
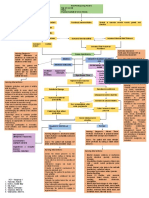
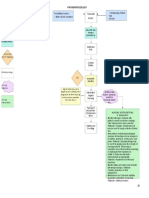
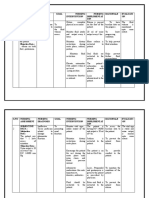
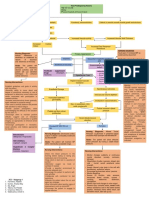
Management: Diagnosis
Management: Diagnosis
You might also like
- NRNP 6635 Final ExamDocument17 pagesNRNP 6635 Final Examerick kanyiNo ratings yet
- Manual of Standards and Guidelines On The Management of The Hospital Emergency Department 2nd Ed 2022Document169 pagesManual of Standards and Guidelines On The Management of The Hospital Emergency Department 2nd Ed 2022shane natividad100% (1)
- Drug Study Heparin and FenylDocument4 pagesDrug Study Heparin and FenylAnisa Jamito75% (4)
- Hemodynamic Monitoring of The Critical PatientDocument58 pagesHemodynamic Monitoring of The Critical PatientScribdTranslationsNo ratings yet
- Risk For Decreased Cardiac Tissue PerfusionDocument3 pagesRisk For Decreased Cardiac Tissue PerfusionKarina MadriagaNo ratings yet
- CARE PLAN Urinary ObstructionDocument2 pagesCARE PLAN Urinary Obstructionjinsi georgeNo ratings yet
- Rangkuman CCS 1Document16 pagesRangkuman CCS 1Tesis Maruli Tua SianiparNo ratings yet
- Intensivist Use of Hand-Carried Ultrasonography To Measure IVC Collapsibility in Estimating Intravascular Volume Status: Correlations With CVPDocument2 pagesIntensivist Use of Hand-Carried Ultrasonography To Measure IVC Collapsibility in Estimating Intravascular Volume Status: Correlations With CVPArjun RajagopalanNo ratings yet
- Invasive Monitoring in The Intensive Care UnitDocument6 pagesInvasive Monitoring in The Intensive Care UnitArjunNo ratings yet
- Angiography (Cardiac Catherization) : Patient Teaching/preparationDocument2 pagesAngiography (Cardiac Catherization) : Patient Teaching/preparationpsyNo ratings yet
- Combinepdf 3Document95 pagesCombinepdf 3paruNo ratings yet
- Salvi Et Al 2019 Noninvasive Estimation of Aortic Stiffness Through Different ApproachesDocument13 pagesSalvi Et Al 2019 Noninvasive Estimation of Aortic Stiffness Through Different ApproachesLilia RadjefNo ratings yet
- Akut Limb IskemikDocument31 pagesAkut Limb IskemikLaluMuhammadSabarSetiawanNo ratings yet
- Renal Trauma: EAU Guideline 2020 & WSES-AAST GuidelinesDocument33 pagesRenal Trauma: EAU Guideline 2020 & WSES-AAST Guidelinesduo_ngoNo ratings yet
- Early Mobilization in Aneurysmal Subarachnoid Hemorrhage Accelerates The Recovery of FunctionDocument2 pagesEarly Mobilization in Aneurysmal Subarachnoid Hemorrhage Accelerates The Recovery of FunctionKawey CaiNo ratings yet
- Appendix A Nursing Management TablesDocument27 pagesAppendix A Nursing Management Tablesba.ramirez11No ratings yet
- Revascularization in Chronic Coronary Syndromes - Dr. A. Fauzi Yahya, SP - JPDocument46 pagesRevascularization in Chronic Coronary Syndromes - Dr. A. Fauzi Yahya, SP - JPGianti wulandariNo ratings yet
- Management of OliguriaDocument14 pagesManagement of OliguriaAhmed El-MalkyNo ratings yet
- Acute Kidney Injury Prevention & Early Detection With Novel BiomarkersDocument37 pagesAcute Kidney Injury Prevention & Early Detection With Novel Biomarkerssapphire_asaphNo ratings yet
- DIALYSIS Brochure - RAMOSDocument2 pagesDIALYSIS Brochure - RAMOSJan Clarisse RamosNo ratings yet
- Dynamic Practice Guidelines For Emergency General SurgeryDocument19 pagesDynamic Practice Guidelines For Emergency General SurgeryJolaine ValloNo ratings yet
