Download as pdf or txt
You might also like
- Adhesive Capsulitis Presentation May 2009Document29 pagesAdhesive Capsulitis Presentation May 2009cm4100% (1)
- Clinical Neurological Examination and Localization Vinit Suri Z PDFDocument150 pagesClinical Neurological Examination and Localization Vinit Suri Z PDFEmergencias Rebagliati100% (1)
- Neurodynamic Testing and Neural MobilizationDocument44 pagesNeurodynamic Testing and Neural MobilizationSravs 9999No ratings yet
- Do Sliders' Slide and Tensioners' Tension An Analysis of Neurodynamic Techniques and Considerations Regarding Their Application PDFDocument9 pagesDo Sliders' Slide and Tensioners' Tension An Analysis of Neurodynamic Techniques and Considerations Regarding Their Application PDFryanbroad82No ratings yet
- Position Syndesmotic ScrewDocument4 pagesPosition Syndesmotic ScrewRoger WatersNo ratings yet
- Mccre Esh 2013Document1 pageMccre Esh 2013Francisco Javier Luza RamosNo ratings yet
- Balducci2006 PDFDocument8 pagesBalducci2006 PDFDimasBanyakRejekiNo ratings yet
- 2003 Changes in Median Nerve Somatosensory Transmission and Motor OutputDocument12 pages2003 Changes in Median Nerve Somatosensory Transmission and Motor OutputchooNo ratings yet
- Fatigue On Body BalanceDocument12 pagesFatigue On Body BalanceGeorge VasileiadisNo ratings yet
- Effects of Ankle Dorsiflexion On Range and Reliability of Straight Leg RaisingDocument10 pagesEffects of Ankle Dorsiflexion On Range and Reliability of Straight Leg RaisingMevi AniNo ratings yet
- Naskah Publikasi Dwi 12Document13 pagesNaskah Publikasi Dwi 12Isnawaty ZakariahNo ratings yet
- Normal Response To Upper Limb.......Document6 pagesNormal Response To Upper Limb.......PEDRONo ratings yet
- Conduction Block in Acute Motor AxonalDocument12 pagesConduction Block in Acute Motor Axonalgstam69No ratings yet
- 196 1025 1 PBDocument3 pages196 1025 1 PBJunaidy TahirNo ratings yet
- Artículo 1Document7 pagesArtículo 1angie caicedoNo ratings yet
- Descarga Repetitiva 4Document4 pagesDescarga Repetitiva 4fulgencio garciaNo ratings yet
- Lumbar Spinal Instability An Updated Rewiew 2167 7964.1000178Document5 pagesLumbar Spinal Instability An Updated Rewiew 2167 7964.1000178Yulita MustikasariNo ratings yet
- Diurnal T2 Changes of The Intervertebral Discs of The Entire Spine and The Influence of WeightliftingDocument6 pagesDiurnal T2 Changes of The Intervertebral Discs of The Entire Spine and The Influence of WeightliftingAlonso FernandezNo ratings yet
- Jpts 27 3355Document3 pagesJpts 27 3355Gabriel GonzalezNo ratings yet
- Cattaneo 2019Document11 pagesCattaneo 2019Rolando Huaman BravoNo ratings yet
- Comparison of Mulligan Technique Versus Muscle Energy Technique in Patients (Ingles)Document5 pagesComparison of Mulligan Technique Versus Muscle Energy Technique in Patients (Ingles)mauricio castroNo ratings yet
- Cranio-Cervical Exor Muscle Impairment at Maximal, Moderate, and Low Loads Is A Feature of Neck PainDocument6 pagesCranio-Cervical Exor Muscle Impairment at Maximal, Moderate, and Low Loads Is A Feature of Neck PainCristian Alejandro Flores PinuerNo ratings yet
- VISC Low Back Pain and Kidney Mobility Local Osteopathic Fascial Manipulation Decreases Pain Perception and Improves Renal MobilityDocument11 pagesVISC Low Back Pain and Kidney Mobility Local Osteopathic Fascial Manipulation Decreases Pain Perception and Improves Renal MobilityTito AlhoNo ratings yet
- Effect of Low-Level Light Therapy On Diabetic Foot Ulcers A Near-Infrared Spectroscopy StudyDocument8 pagesEffect of Low-Level Light Therapy On Diabetic Foot Ulcers A Near-Infrared Spectroscopy Studydaniele riminiNo ratings yet
- TendinitisDocument6 pagesTendinitisRivani KurniawanNo ratings yet
