisWarrenSandovalNo ratings yet
- University of Perpetual Help System Laguna Dr. Jose G. Tamayo Medical University College of NursingDocument68 pagesUniversity of Perpetual Help System Laguna Dr. Jose G. Tamayo Medical University College of NursingjessamariefajardoNo ratings yet
- Intro To Communicable Diseases-1Document101 pagesIntro To Communicable Diseases-1Natukunda DianahNo ratings yet
- Hospital Hygiene and Infection ControlDocument8 pagesHospital Hygiene and Infection ControlUday KumarNo ratings yet
- d1 InfectionDocument56 pagesd1 InfectionTamar GrdzelishviliNo ratings yet
- ZohaibDocument6 pagesZohaibMUHAMMAD ZOHAIBNo ratings yet
- Communicable DiseasesDocument25 pagesCommunicable DiseasesMaria Jubel Maceda Cabahug100% (1)
- Unit 2 Preventive Pharmacy 1Document44 pagesUnit 2 Preventive Pharmacy 1tshradha2003No ratings yet
- The Chain of Infection What Is An Infection?: Peel Public Health - Take Control Guide 2013Document5 pagesThe Chain of Infection What Is An Infection?: Peel Public Health - Take Control Guide 2013joaojoaomendes6846No ratings yet
- COMMUNICABLE AND NCDsDocument147 pagesCOMMUNICABLE AND NCDschristine gisembaNo ratings yet
- Introduction To Tropical MedicineDocument5 pagesIntroduction To Tropical MedicineisaacturyabikirizaNo ratings yet
- Pandemic of COVID-19Document25 pagesPandemic of COVID-19Arpita MohapatraNo ratings yet
- Infection Control and Safety MeasuresDocument29 pagesInfection Control and Safety MeasuresAlma Susan100% (2)
- Communicable Disease Nursing Ca1 July 2018 5Document461 pagesCommunicable Disease Nursing Ca1 July 2018 5Jordz PlaciNo ratings yet
- Infection Control With BMWDocument19 pagesInfection Control With BMWgouri debNo ratings yet
- Chain of InfectionDocument34 pagesChain of InfectionJohn Drazen T SeguiNo ratings yet
- SOP For Hospital Infection Control-1Document33 pagesSOP For Hospital Infection Control-1Anmol GhaiNo ratings yet
- Transmission of Food ContaminationDocument3 pagesTransmission of Food ContaminationShaista MahvishNo ratings yet
- Eddy MTCDocument61 pagesEddy MTCkhelianderrick81No ratings yet
- Historical Background and Trends in The Treatment of Infectious DiseasesDocument50 pagesHistorical Background and Trends in The Treatment of Infectious DiseasesJoeven HilarioNo ratings yet
- Communicable-D FINAL 2021-1-9Document16 pagesCommunicable-D FINAL 2021-1-9Shimaa KashefNo ratings yet
- Respiratory Infections ....Document195 pagesRespiratory Infections ....Poorny PurushothNo ratings yet
- Stages of Infection 2Document7 pagesStages of Infection 2Karren Taquiqui PleteNo ratings yet
- Community Health Nursing IiDocument13 pagesCommunity Health Nursing Iikimfrancess55No ratings yet
- INFECTIOUS PROC-WPS OfficeDocument6 pagesINFECTIOUS PROC-WPS OfficeNifemi AketanNo ratings yet
- Peter John P. Gono, RN, ManDocument22 pagesPeter John P. Gono, RN, ManGardoke Jr. M. LansonNo ratings yet
- Terminologies 1 ClassDocument55 pagesTerminologies 1 Classrakshayadahal9No ratings yet
- 15 Communicable Disease - Health Risk and PreventionDocument81 pages15 Communicable Disease - Health Risk and PreventionsyakirohNo ratings yet
- Communicable DiseaseDocument19 pagesCommunicable DiseaseRwapembe StephenNo ratings yet
- Guideline Prevention of Communicable Diseases RCHD 1 Concepts of Communicable DiseasesDocument4 pagesGuideline Prevention of Communicable Diseases RCHD 1 Concepts of Communicable DiseasesGerald HanNo ratings yet
- Infection Control: IntroductionDocument17 pagesInfection Control: Introductionsuman gupta100% (1)
- Communicable DiseasesDocument292 pagesCommunicable DiseasesBL AR100% (2)
- The Patient From Becoming Re-Infected and The Infection From Spreading To Other PersonsDocument13 pagesThe Patient From Becoming Re-Infected and The Infection From Spreading To Other PersonshahahahaaaaaaaNo ratings yet
- Asepsis and Infection PreventionDocument31 pagesAsepsis and Infection PreventionPamela Ria HensonNo ratings yet
- Contagious Diseases: The Science, History, and Future of Epidemics. From Ancient Plagues to Modern Pandemics, How to Stay Ahead of a Global Health CrisisFrom EverandContagious Diseases: The Science, History, and Future of Epidemics. From Ancient Plagues to Modern Pandemics, How to Stay Ahead of a Global Health CrisisNo ratings yet