- Central Venous Pressure 55Document2 pagesCentral Venous Pressure 55Pamipam100% (1)
- Procedure File M.S.NDocument11 pagesProcedure File M.S.NShalabh JoharyNo ratings yet
- ShitDocument1 pageShitENKELI VALDECANTOSNo ratings yet
- Algorithms For IV Fluid Therapy in Children and Young People in Hospital Set of 6 PDF 2190274957 PDFDocument6 pagesAlgorithms For IV Fluid Therapy in Children and Young People in Hospital Set of 6 PDF 2190274957 PDFFurqon AfandriNo ratings yet
- Physiologic MonitoringDocument4 pagesPhysiologic MonitoringAimie DagaleaNo ratings yet
- Blood Test - LFTDocument4 pagesBlood Test - LFTAbhi NikamNo ratings yet
- LidocaineDocument2 pagesLidocaineRomwella May AlgoNo ratings yet
- Q Tip TestDocument4 pagesQ Tip TestAdelia MakmurNo ratings yet
- Hemorrhage NCPDocument4 pagesHemorrhage NCPElishaNo ratings yet
- Hypovolemic Shock Concept MapDocument1 pageHypovolemic Shock Concept MapJM AsentistaNo ratings yet
- Neurosurgery Research PaperDocument7 pagesNeurosurgery Research PaperAhmadNo ratings yet
- Minimally Invasive Cardiac Output by BJApdfDocument6 pagesMinimally Invasive Cardiac Output by BJApdfblessing akataNo ratings yet
- Incomplete Abortion PATHODocument2 pagesIncomplete Abortion PATHOaprilkate banagodosNo ratings yet
- Haemodynamic Monitoring: WWW - Vygon.co - UkDocument12 pagesHaemodynamic Monitoring: WWW - Vygon.co - UkJuita yuliarniNo ratings yet
- R02Y2002N04A0219Document7 pagesR02Y2002N04A0219gustiNo ratings yet
- NCP of GlomerularnephritisDocument6 pagesNCP of GlomerularnephritisSimran JosanNo ratings yet
- Byecsu SurgDocument22 pagesByecsu SurgBea Y. Bas-ongNo ratings yet
- euae156Document3 pageseuae156mauricecor22No ratings yet
- Drug StudyDocument10 pagesDrug StudyJeraldine GumpalNo ratings yet
- 9 - Role of Non InvasiveDocument46 pages9 - Role of Non InvasiveHavara Kausar AkbarNo ratings yet
- NCPDocument9 pagesNCPKarell Eunice Estrellado Gutierrez100% (1)
- Pioquinto (Rot 2 NCP)Document4 pagesPioquinto (Rot 2 NCP)Ghianx Carlox PioquintoxNo ratings yet
- Neurogenic Shock Concept MapDocument1 pageNeurogenic Shock Concept MapJessa Mae Alforque Asentista0% (1)
- Echo ReportDocument2 pagesEcho ReportweareweNo ratings yet
- Non-Operating Room Anesthesia: April 2017Document26 pagesNon-Operating Room Anesthesia: April 2017Eolia EffendiNo ratings yet
- Acute Kidney Injury W/ Hyperkalemia NCPDocument5 pagesAcute Kidney Injury W/ Hyperkalemia NCPMyrvic Ortiz La OrdenNo ratings yet
- EP Club - Basic Holter MonitoringDocument29 pagesEP Club - Basic Holter Monitoringzakiyyatul aflakhaNo ratings yet
- 3C3 Subgroup1 M11 PT1Document1 page3C3 Subgroup1 M11 PT1ENKELI VALDECANTOSNo ratings yet
- 12-Adult Post Resuscitation Care Algorithm 2021Document1 page12-Adult Post Resuscitation Care Algorithm 2021khaledNo ratings yet
- Advanced Hemodynamic Monitoring: Fahmi Agnesha EdwinDocument28 pagesAdvanced Hemodynamic Monitoring: Fahmi Agnesha EdwinfahmiNo ratings yet
- PDF Passive Leg Raise PLR Test Stroke Volume Index SviDocument3 pagesPDF Passive Leg Raise PLR Test Stroke Volume Index SviNama ManaNo ratings yet
- Current State of Noninvasive, Continuous.12 PDFDocument7 pagesCurrent State of Noninvasive, Continuous.12 PDFFIA SlotNo ratings yet