- HTTPS:WWW Ncbi NLM Nih gov:pmc:articles:PMC9144471:pdf:jpm-12-00808Document12 pagesHTTPS:WWW Ncbi NLM Nih gov:pmc:articles:PMC9144471:pdf:jpm-12-00808Ihsanul Ma'arifNo ratings yet
- SpondyloarthrosisDocument8 pagesSpondyloarthrosiselok ellyaNo ratings yet
- Effect of Thoracic Spinal Manipulation On Lower Limb Neurodynamics in Healthy Young Adults: Neural Link To Regional InterdependenceDocument10 pagesEffect of Thoracic Spinal Manipulation On Lower Limb Neurodynamics in Healthy Young Adults: Neural Link To Regional InterdependencekotzaNo ratings yet
- 2014 Calcium Channel Proteins Mediate Trigeminal Neuropathic Pain States Associated With Aberrant Excitatory SynaptogenesisDocument13 pages2014 Calcium Channel Proteins Mediate Trigeminal Neuropathic Pain States Associated With Aberrant Excitatory SynaptogenesisCristian OyarzoNo ratings yet
- 2003 Rapid Reversible Changes To Multiple Levels of The Human Somatosensory SystemDocument7 pages2003 Rapid Reversible Changes To Multiple Levels of The Human Somatosensory SystemchooNo ratings yet
- Final PPRDocument24 pagesFinal PPRAman hussainNo ratings yet
- To Compare The Effects of Maitland MobilizationDocument4 pagesTo Compare The Effects of Maitland MobilizationravichandragoudaNo ratings yet
- Effects of Tendon An Nerve Gliding Exercises and Instructions in Activities of Daily Livin Following Endoscopic Carpal Tunnel ReleaseDocument7 pagesEffects of Tendon An Nerve Gliding Exercises and Instructions in Activities of Daily Livin Following Endoscopic Carpal Tunnel ReleaseYimena JoyNo ratings yet
- 1 2011 Reduced Postoperative Wound Pain After Lumbar Spinous Process-Splitting LaminectDocument8 pages1 2011 Reduced Postoperative Wound Pain After Lumbar Spinous Process-Splitting Laminect18906628697No ratings yet
- Original Paper: Lumbar Disk Herniations - Clinical Status, Diagnosis, Imaging, Surgical Treatment and Global OutcomeDocument6 pagesOriginal Paper: Lumbar Disk Herniations - Clinical Status, Diagnosis, Imaging, Surgical Treatment and Global Outcomeasep budiyantoNo ratings yet
- Degala S.Document8 pagesDegala S.odontologia uvNo ratings yet
- Moore 2013Document9 pagesMoore 2013Andrés MardonesNo ratings yet
- Pulsed Shortwave Diathermy and Joint Mobilizations Restore A Twice Fractured Elbow With Metal Implants To Full Range of MotionDocument7 pagesPulsed Shortwave Diathermy and Joint Mobilizations Restore A Twice Fractured Elbow With Metal Implants To Full Range of MotionIndah YulantariNo ratings yet
- Penatalaksanaan Fisioterapi Kondisi Frozen ShoulderDocument11 pagesPenatalaksanaan Fisioterapi Kondisi Frozen ShoulderSasti aliciaNo ratings yet
- The Effectiveness of The Combination of Neuromuscular Taping (NMT) and Codman Pendulum Exercise To Improve The Functional Ability of The Shoulder in Patients With Frozen ShouldersDocument3 pagesThe Effectiveness of The Combination of Neuromuscular Taping (NMT) and Codman Pendulum Exercise To Improve The Functional Ability of The Shoulder in Patients With Frozen ShouldersInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Short Versus Long Outcome RadiologisDocument7 pagesShort Versus Long Outcome Radiologisandy ardiansyahNo ratings yet
- Hypothalamus and Amygdala Response To Acupuncture StimuliDocument13 pagesHypothalamus and Amygdala Response To Acupuncture StimuliAnibal CisternasNo ratings yet
- Abat 2016Document8 pagesAbat 2016toaldoNo ratings yet
- Paper Positional Release Technique SF MWDocument17 pagesPaper Positional Release Technique SF MWkamNo ratings yet
- Awh 291Document15 pagesAwh 291Emad Moody KaremNo ratings yet
- Original Article Vestibular Function After Spinal Cord Injury: Preliminary ResultsDocument4 pagesOriginal Article Vestibular Function After Spinal Cord Injury: Preliminary ResultsManik MishraNo ratings yet
- Banwell 2003Document5 pagesBanwell 2003JAVIERA NAVARRETE VIONo ratings yet
