Download as xls, pdf, or txt
You might also like
- International Bill of Exchange TemplateDocument1 pageInternational Bill of Exchange Templatejj86% (95)
- Document PDFDocument1 pageDocument PDFAyo Boyi100% (1)
- Ethics Code - American ApparelDocument12 pagesEthics Code - American ApparelJeffTrexlerNo ratings yet
- Answers of Cash and Cash Equivalents AssignmentDocument4 pagesAnswers of Cash and Cash Equivalents AssignmentGee Lysa Pascua Vilbar50% (2)
- Full Merger Model Kraft-Kellogg - ShellDocument9 pagesFull Merger Model Kraft-Kellogg - ShellGeorgi VankovNo ratings yet
- MPR Attachment IRR 02 Lot 03Document9 pagesMPR Attachment IRR 02 Lot 03Sahinur RahamanNo ratings yet
- Form 26AS: Annual Tax Statement Under Section 203AA of The Income Tax Act, 1961Document4 pagesForm 26AS: Annual Tax Statement Under Section 203AA of The Income Tax Act, 1961NN Sarfaesi Solutions AgencyNo ratings yet
- Adt & Aadt Calculation As Per Irc:Sp:72-2007Document1 pageAdt & Aadt Calculation As Per Irc:Sp:72-2007ANKESH SHRIVASTAVANo ratings yet
- SBI Challan FormDocument1 pageSBI Challan FormPandu ChinnuNo ratings yet
- KWASalary Maker V.4.03Document79 pagesKWASalary Maker V.4.03Prudhvi ChargeNo ratings yet
- Monthly Suspense Report Dec 2023Document55 pagesMonthly Suspense Report Dec 2023Abata BageyuNo ratings yet
- GA Tax GuideDocument46 pagesGA Tax Guidedamilano1No ratings yet
- Journal, Ledger & Trial BalanceDocument5 pagesJournal, Ledger & Trial Balanceshikhamit20No ratings yet
- Check List 4Document2 pagesCheck List 4rababNo ratings yet
- Cqips5715a 2023Document4 pagesCqips5715a 2023Sneha SharmaNo ratings yet
- PRATAP DOME HoldingDocument1 pagePRATAP DOME HoldingRaj MishraNo ratings yet
- Portfolio Trades Market RateDocument35 pagesPortfolio Trades Market RateVenu MadhavNo ratings yet
- I 22 P100 1 2013Document1 pageI 22 P100 1 2013Casian GosaNo ratings yet
- 15 Dinora 115557 PDFDocument91 pages15 Dinora 115557 PDFMadhur GuptaNo ratings yet
- Uttaranchal Gramin BankDocument1 pageUttaranchal Gramin BankcsashikumarNo ratings yet
- Kajal Ghosh Holding TaxDocument1 pageKajal Ghosh Holding TaxRaj MishraNo ratings yet
- ChallanSBI GRBDocument1 pageChallanSBI GRBHimanshu BarthwalNo ratings yet
- Out StandingDocument1 pageOut Standingpyramid lavanNo ratings yet
- CashVoucher CLDocument1 pageCashVoucher CL123786123No ratings yet
- Anex ADocument4 pagesAnex AArshad BashirNo ratings yet
- Accrue WW May23Document9 pagesAccrue WW May23gudangasta321 asta321No ratings yet
- Description Previous This Period CumulativeDocument3 pagesDescription Previous This Period CumulativeChathuranga PriyasamanNo ratings yet
- A.Y. 2021-22Document4 pagesA.Y. 2021-22LAXMI FINANCENo ratings yet
- Gujrat Institute of Management Sciences Gujrat Institute of Management Sciences Gujrat Institute of Management SciencesDocument1 pageGujrat Institute of Management Sciences Gujrat Institute of Management Sciences Gujrat Institute of Management SciencesMuhammad Abdul SattarNo ratings yet
- Brajesh Kumar TA - 05 - 08 - 22Document3 pagesBrajesh Kumar TA - 05 - 08 - 22Sandeep BoraNo ratings yet
- Prepared By: Approved By: Reviewed By: Certified Correct By: Noted byDocument16 pagesPrepared By: Approved By: Reviewed By: Certified Correct By: Noted byAnonymous g0kSveSlLNo ratings yet