- 273 Full PDFDocument4 pages273 Full PDFSubas SharmaNo ratings yet
- DRUG STUDY ICU and ACSDocument22 pagesDRUG STUDY ICU and ACSSheila Mae ReyesNo ratings yet
- College of Nursing: Maternal and Child NursingDocument2 pagesCollege of Nursing: Maternal and Child NursingLeahmore Amor Padayhag AlineaNo ratings yet
- Perdarahan Saluran Cerna Bagian BawahDocument33 pagesPerdarahan Saluran Cerna Bagian BawahGiyani LiberthiNo ratings yet
- Starling Published StudiesDocument4 pagesStarling Published Studiesjobbathebutty mamamaNo ratings yet
- Pioquinto Rot 2 (Sic)Document10 pagesPioquinto Rot 2 (Sic)Ghianx Carlox PioquintoxNo ratings yet
- NCPDocument3 pagesNCPSteffi MurielNo ratings yet
- Sirosis Hepatis Dan KomplikasiDocument36 pagesSirosis Hepatis Dan KomplikasiMuhammad HafizdNo ratings yet
- Management: DiagnosisDocument6 pagesManagement: DiagnosisAhmed El-MalkyNo ratings yet
- Sciatic Nerve: by Name: Ahmed Abdalla Mahmoud Salem ID: 052608064Document35 pagesSciatic Nerve: by Name: Ahmed Abdalla Mahmoud Salem ID: 052608064Ahmed El-MalkyNo ratings yet
- Management of OliguriaDocument14 pagesManagement of OliguriaAhmed El-MalkyNo ratings yet
- Sodium Channels: Name: Sara Abdallah Almalky ID: 555 Tutor: Dr. Samar Al-GhetnyDocument5 pagesSodium Channels: Name: Sara Abdallah Almalky ID: 555 Tutor: Dr. Samar Al-GhetnyAhmed El-MalkyNo ratings yet
- Plasma Cells: DefinitionDocument4 pagesPlasma Cells: DefinitionAhmed El-MalkyNo ratings yet
- Ent History Taking and Examination-1Document16 pagesEnt History Taking and Examination-1Jyotirmayee100% (6)
- Reviewer - Quick NotesDocument51 pagesReviewer - Quick NotesNorvie Kim MagdaongNo ratings yet
- Developing Review QuestionsDocument2 pagesDeveloping Review QuestionsKlaudia D. KarboviakNo ratings yet
- University of Basra Al-Zahra College of Medicine First ClassDocument11 pagesUniversity of Basra Al-Zahra College of Medicine First Classعـَــٻاس مَـــشتاق عـَــليNo ratings yet
- Pe SbaDocument30 pagesPe Sbaselina fraser100% (1)
- Day 14 NCM 109 FE AdolescentDocument57 pagesDay 14 NCM 109 FE AdolescentSheena Patricia ArasulaNo ratings yet
- Pathology of Skeletal SystemDocument65 pagesPathology of Skeletal SystemFirda S SalsabilaNo ratings yet
- Nclex Random Fact To StudyDocument431 pagesNclex Random Fact To StudyNeko Neko100% (1)
- Marshall Community Letter: Person at Middle School Tests Positive For CoronavirusDocument1 pageMarshall Community Letter: Person at Middle School Tests Positive For CoronavirusJoy M. HosfordNo ratings yet
- Nursing Care Plan Hyperthermia (Cap)Document2 pagesNursing Care Plan Hyperthermia (Cap)Algen UbasaNo ratings yet
- Risk Based Food Inspection SystemDocument52 pagesRisk Based Food Inspection Systemthanveer789No ratings yet
- The Exercise PrescriptionDocument68 pagesThe Exercise PrescriptionDario MoralesNo ratings yet
- REVISION Unit 4 - Unit 6: A Sore Throat A Headache A Stomach AcheDocument4 pagesREVISION Unit 4 - Unit 6: A Sore Throat A Headache A Stomach AcheNguyễn Hằng NgaNo ratings yet
- Kapalbhati PDFDocument2 pagesKapalbhati PDFRahul MishraNo ratings yet
- Anaplastic Thyroid CancerDocument40 pagesAnaplastic Thyroid Cancershita febrianaNo ratings yet
- Therapeutic Roles of Medicinal Herbs For The Treatment of Jaundice and Hepatitis BDocument7 pagesTherapeutic Roles of Medicinal Herbs For The Treatment of Jaundice and Hepatitis BEditor IJTSRDNo ratings yet