- Entrapment of The Posterior Interosseous Nerve - Ax ArticleDocument9 pagesEntrapment of The Posterior Interosseous Nerve - Ax ArticleNaz HossNo ratings yet
- Jurnal 1Document9 pagesJurnal 1fauziahsalsabilNo ratings yet
- 1 3劈开和开放随机对比Reduced postoperative wound pain after lumbar spinous process-splitting laminectDocument8 pages1 3劈开和开放随机对比Reduced postoperative wound pain after lumbar spinous process-splitting laminect18906628697No ratings yet
- 2014 The Anatomy of The Hip Abductors MusclesDocument13 pages2014 The Anatomy of The Hip Abductors Musclesmari netaNo ratings yet
- Ultrasound Therapy CTADocument5 pagesUltrasound Therapy CTAmitchNo ratings yet
- The Effects of Taping Neuromuscular Compare To Physical Therapies Modalities in Patients With Adhesive Capsulitis of The ShoulderDocument8 pagesThe Effects of Taping Neuromuscular Compare To Physical Therapies Modalities in Patients With Adhesive Capsulitis of The ShouldersilviaNo ratings yet
- Cat 2Document5 pagesCat 2Edgardo BivimasNo ratings yet
- Physiotherapy Management of SciaticaDocument6 pagesPhysiotherapy Management of SciaticaMuly Arafah ZakariaNo ratings yet
- Examination of Shoulder Positioning After Stroke: A Randomised Controlled Pilot TrialDocument6 pagesExamination of Shoulder Positioning After Stroke: A Randomised Controlled Pilot TrialAnggelia jopa sariNo ratings yet
- The Use of Kinesio Tape For Carpal Tunnel Syndrome: Mindy (Ming-Yao) Lou and Pou-Yu LeeDocument4 pagesThe Use of Kinesio Tape For Carpal Tunnel Syndrome: Mindy (Ming-Yao) Lou and Pou-Yu LeeAna Lu LoboNo ratings yet
- Altered Sensorimotor Integration in Parkinson's DiseaseDocument11 pagesAltered Sensorimotor Integration in Parkinson's Diseaseadit020586No ratings yet
- Background:: TH ST THDocument6 pagesBackground:: TH ST THRahayu WindariNo ratings yet
- Review: New Horizons in Diabetic Neuropathy: Mechanisms, Bioenergetics, and PainDocument18 pagesReview: New Horizons in Diabetic Neuropathy: Mechanisms, Bioenergetics, and PainDIBA TRIULANDARI KUSNADINo ratings yet
- Systemic Lupus Erythematosus: A Systematic Approach to Arthritis of Rheumatic Diseases: Volume 4From EverandSystemic Lupus Erythematosus: A Systematic Approach to Arthritis of Rheumatic Diseases: Volume 4No ratings yet
- MRI of Degenerative Disease of the Spine: A Case-Based AtlasFrom EverandMRI of Degenerative Disease of the Spine: A Case-Based AtlasNo ratings yet
- Specifications For Building A Verticalforce Platform Designed Forclinical StabilometryDocument3 pagesSpecifications For Building A Verticalforce Platform Designed Forclinical StabilometryMonica ViverosNo ratings yet
- Simoneau 1994Document11 pagesSimoneau 1994Monica ViverosNo ratings yet
- Does Somatosensory Loss Induce Adaptation of The Gait Initiation Process?Document4 pagesDoes Somatosensory Loss Induce Adaptation of The Gait Initiation Process?Monica ViverosNo ratings yet
- Gait & Posture: Fabio Scoppa, Roberto Capra, Michele Gallamini, Riccardo ShifferDocument3 pagesGait & Posture: Fabio Scoppa, Roberto Capra, Michele Gallamini, Riccardo ShifferMonica ViverosNo ratings yet
- Vitamin B12, Demyelination, Remyelination and Repair in Multiple SclerosisDocument5 pagesVitamin B12, Demyelination, Remyelination and Repair in Multiple SclerosisMonica ViverosNo ratings yet
- Salsa Bili 487Document12 pagesSalsa Bili 487Monica ViverosNo ratings yet
- Gait & Posture: Ana Flavia Gomes Paiva, Philippe Thoumie, Besma MissaouiDocument4 pagesGait & Posture: Ana Flavia Gomes Paiva, Philippe Thoumie, Besma MissaouiMonica ViverosNo ratings yet
- Fitzpatrick 1994Document14 pagesFitzpatrick 1994Monica ViverosNo ratings yet
- The Rochester Diabetic Neuropathy StudyDocument10 pagesThe Rochester Diabetic Neuropathy StudyMonica ViverosNo ratings yet
