Download as pdf or txt
You might also like
- Comprehensive - Pharmacy Review For NAPLEX Practice Exams Cases and Test Prep.8thDocument63 pagesComprehensive - Pharmacy Review For NAPLEX Practice Exams Cases and Test Prep.8thRabie YahfoufiNo ratings yet
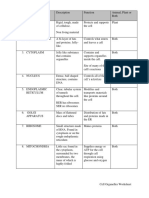
- Cell Organelles WorksheetDocument8 pagesCell Organelles WorksheetJohn OsborneNo ratings yet
- Pharmacokinetics: Biological MembraneDocument18 pagesPharmacokinetics: Biological MembraneRahul PalsNo ratings yet
- Pharmaco KineticsDocument42 pagesPharmaco KineticsNaghman ZuberiNo ratings yet
- PharmacokineticsDocument34 pagesPharmacokineticsAbdelrahman GalalNo ratings yet
- ADMEDocument15 pagesADMEsachin kumarNo ratings yet
- pharmacokineticsDocument20 pagespharmacokineticsAlfiya SaadiaNo ratings yet
- Seminar On Factor Affecting Drug Absorption: Presented byDocument42 pagesSeminar On Factor Affecting Drug Absorption: Presented byKrunal SamejaNo ratings yet
- Pharma Unit 3 2022 MidtermDocument57 pagesPharma Unit 3 2022 MidtermJohn Dave V. VillarmenteNo ratings yet
- Pharmaco 2Document83 pagesPharmaco 2marydenu101No ratings yet
- Drug AbsorptionDocument36 pagesDrug AbsorptionLawal AbidatNo ratings yet
- Main Principles of Clinical Pharmacology and Rational PharmacotherapyDocument58 pagesMain Principles of Clinical Pharmacology and Rational PharmacotherapyLucas Victor AlmeidaNo ratings yet
- Pharma Unit 3 2022Document51 pagesPharma Unit 3 2022John Dave V. VillarmenteNo ratings yet
- بيDocument48 pagesبيMojied AmeerNo ratings yet
- S.P.U - 404 - P'coloy-I - 4TH Sem - PK PDFDocument81 pagesS.P.U - 404 - P'coloy-I - 4TH Sem - PK PDFSiddh PatelNo ratings yet
- Absorption of DrugsDocument41 pagesAbsorption of DrugsSibtain100% (2)
- Basic Principles General PharmacologyDocument47 pagesBasic Principles General Pharmacologysapiah raman100% (2)
- PHARMACOKINETICS & PharmacokineticsDocument60 pagesPHARMACOKINETICS & PharmacokineticsRaj PathakNo ratings yet
- PHRM 0 KinetcxDocument37 pagesPHRM 0 KinetcxbumchikkNo ratings yet
- Pharmaco KineticsDocument69 pagesPharmaco KineticsSristeeNo ratings yet
- Pharmacokinetics - 1Document41 pagesPharmacokinetics - 1SristeeNo ratings yet
- PharmacokineticsDocument112 pagesPharmacokineticsGog Rg100% (2)
- Dosage Form Design CH 5 Lec 7Document68 pagesDosage Form Design CH 5 Lec 7noorlateffNo ratings yet
- Pharmacokinetics 2022Document63 pagesPharmacokinetics 2022amiruthejanaNo ratings yet
- PHARMACOKINETICSDocument55 pagesPHARMACOKINETICSnezifzenu2023No ratings yet
- Pharmacokinetics: DR Narendra KumarDocument60 pagesPharmacokinetics: DR Narendra Kumarperala vinaykumarNo ratings yet
- L6 AbsorptionDocument27 pagesL6 AbsorptionPatrick JnrNo ratings yet
- General PharmacologyDocument76 pagesGeneral PharmacologyMiyuru HasarangaNo ratings yet
- Factors Affecting Drug Absorption and BioavailabilityDocument4 pagesFactors Affecting Drug Absorption and BioavailabilityPGDME 20192020100% (1)
- Lecture 4 - Factors Affecting Drug ActionDocument31 pagesLecture 4 - Factors Affecting Drug ActionA. FatimaNo ratings yet
- Drug Absorption-DistributionDocument60 pagesDrug Absorption-DistributionRuqayya AdamuNo ratings yet
- Pharmacokinetics: Drug Absorption, Distribution, Metabolism and EliminationDocument25 pagesPharmacokinetics: Drug Absorption, Distribution, Metabolism and EliminationYoshiNo ratings yet
- Pharmacology - Pharmacology en PDFDocument386 pagesPharmacology - Pharmacology en PDFMaksym DemianchukNo ratings yet