- Geriatric Nursing: Theories of AgingDocument4 pagesGeriatric Nursing: Theories of AgingNikkaDablioNo ratings yet
- Klayman Lawsuit Against ChinaDocument24 pagesKlayman Lawsuit Against ChinaLaw&Crime100% (5)
- QUESTIONNAIRE in Business ProfilingDocument4 pagesQUESTIONNAIRE in Business ProfilingLilibeth AgdamagNo ratings yet
- VNSG 1409 - Exam 3Document24 pagesVNSG 1409 - Exam 3luna nguyenNo ratings yet
- The Final FRCA Short Answer Questions - A Practical Study Guide (PDFDrive)Document348 pagesThe Final FRCA Short Answer Questions - A Practical Study Guide (PDFDrive)Andreea0% (1)
- APPENDICITISDocument6 pagesAPPENDICITISJAN ACCEL PAGADUANNo ratings yet
- Related Teenshealth Links: Health Problems SeriesDocument13 pagesRelated Teenshealth Links: Health Problems SeriesMario BadayosNo ratings yet
- Patient Classification & AssignmentDocument37 pagesPatient Classification & AssignmentAkhila UsNo ratings yet
- Supernumerary Teeth: Review of The Literature and A Survey of 152 CasesDocument11 pagesSupernumerary Teeth: Review of The Literature and A Survey of 152 CasesfatimahNo ratings yet
- African Americans Struggle With Disproportionate COVID Death TollDocument3 pagesAfrican Americans Struggle With Disproportionate COVID Death TollRodney BrooksNo ratings yet
- Oxford Handbook of Geriatric Medicine 3nbsped 0198738382 9780198738381 CompressDocument753 pagesOxford Handbook of Geriatric Medicine 3nbsped 0198738382 9780198738381 CompressNemer Isaeed100% (3)
- HLTH9 - 3Q First Aid For Common Unintentional InjuriesDocument5 pagesHLTH9 - 3Q First Aid For Common Unintentional InjuriesNardriel Kinsley TrongcosoNo ratings yet
























































































Download as docx, pdf, or txt
You might also like
- NRNP 6635 Final ExamDocument17 pagesNRNP 6635 Final Examerick kanyiNo ratings yet
- Manual of Standards and Guidelines On The Management of The Hospital Emergency Department 2nd Ed 2022Document169 pagesManual of Standards and Guidelines On The Management of The Hospital Emergency Department 2nd Ed 2022shane natividad100% (1)
- Drug Study Heparin and FenylDocument4 pagesDrug Study Heparin and FenylAnisa Jamito75% (4)
- Hemodynamic Monitoring of The Critical PatientDocument58 pagesHemodynamic Monitoring of The Critical PatientScribdTranslationsNo ratings yet
- Risk For Decreased Cardiac Tissue PerfusionDocument3 pagesRisk For Decreased Cardiac Tissue PerfusionKarina MadriagaNo ratings yet
- CARE PLAN Urinary ObstructionDocument2 pagesCARE PLAN Urinary Obstructionjinsi georgeNo ratings yet
- Rangkuman CCS 1Document16 pagesRangkuman CCS 1Tesis Maruli Tua SianiparNo ratings yet
- Intensivist Use of Hand-Carried Ultrasonography To Measure IVC Collapsibility in Estimating Intravascular Volume Status: Correlations With CVPDocument2 pagesIntensivist Use of Hand-Carried Ultrasonography To Measure IVC Collapsibility in Estimating Intravascular Volume Status: Correlations With CVPArjun RajagopalanNo ratings yet
- Invasive Monitoring in The Intensive Care UnitDocument6 pagesInvasive Monitoring in The Intensive Care UnitArjunNo ratings yet
- Angiography (Cardiac Catherization) : Patient Teaching/preparationDocument2 pagesAngiography (Cardiac Catherization) : Patient Teaching/preparationpsyNo ratings yet