- Income - Tax - Return - 22-23 Enamul - FinalDocument17 pagesIncome - Tax - Return - 22-23 Enamul - Finalenamul whab100% (1)
- Punjab National Bank-01Document2 pagesPunjab National Bank-01Rahul .......No ratings yet
- Computation SlipDocument3 pagesComputation SlipDonnabelle MaquimotNo ratings yet
- Atlpr9507m 2021Document4 pagesAtlpr9507m 2021chandra DiveshNo ratings yet
- Total Amount of Checks Previously Issued Add:Checks Issued This PeriodDocument11 pagesTotal Amount of Checks Previously Issued Add:Checks Issued This PeriodDARYL DAVE FLORESNo ratings yet
- Onett Computation SheetDocument1 pageOnett Computation SheetBreahziel ParillaNo ratings yet
- Income - Tax - Return - NIAJ - 2018 - 2019 - 2020FINAL FORMDocument23 pagesIncome - Tax - Return - NIAJ - 2018 - 2019 - 2020FINAL FORMmostafiz18jun2007No ratings yet
- Daily Packing Report 2018-19Document23 pagesDaily Packing Report 2018-19pthimanshuNo ratings yet
- Statement of Account For Lpun0Hl0000052122: Demographic DetailsDocument3 pagesStatement of Account For Lpun0Hl0000052122: Demographic DetailsPradeep PandeyNo ratings yet
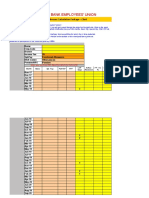
- Karur Vysya Bank Employees' Union: 11th Bipartite Arrears Calculation Package - ClerkDocument10 pagesKarur Vysya Bank Employees' Union: 11th Bipartite Arrears Calculation Package - ClerkDeepa ManianNo ratings yet
- PWD Budget 2019 - bp18Document76 pagesPWD Budget 2019 - bp18amitNo ratings yet
- Karan Kumar AprilDocument1 pageKaran Kumar AprilKirtan KumarNo ratings yet
- CBFM Form 06a by Contract ImplementationDocument4 pagesCBFM Form 06a by Contract ImplementationRoy RoqueNo ratings yet
- Petty Expenses Vendor Expenses: Synergy Property Development Page 1 of 6Document6 pagesPetty Expenses Vendor Expenses: Synergy Property Development Page 1 of 6daljeet singhNo ratings yet
- CLERKmodDocument2 pagesCLERKmodnishantyagi619No ratings yet
- Forms Sef Budget 1Document9 pagesForms Sef Budget 1Bryan Jeff AntonioNo ratings yet
- NurdiwiyantoDocument1 pageNurdiwiyantonur boyNo ratings yet
- ComputationDocument4 pagesComputationshriniwas83No ratings yet
- Test FileDocument1 pageTest FilealjamhisalemNo ratings yet
- Semester Registration Fees (Regular) Semester Registration Fees (Regular) Semester Registration Fees (Regular) Semester Registration Fees (Regular)Document2 pagesSemester Registration Fees (Regular) Semester Registration Fees (Regular) Semester Registration Fees (Regular) Semester Registration Fees (Regular)hemanta beheraNo ratings yet
- Bindu EXPENSES SHEETDocument1 pageBindu EXPENSES SHEETKrishna ReddyNo ratings yet
- TA Bill From 040320 To 070320Document2 pagesTA Bill From 040320 To 070320Ankit KhuranaNo ratings yet
- Property Details: Self Valuation ReportDocument1 pageProperty Details: Self Valuation ReportYogesh GautamNo ratings yet
- ChallanDocument1 pageChallankasiseerapuNo ratings yet
- Mhban14374600000012832 2020Document1 pageMhban14374600000012832 2020swapnildanavale17No ratings yet
- Transactions by Account: Tipco Estates CorporationDocument3 pagesTransactions by Account: Tipco Estates CorporationJa'maine ManguerraNo ratings yet
- Trip TicketDocument4 pagesTrip TicketMDRRMO ALAMADANo ratings yet
- Haryana Gramin Bank-01Document2 pagesHaryana Gramin Bank-01Rajkumar SoniNo ratings yet