- The Big Book of Infectious Disease Trivia: Everything You Ever Wanted to Know about the World's Worst Pandemics, Epidemics and DiseasesFrom EverandThe Big Book of Infectious Disease Trivia: Everything You Ever Wanted to Know about the World's Worst Pandemics, Epidemics and DiseasesNo ratings yet
- Viral Vistas: Insights into Infectious Diseases: The Invisible War: Decoding the Game of Hide and Seek with PathogensFrom EverandViral Vistas: Insights into Infectious Diseases: The Invisible War: Decoding the Game of Hide and Seek with PathogensNo ratings yet
- Snakes Are Needed in Our World For ManyDocument18 pagesSnakes Are Needed in Our World For Manyapi-600442421No ratings yet
- Digital Studio: Course DescriptionDocument12 pagesDigital Studio: Course DescriptionCornNo ratings yet
- What Is A Competent TeacherDocument2 pagesWhat Is A Competent TeacherJoy Dacuan100% (2)
- Final Project 2nd Semester 2019ADocument3 pagesFinal Project 2nd Semester 2019AEsthr GaNo ratings yet
- Tinea CapitisDocument7 pagesTinea CapitiswinNo ratings yet
- Lesson Plan Death CareDocument19 pagesLesson Plan Death CareLoma Waghmare (Jadhav)No ratings yet
- Junsay Btths-ClaygoDocument8 pagesJunsay Btths-ClaygoShefhannie CabanusNo ratings yet
- (April 2020) : Is The Indication Appropriate For A Doac?Document1 page(April 2020) : Is The Indication Appropriate For A Doac?SNo ratings yet
- LECTURE ExodontiaDocument113 pagesLECTURE ExodontiaNuzhat Noor Ayesha89% (9)
- Egyptian Stories - Egypt Bottled Water - UNSAFEDocument4 pagesEgyptian Stories - Egypt Bottled Water - UNSAFEtefovNo ratings yet
- Psychiatric Nursing FCDocument8 pagesPsychiatric Nursing FCdhodejunlNo ratings yet
- Approaches To The Study of Hypnotic Dreams: Charles T. TartDocument1 pageApproaches To The Study of Hypnotic Dreams: Charles T. TartIno MoxoNo ratings yet
- Prac Res Q2 Module 8Document12 pagesPrac Res Q2 Module 8Benicel Lane De VeraNo ratings yet
- The Dynamics of Psychological Security-Insecurity: Brooklyn CollegeDocument15 pagesThe Dynamics of Psychological Security-Insecurity: Brooklyn Collegetanisya aurely12No ratings yet
- A Study On Work From Home, Motivation & Productivity of Employees in Indian Population During COVID-19 PandemicDocument15 pagesA Study On Work From Home, Motivation & Productivity of Employees in Indian Population During COVID-19 Pandemicمعن الفاعوريNo ratings yet
- Alternative Work Scheme vs. On Site Labor PhilippinesDocument3 pagesAlternative Work Scheme vs. On Site Labor PhilippinesLayaDioknoNo ratings yet
- Presentation: Submitted To Ma'am Ayesha Sadaf Subject Media & SocietyDocument23 pagesPresentation: Submitted To Ma'am Ayesha Sadaf Subject Media & Societylaiba asadNo ratings yet
- Assignment Ni Ayang Sa TechnologyDocument2 pagesAssignment Ni Ayang Sa TechnologyJohn Mico MacatigbacNo ratings yet
- Cone-Beam Computed Tomography Vs Conventional Radiography in Visualization of Maxillary Impacted-Canine Localization A Systematic Review of Comparative Studies.Document11 pagesCone-Beam Computed Tomography Vs Conventional Radiography in Visualization of Maxillary Impacted-Canine Localization A Systematic Review of Comparative Studies.bichocorralNo ratings yet
- Final Exam Schedule-StudentsDocument2 pagesFinal Exam Schedule-StudentsBLESSEDNo ratings yet
- KIS MYP Summative Assessment - Grade 7 C ADocument4 pagesKIS MYP Summative Assessment - Grade 7 C AAahan ShahNo ratings yet
- Human Ass (Point)Document4 pagesHuman Ass (Point)chuojx-jb23No ratings yet
- dm2019-0365 Interim Guidelines On LNS SQDocument8 pagesdm2019-0365 Interim Guidelines On LNS SQMary Joy GaloloNo ratings yet
- Thanathbhorn@knc - Ac.th: 2017 ANPOR ANNUAL ConferenceDocument8 pagesThanathbhorn@knc - Ac.th: 2017 ANPOR ANNUAL ConferenceRebecaDiasNo ratings yet
- Project PrimaryDocument7 pagesProject PrimaryLisanwork HonseboNo ratings yet
- Anthropology Unit 4Document8 pagesAnthropology Unit 4amaniNo ratings yet
- Clinical 3 Dump Dusting Chimozi 3Document8 pagesClinical 3 Dump Dusting Chimozi 3Miriward ZimbaNo ratings yet
- Chapter 2 - Market Analysis - Group 2Document26 pagesChapter 2 - Market Analysis - Group 2Allan AntonioNo ratings yet
- Marram Email BrochureDocument5 pagesMarram Email Brochurethangth1986No ratings yet
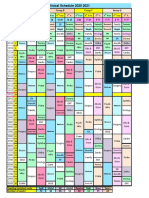
- R Schedule 2020 2021Document1 pageR Schedule 2020 2021Mohammed AhmedNo ratings yet