- Combinepdf 3Document95 pagesCombinepdf 3paruNo ratings yet
- Salvi Et Al 2019 Noninvasive Estimation of Aortic Stiffness Through Different ApproachesDocument13 pagesSalvi Et Al 2019 Noninvasive Estimation of Aortic Stiffness Through Different ApproachesLilia RadjefNo ratings yet
- Akut Limb IskemikDocument31 pagesAkut Limb IskemikLaluMuhammadSabarSetiawanNo ratings yet
- Renal Trauma: EAU Guideline 2020 & WSES-AAST GuidelinesDocument33 pagesRenal Trauma: EAU Guideline 2020 & WSES-AAST Guidelinesduo_ngoNo ratings yet
- Early Mobilization in Aneurysmal Subarachnoid Hemorrhage Accelerates The Recovery of FunctionDocument2 pagesEarly Mobilization in Aneurysmal Subarachnoid Hemorrhage Accelerates The Recovery of FunctionKawey CaiNo ratings yet
- Appendix A Nursing Management TablesDocument27 pagesAppendix A Nursing Management Tablesba.ramirez11No ratings yet
- Revascularization in Chronic Coronary Syndromes - Dr. A. Fauzi Yahya, SP - JPDocument46 pagesRevascularization in Chronic Coronary Syndromes - Dr. A. Fauzi Yahya, SP - JPGianti wulandariNo ratings yet
- Management of OliguriaDocument14 pagesManagement of OliguriaAhmed El-MalkyNo ratings yet
- Acute Kidney Injury Prevention & Early Detection With Novel BiomarkersDocument37 pagesAcute Kidney Injury Prevention & Early Detection With Novel Biomarkerssapphire_asaphNo ratings yet
- DIALYSIS Brochure - RAMOSDocument2 pagesDIALYSIS Brochure - RAMOSJan Clarisse RamosNo ratings yet
- Dynamic Practice Guidelines For Emergency General SurgeryDocument19 pagesDynamic Practice Guidelines For Emergency General SurgeryJolaine ValloNo ratings yet
- Central Venous Pressure 55Document2 pagesCentral Venous Pressure 55Pamipam100% (1)
- Procedure File M.S.NDocument11 pagesProcedure File M.S.NShalabh JoharyNo ratings yet
- ShitDocument1 pageShitENKELI VALDECANTOSNo ratings yet
- Algorithms For IV Fluid Therapy in Children and Young People in Hospital Set of 6 PDF 2190274957 PDFDocument6 pagesAlgorithms For IV Fluid Therapy in Children and Young People in Hospital Set of 6 PDF 2190274957 PDFFurqon AfandriNo ratings yet
- Physiologic MonitoringDocument4 pagesPhysiologic MonitoringAimie DagaleaNo ratings yet
- Blood Test - LFTDocument4 pagesBlood Test - LFTAbhi NikamNo ratings yet
- LidocaineDocument2 pagesLidocaineRomwella May AlgoNo ratings yet
- Q Tip TestDocument4 pagesQ Tip TestAdelia MakmurNo ratings yet
- Hemorrhage NCPDocument4 pagesHemorrhage NCPElishaNo ratings yet
- Hypovolemic Shock Concept MapDocument1 pageHypovolemic Shock Concept MapJM AsentistaNo ratings yet
- Neurosurgery Research PaperDocument7 pagesNeurosurgery Research PaperAhmadNo ratings yet
- Minimally Invasive Cardiac Output by BJApdfDocument6 pagesMinimally Invasive Cardiac Output by BJApdfblessing akataNo ratings yet
- Incomplete Abortion PATHODocument2 pagesIncomplete Abortion PATHOaprilkate banagodosNo ratings yet
- Haemodynamic Monitoring: WWW - Vygon.co - UkDocument12 pagesHaemodynamic Monitoring: WWW - Vygon.co - UkJuita yuliarniNo ratings yet
- R02Y2002N04A0219Document7 pagesR02Y2002N04A0219gustiNo ratings yet
- NCP of GlomerularnephritisDocument6 pagesNCP of GlomerularnephritisSimran JosanNo ratings yet
- Byecsu SurgDocument22 pagesByecsu SurgBea Y. Bas-ongNo ratings yet