- Local Counterpart In-Kind Contribution Journal CDD-87Document1 pageLocal Counterpart In-Kind Contribution Journal CDD-87EJ OsorioNo ratings yet
- District Wise Target Change RSODocument5 pagesDistrict Wise Target Change RSODevesh KumarNo ratings yet
- ePDS Ration Distribution RegisterDocument17 pagesePDS Ration Distribution RegisterAmit RanaNo ratings yet
- Framanlis Farms Vs MOLE: Substitute PaymentDocument9 pagesFramanlis Farms Vs MOLE: Substitute PaymentEzra Joy Angagan CanosaNo ratings yet
- Deed of SaleDocument2 pagesDeed of SaleJerickulit Ni Khimoy100% (1)
- Policy MacalisangDocument3 pagesPolicy MacalisangCrush RockNo ratings yet
- Instructions For MEEI TAX FORM 1Document3 pagesInstructions For MEEI TAX FORM 1Raghu AlankarNo ratings yet
- Grave Oral Defamation CasesDocument25 pagesGrave Oral Defamation Casesaj salazarNo ratings yet
- Consti CasesDocument43 pagesConsti CasesVIA ROMINA SOFIA VILLA VELASCONo ratings yet
- Invoice FANDocument1 pageInvoice FANVarsha A Kankanala0% (1)
- History of The Conflicts of LawDocument8 pagesHistory of The Conflicts of LawEdz Votefornoymar Del RosarioNo ratings yet
- Extended ECM - Solution Accelerator OverviewDocument30 pagesExtended ECM - Solution Accelerator OverviewIgnacio LucanoNo ratings yet
- TOEFL Teste PDFDocument2 pagesTOEFL Teste PDFLeonardo CorreiaNo ratings yet
- United States Court of Appeals, Tenth CircuitDocument9 pagesUnited States Court of Appeals, Tenth CircuitScribd Government DocsNo ratings yet
- 65 Sand V Abad Santos Educational InstitutionDocument2 pages65 Sand V Abad Santos Educational InstitutionCJ MillenaNo ratings yet
- Pros and Cons of Delegated LegislationDocument1 pagePros and Cons of Delegated LegislationNikhilesh MallickNo ratings yet
- Full Download Culture Counts A Concise Introduction To Cultural Anthropology 2nd Edition Nanda Test BankDocument11 pagesFull Download Culture Counts A Concise Introduction To Cultural Anthropology 2nd Edition Nanda Test Bankmasonpierce2z8s100% (41)
- Biblical Roots of DialogueDocument2 pagesBiblical Roots of DialogueBua NyohNo ratings yet
- Factsheet-Entrepreneur Transformation Ka GurukulDocument4 pagesFactsheet-Entrepreneur Transformation Ka GurukulJay Kumar BhattNo ratings yet
- Final-Draft ProposalDocument7 pagesFinal-Draft ProposalJaypee Semeni ApitNo ratings yet
- Admissions Policy 22-23 rvD8jMtDocument9 pagesAdmissions Policy 22-23 rvD8jMtRusu ElenaNo ratings yet
- 25 People V Balmores DigestDocument2 pages25 People V Balmores Digestjacaringal1No ratings yet
- H100Manual PDFDocument33 pagesH100Manual PDFKang Ray MonthNo ratings yet
- The Women S Suffrage MovementDocument22 pagesThe Women S Suffrage MovementRehanNo ratings yet
- 2 Term Mock Exam: Paper 1 Name: - Total Mark: - /30Document8 pages2 Term Mock Exam: Paper 1 Name: - Total Mark: - /30Training & Development GWCNo ratings yet
- Midterm Utp Malaysian StudiesDocument8 pagesMidterm Utp Malaysian StudiesNurul AishahNo ratings yet
- The Responsive Community JournalDocument144 pagesThe Responsive Community JournalMarceloNo ratings yet
- Cheque Bounce CaseDocument2 pagesCheque Bounce CasepreethiNo ratings yet
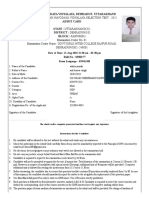
- Class Vi Jawahar Navodaya Vidyalaya Selection Test - 2021Document2 pagesClass Vi Jawahar Navodaya Vidyalaya Selection Test - 2021AkanshaNo ratings yet