- Lecture 2 - Basic Concepts of PharmacokineticsDocument63 pagesLecture 2 - Basic Concepts of Pharmacokineticsahmadslayman1No ratings yet
- What Is Drug Absorption?: Yolanda Smith, B.PharmDocument5 pagesWhat Is Drug Absorption?: Yolanda Smith, B.PharmNoorNo ratings yet
- 01 Concept of Medication TherapyDocument145 pages01 Concept of Medication TherapytoepaNo ratings yet
- Pharmacokinetics Part 1Document18 pagesPharmacokinetics Part 1Mahfuja khatun UrmeNo ratings yet
- Into Small Particles and Combine With A Liquid To Form A Solution, A Process Known As DISSOLUTION (DrugsDocument6 pagesInto Small Particles and Combine With A Liquid To Form A Solution, A Process Known As DISSOLUTION (DrugsMaemae MonNo ratings yet
- AbsorptionDocument61 pagesAbsorptionGreenNo ratings yet
- Metabolic Pathway & Renal ExcretionDocument29 pagesMetabolic Pathway & Renal ExcretionRadha krishnaNo ratings yet
- Absorpsi ObatDocument30 pagesAbsorpsi ObatdanielNo ratings yet
- Pharmacology Transes - Unit 1Document13 pagesPharmacology Transes - Unit 1venturaphoenixNo ratings yet
- Tugas Biofarmasetika 1 MetabolismeDocument21 pagesTugas Biofarmasetika 1 MetabolismePutri Zharifah MeutiaNo ratings yet
- Absorption of Drugs PDFDocument32 pagesAbsorption of Drugs PDFFirgo Arsalan100% (1)
- Lecture PharmacokineticsDocument55 pagesLecture Pharmacokineticssatya narayan100% (2)
- 3.unit - Pharmacokinetics 2Document40 pages3.unit - Pharmacokinetics 22020253350No ratings yet
- 1.pharmacology OpeningDocument6 pages1.pharmacology OpeningHOPENo ratings yet
- Drug Absorption 01Document15 pagesDrug Absorption 01Jannaatul Ferdous MimNo ratings yet
- Pharmacology 1st Chapter PPT New TOSDocument73 pagesPharmacology 1st Chapter PPT New TOSsajid aliNo ratings yet
- Tugas Biofarmasetika 1 Metabolisme: Nama: Yuliano Medora No BP: 1201169 Kelas: Reguler Stifarm Padang 2013Document21 pagesTugas Biofarmasetika 1 Metabolisme: Nama: Yuliano Medora No BP: 1201169 Kelas: Reguler Stifarm Padang 2013Putri Zharifah MeutiaNo ratings yet
- ADME Pertemuan 2Document54 pagesADME Pertemuan 2Andi ArdiansyahNo ratings yet
- Class Drug AbsorptionDocument35 pagesClass Drug Absorptionesha yadavNo ratings yet
- PharmacokineticsDocument25 pagesPharmacokineticsRajkishor YadavNo ratings yet
- Lecture 3Document37 pagesLecture 3Shafqat UllahNo ratings yet
- Pharmacokinetics: "What The Body Does To The Drug"Document41 pagesPharmacokinetics: "What The Body Does To The Drug"Virgo Eri SendiNo ratings yet
- Drug Action: Pharmaceutic, Pharmacokinetic, and Pharmacodynamic PhasesDocument10 pagesDrug Action: Pharmaceutic, Pharmacokinetic, and Pharmacodynamic PhasesVIGO, JERECELNo ratings yet
- Pharmaco KineticsDocument10 pagesPharmaco KineticsVithyaah ParameswaranNo ratings yet
- Membrane Permeability Versus Lipid (Olive Oil) :water Partition Coefficient ÀDocument11 pagesMembrane Permeability Versus Lipid (Olive Oil) :water Partition Coefficient ÀWindiarti RahayuNo ratings yet
- Pharmacokinetic & PharmacodynamicDocument77 pagesPharmacokinetic & Pharmacodynamicdimasscrib100% (1)
- General PharmacologyDocument101 pagesGeneral PharmacologyAditya RathoreNo ratings yet
- Handbook of Drug Interaction and the Mechanism of InteractionFrom EverandHandbook of Drug Interaction and the Mechanism of InteractionRating: 1 out of 5 stars1/5 (1)
- Cor 007 Module 17Document12 pagesCor 007 Module 17Camille ManlongatNo ratings yet