- euae156Document3 pageseuae156mauricecor22No ratings yet
- Drug StudyDocument10 pagesDrug StudyJeraldine GumpalNo ratings yet
- 9 - Role of Non InvasiveDocument46 pages9 - Role of Non InvasiveHavara Kausar AkbarNo ratings yet
- NCPDocument9 pagesNCPKarell Eunice Estrellado Gutierrez100% (1)
- Pioquinto (Rot 2 NCP)Document4 pagesPioquinto (Rot 2 NCP)Ghianx Carlox PioquintoxNo ratings yet
- Neurogenic Shock Concept MapDocument1 pageNeurogenic Shock Concept MapJessa Mae Alforque Asentista0% (1)
- Echo ReportDocument2 pagesEcho ReportweareweNo ratings yet
- Non-Operating Room Anesthesia: April 2017Document26 pagesNon-Operating Room Anesthesia: April 2017Eolia EffendiNo ratings yet
- Acute Kidney Injury W/ Hyperkalemia NCPDocument5 pagesAcute Kidney Injury W/ Hyperkalemia NCPMyrvic Ortiz La OrdenNo ratings yet
- EP Club - Basic Holter MonitoringDocument29 pagesEP Club - Basic Holter Monitoringzakiyyatul aflakhaNo ratings yet
- 3C3 Subgroup1 M11 PT1Document1 page3C3 Subgroup1 M11 PT1ENKELI VALDECANTOSNo ratings yet
- 12-Adult Post Resuscitation Care Algorithm 2021Document1 page12-Adult Post Resuscitation Care Algorithm 2021khaledNo ratings yet
- Advanced Hemodynamic Monitoring: Fahmi Agnesha EdwinDocument28 pagesAdvanced Hemodynamic Monitoring: Fahmi Agnesha EdwinfahmiNo ratings yet
- PDF Passive Leg Raise PLR Test Stroke Volume Index SviDocument3 pagesPDF Passive Leg Raise PLR Test Stroke Volume Index SviNama ManaNo ratings yet
- Current State of Noninvasive, Continuous.12 PDFDocument7 pagesCurrent State of Noninvasive, Continuous.12 PDFFIA SlotNo ratings yet
- 273 Full PDFDocument4 pages273 Full PDFSubas SharmaNo ratings yet
- DRUG STUDY ICU and ACSDocument22 pagesDRUG STUDY ICU and ACSSheila Mae ReyesNo ratings yet
- College of Nursing: Maternal and Child NursingDocument2 pagesCollege of Nursing: Maternal and Child NursingLeahmore Amor Padayhag AlineaNo ratings yet
- Perdarahan Saluran Cerna Bagian BawahDocument33 pagesPerdarahan Saluran Cerna Bagian BawahGiyani LiberthiNo ratings yet
- Starling Published StudiesDocument4 pagesStarling Published Studiesjobbathebutty mamamaNo ratings yet
- Pioquinto Rot 2 (Sic)Document10 pagesPioquinto Rot 2 (Sic)Ghianx Carlox PioquintoxNo ratings yet
- NCPDocument3 pagesNCPSteffi MurielNo ratings yet
- Sirosis Hepatis Dan KomplikasiDocument36 pagesSirosis Hepatis Dan KomplikasiMuhammad HafizdNo ratings yet
- Management: DiagnosisDocument6 pagesManagement: DiagnosisAhmed El-MalkyNo ratings yet
- Sciatic Nerve: by Name: Ahmed Abdalla Mahmoud Salem ID: 052608064Document35 pagesSciatic Nerve: by Name: Ahmed Abdalla Mahmoud Salem ID: 052608064Ahmed El-MalkyNo ratings yet
- Management of OliguriaDocument14 pagesManagement of OliguriaAhmed El-MalkyNo ratings yet
- Sodium Channels: Name: Sara Abdallah Almalky ID: 555 Tutor: Dr. Samar Al-GhetnyDocument5 pagesSodium Channels: Name: Sara Abdallah Almalky ID: 555 Tutor: Dr. Samar Al-GhetnyAhmed El-MalkyNo ratings yet
- Plasma Cells: DefinitionDocument4 pagesPlasma Cells: DefinitionAhmed El-MalkyNo ratings yet
- Ent History Taking and Examination-1Document16 pagesEnt History Taking and Examination-1Jyotirmayee100% (6)
- Reviewer - Quick NotesDocument51 pagesReviewer - Quick NotesNorvie Kim MagdaongNo ratings yet
- Developing Review QuestionsDocument2 pagesDeveloping Review QuestionsKlaudia D. KarboviakNo ratings yet
