Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5824)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Project Report On Cyber SecurityDocument60 pagesProject Report On Cyber SecurityHaritha63% (16)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Technical Manual (Part A) Tatuus-Msv 023: Release 1.03 (27/02/2023)Document80 pagesTechnical Manual (Part A) Tatuus-Msv 023: Release 1.03 (27/02/2023)Nelson Piquet Souto Maior100% (1)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Lincoln-Sl1 Centro-Matic Injector PDFDocument5 pagesLincoln-Sl1 Centro-Matic Injector PDFTaufan Nanjaya100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- CH 04Document110 pagesCH 04Angela Kuswandi100% (1)
- The Cadbury Code of Best Practices Had 19 RecommendationsDocument2 pagesThe Cadbury Code of Best Practices Had 19 RecommendationsAnam Shoaib82% (11)
- Abebe BasazinewDocument91 pagesAbebe BasazinewdagneNo ratings yet
- Media Preparation and Uses in Medical MicrobiologyDocument20 pagesMedia Preparation and Uses in Medical MicrobiologyPrincewill SeiyefaNo ratings yet
- Pe 4Document5 pagesPe 4slide_poshNo ratings yet
- Builder - PDF (China Substitution)Document11 pagesBuilder - PDF (China Substitution)Finsen SooNo ratings yet
- Software Defined Radio (SDR)Document11 pagesSoftware Defined Radio (SDR)Sanjay GiriNo ratings yet
- PQR Amp WPQ Standard Testing Parameter WorksheetDocument4 pagesPQR Amp WPQ Standard Testing Parameter WorksheetvinodNo ratings yet
- Geothermal Reservoir Simulation in Hot Sedimentary Aquifer System Using FeflowDocument1 pageGeothermal Reservoir Simulation in Hot Sedimentary Aquifer System Using FeflowImmanuel Lumban GaolNo ratings yet
- Simbol A4Document3 pagesSimbol A4ibnu100% (1)
- Zumba DLPDocument8 pagesZumba DLPJohnne Erika LarosaNo ratings yet
- Reading Comprehension 2 (Teamwork & Competition)Document16 pagesReading Comprehension 2 (Teamwork & Competition)Ibtisam alanaziNo ratings yet
- Confirmation For Booking ID # 843643049Document1 pageConfirmation For Booking ID # 843643049cindy brigitaNo ratings yet
- Fermentation of Cucumbers Brined With Calcium Chloride Instead of Sodium ChlorideDocument6 pagesFermentation of Cucumbers Brined With Calcium Chloride Instead of Sodium ChloridedupitosariNo ratings yet
- Capd 000000144Document83 pagesCapd 000000144Capitol Breach DiscoveryNo ratings yet
- Wallenberg's BlizzBaller - Diablo 2 at Diablo2Document9 pagesWallenberg's BlizzBaller - Diablo 2 at Diablo2kuntokinteNo ratings yet
- 89C51 Instruction SetDocument49 pages89C51 Instruction SetYashaswini B Srinivas100% (1)
- Disk No. Label Comments BootDocument1 pageDisk No. Label Comments BootDavid HiddingsNo ratings yet
- CIV2037F Additional QuestionsDocument3 pagesCIV2037F Additional QuestionsquikgoldNo ratings yet
- August 12, 2016 Strathmore TimesDocument20 pagesAugust 12, 2016 Strathmore TimesStrathmore TimesNo ratings yet
- At EgmrDocument1 pageAt EgmrQasim ButtNo ratings yet
- All Pass Comb FiltersDocument13 pagesAll Pass Comb Filterspho144No ratings yet
- Nutanix: NCP-MCI-5.15 ExamDocument7 pagesNutanix: NCP-MCI-5.15 ExamAlvin BosqueNo ratings yet
- IIFL Multicap PMS TermsheetDocument4 pagesIIFL Multicap PMS TermsheetRanjithNo ratings yet
- 1 - Proposal For 'Vision'Document3 pages1 - Proposal For 'Vision'hiram lodgeNo ratings yet
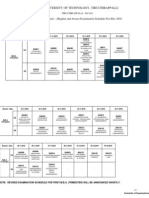
- Anna University of Technology, TiruchirappalliDocument2 pagesAnna University of Technology, TiruchirappallisanjeevrksNo ratings yet
- COT-Router Configuration - Docx - Republic of The Philippines DEPARTMENT OF EDUCATION Division of Sultan Kudarat BAI SARIPINANG - College SidekickDocument10 pagesCOT-Router Configuration - Docx - Republic of The Philippines DEPARTMENT OF EDUCATION Division of Sultan Kudarat BAI SARIPINANG - College Sidekickmarivic itongNo ratings yet