- Bio-FIT Book EN PDFDocument256 pagesBio-FIT Book EN PDFCesar Augusto Colorado RamirezNo ratings yet
- 5.nutrition Study and Quality Assurance Analysis by HPLCaaDocument65 pages5.nutrition Study and Quality Assurance Analysis by HPLCaayen88tvNo ratings yet
- Biofertilizer Part 2Document20 pagesBiofertilizer Part 2Garima BartariyaNo ratings yet
- General Biology - Chapter IDocument10 pagesGeneral Biology - Chapter IG.k. Vinnan Rao100% (2)
- Questionbank EST IMPDocument12 pagesQuestionbank EST IMPSaquibh Shaikh0% (1)
- Teal Sheets Addendum 02 - 2008Document2 pagesTeal Sheets Addendum 02 - 2008joséNo ratings yet
- Experiment 12 (Synthesis of Acetylsalicylic Acid)Document8 pagesExperiment 12 (Synthesis of Acetylsalicylic Acid)Cheng Bauzon100% (1)
- Understanding Nutrition 13th Edition Whitney Test Bank DownloadDocument18 pagesUnderstanding Nutrition 13th Edition Whitney Test Bank DownloadMichael Lozano100% (19)
- Southwick2017 Chapter LeadershipAndResilienceDocument19 pagesSouthwick2017 Chapter LeadershipAndResilienceUrsula MancusoNo ratings yet
- BSC Hons Zoology 2016-17 - 23 - 7 - 18Document45 pagesBSC Hons Zoology 2016-17 - 23 - 7 - 18DHUVADU JAGANATHAMNo ratings yet
- The Semantics of Morphological RelationsDocument65 pagesThe Semantics of Morphological RelationsDương Bùi100% (1)
- Kidney Structure and FunctionDocument68 pagesKidney Structure and FunctionAsmara Syed100% (1)
- DISLIPIDEMIA112Document20 pagesDISLIPIDEMIA112Apotek TribrataNo ratings yet
- Enzyme Application in The Textile IndustryDocument14 pagesEnzyme Application in The Textile IndustryFie100% (1)
- When A Women Picks Up An Apple and Bits ItDocument1 pageWhen A Women Picks Up An Apple and Bits ItDanial2296No ratings yet
- Blank2021 Article MarkerAllergensInHymenopteraVeDocument13 pagesBlank2021 Article MarkerAllergensInHymenopteraVeAna-Maria DuMiNo ratings yet
- Full Time Member, State Planning Commission, Government of Tamil NaduDocument5 pagesFull Time Member, State Planning Commission, Government of Tamil NadughurukumarNo ratings yet
- Rafaiqa-17Mar2023-Health Che PDFDocument8 pagesRafaiqa-17Mar2023-Health Che PDFmr copy xeroxNo ratings yet
- Shilajit A Panacea For CancerDocument9 pagesShilajit A Panacea For CancerRakeshKumarNo ratings yet
- Handwriting Saying - OralDocument1 pageHandwriting Saying - OralEsther FernandezNo ratings yet
- نباتاتDocument2 pagesنباتاتhaneen refaeeNo ratings yet
- Anti Bacterial and Biofilm Inhibitory Activities of Aegle Marmelos Methanol Leaf ExtractDocument9 pagesAnti Bacterial and Biofilm Inhibitory Activities of Aegle Marmelos Methanol Leaf ExtractIJAR JOURNALNo ratings yet
- Science L4 P2: Questions 1-11 Are Based On The Following PassageDocument108 pagesScience L4 P2: Questions 1-11 Are Based On The Following PassageMinhNo ratings yet
- IIB Sant Pau 2020 WebDocument336 pagesIIB Sant Pau 2020 WebAinhoa GaNo ratings yet
- VPH 83.43 Rev.1Document60 pagesVPH 83.43 Rev.1jubatus.libroNo ratings yet
- Evaluation of The Performance of Sysmex XN-3100 Automated Hematology Analyzer Regarding The Sysmex XE-2100 and Microscopic ExaminationDocument9 pagesEvaluation of The Performance of Sysmex XN-3100 Automated Hematology Analyzer Regarding The Sysmex XE-2100 and Microscopic ExaminationbalkisNo ratings yet
- Human Health & DiseaseDocument25 pagesHuman Health & DiseaseShiva PrabhakarNo ratings yet
- X Rays Benefit RiskDocument16 pagesX Rays Benefit RiskGianne KuizonNo ratings yet