- University of Basra Al-Zahra College of Medicine First ClassDocument11 pagesUniversity of Basra Al-Zahra College of Medicine First Classعـَــٻاس مَـــشتاق عـَــليNo ratings yet
- Pe SbaDocument30 pagesPe Sbaselina fraser100% (1)
- Day 14 NCM 109 FE AdolescentDocument57 pagesDay 14 NCM 109 FE AdolescentSheena Patricia ArasulaNo ratings yet
- Pathology of Skeletal SystemDocument65 pagesPathology of Skeletal SystemFirda S SalsabilaNo ratings yet
- Nclex Random Fact To StudyDocument431 pagesNclex Random Fact To StudyNeko Neko100% (1)
- Marshall Community Letter: Person at Middle School Tests Positive For CoronavirusDocument1 pageMarshall Community Letter: Person at Middle School Tests Positive For CoronavirusJoy M. HosfordNo ratings yet
- Nursing Care Plan Hyperthermia (Cap)Document2 pagesNursing Care Plan Hyperthermia (Cap)Algen UbasaNo ratings yet
- Risk Based Food Inspection SystemDocument52 pagesRisk Based Food Inspection Systemthanveer789No ratings yet
- The Exercise PrescriptionDocument68 pagesThe Exercise PrescriptionDario MoralesNo ratings yet
- REVISION Unit 4 - Unit 6: A Sore Throat A Headache A Stomach AcheDocument4 pagesREVISION Unit 4 - Unit 6: A Sore Throat A Headache A Stomach AcheNguyễn Hằng NgaNo ratings yet
- Kapalbhati PDFDocument2 pagesKapalbhati PDFRahul MishraNo ratings yet
- Anaplastic Thyroid CancerDocument40 pagesAnaplastic Thyroid Cancershita febrianaNo ratings yet
- Therapeutic Roles of Medicinal Herbs For The Treatment of Jaundice and Hepatitis BDocument7 pagesTherapeutic Roles of Medicinal Herbs For The Treatment of Jaundice and Hepatitis BEditor IJTSRDNo ratings yet
- Geriatric Nursing: Theories of AgingDocument4 pagesGeriatric Nursing: Theories of AgingNikkaDablioNo ratings yet
- Klayman Lawsuit Against ChinaDocument24 pagesKlayman Lawsuit Against ChinaLaw&Crime100% (5)
- QUESTIONNAIRE in Business ProfilingDocument4 pagesQUESTIONNAIRE in Business ProfilingLilibeth AgdamagNo ratings yet
- VNSG 1409 - Exam 3Document24 pagesVNSG 1409 - Exam 3luna nguyenNo ratings yet
- The Final FRCA Short Answer Questions - A Practical Study Guide (PDFDrive)Document348 pagesThe Final FRCA Short Answer Questions - A Practical Study Guide (PDFDrive)Andreea0% (1)
- APPENDICITISDocument6 pagesAPPENDICITISJAN ACCEL PAGADUANNo ratings yet
- Related Teenshealth Links: Health Problems SeriesDocument13 pagesRelated Teenshealth Links: Health Problems SeriesMario BadayosNo ratings yet
- Patient Classification & AssignmentDocument37 pagesPatient Classification & AssignmentAkhila UsNo ratings yet
- Supernumerary Teeth: Review of The Literature and A Survey of 152 CasesDocument11 pagesSupernumerary Teeth: Review of The Literature and A Survey of 152 CasesfatimahNo ratings yet
- African Americans Struggle With Disproportionate COVID Death TollDocument3 pagesAfrican Americans Struggle With Disproportionate COVID Death TollRodney BrooksNo ratings yet
- Oxford Handbook of Geriatric Medicine 3nbsped 0198738382 9780198738381 CompressDocument753 pagesOxford Handbook of Geriatric Medicine 3nbsped 0198738382 9780198738381 CompressNemer Isaeed100% (3)
- HLTH9 - 3Q First Aid For Common Unintentional InjuriesDocument5 pagesHLTH9 - 3Q First Aid For Common Unintentional InjuriesNardriel Kinsley TrongcosoNo ratings yet