- Organization of Postural Responses Following A Rotational Support Surface Perturbation, After TKA: Sagittal Plane RotationsDocument9 pagesOrganization of Postural Responses Following A Rotational Support Surface Perturbation, After TKA: Sagittal Plane RotationsMonica ViverosNo ratings yet
- Grade 4 Fractions To Decimals ADocument2 pagesGrade 4 Fractions To Decimals AMonica ViverosNo ratings yet
- Convert Between Fractions and Decimals NumbersDocument2 pagesConvert Between Fractions and Decimals NumbersMonica ViverosNo ratings yet
- Percentage of Number Worksheet: Calculate The PercentagesDocument2 pagesPercentage of Number Worksheet: Calculate The PercentagesMonica ViverosNo ratings yet
- Fraction To DecimalDocument2 pagesFraction To DecimalMonica ViverosNo ratings yet
- Write The Correct Comparison Symbol (, or ) in Each BoxDocument2 pagesWrite The Correct Comparison Symbol (, or ) in Each BoxMonica ViverosNo ratings yet
- Decimal ComparisonDocument2 pagesDecimal ComparisonMonica ViverosNo ratings yet
- Free Download Neuroimaging Part Ii Joseph C Masdeu and R Gilberto Gonzalez Eds Full Chapter PDFDocument51 pagesFree Download Neuroimaging Part Ii Joseph C Masdeu and R Gilberto Gonzalez Eds Full Chapter PDFsteve.nunes421100% (20)
- Encore A New Hard Hat Could Help Protect Workers From On The Job Brain Injuries.Document3 pagesEncore A New Hard Hat Could Help Protect Workers From On The Job Brain Injuries.Xander XanderNo ratings yet
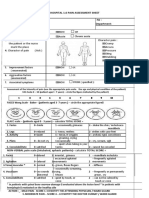
- Fisa Evaluare DurereDocument2 pagesFisa Evaluare DurerecristianNo ratings yet
- Solution Manual For Psychology Canadian 5Th Edition Wade Tavris Garry Saucier Elias 0205960359 9780205960354 Full Chapter PDFDocument36 pagesSolution Manual For Psychology Canadian 5Th Edition Wade Tavris Garry Saucier Elias 0205960359 9780205960354 Full Chapter PDFjoseph.meachen325100% (14)
- Full Download Ebook Ebook PDF Netters Atlas of Neuroscience 3rd Edition PDFDocument35 pagesFull Download Ebook Ebook PDF Netters Atlas of Neuroscience 3rd Edition PDFdavid.anderson198100% (46)
- The Effect of Spinal Exercises On H-Reflex in Subjects With Lumbosacral RadiculopathyDocument5 pagesThe Effect of Spinal Exercises On H-Reflex in Subjects With Lumbosacral RadiculopathyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- MS FileDocument8 pagesMS FileFARAH MOHAMMEDNo ratings yet
- Ex - Cerebellar ExamDocument2 pagesEx - Cerebellar ExamssNo ratings yet
- Organisation of The Motor Cortex Differs OaDocument11 pagesOrganisation of The Motor Cortex Differs OaThiago LoureiroNo ratings yet
- Answers To 3.10: The Nervous SystemDocument1 pageAnswers To 3.10: The Nervous SystembrownieallennNo ratings yet
- 4.2 Higher Brain Function 74Document74 pages4.2 Higher Brain Function 74Namomsa W.No ratings yet
- Physical Education in The Tertiary LevelDocument35 pagesPhysical Education in The Tertiary Levelhatsune mikuNo ratings yet
- MSDSDocument9 pagesMSDSrofano aswanNo ratings yet
- Ncmb317 Lecture: Psychiatric Mental Health Nursing: Bachelor of Science in Nursing 3YBDocument5 pagesNcmb317 Lecture: Psychiatric Mental Health Nursing: Bachelor of Science in Nursing 3YB2 - GUEVARRA, KYLE JOSHUA M.No ratings yet
- The Neurologic ExamDocument7 pagesThe Neurologic ExamGabriel ArizaNo ratings yet
- Controlling Your Dopamine For Motivation, FocusDocument111 pagesControlling Your Dopamine For Motivation, Focuswnd cNo ratings yet
- J Urnal El-Riyasah, Volume 11 Nomor 1 Tahun 2020 Sosiady & ErmansyahDocument15 pagesJ Urnal El-Riyasah, Volume 11 Nomor 1 Tahun 2020 Sosiady & Ermansyaheko purwantoNo ratings yet
- Cerebrospinal Fluid and Blood Brain BarrierDocument29 pagesCerebrospinal Fluid and Blood Brain BarrierSaiAlekhaBabuNo ratings yet
- 8790 37908 1 PBDocument5 pages8790 37908 1 PBjenna cupidoNo ratings yet
- Nervous System Part 1Document6 pagesNervous System Part 1rb YangzonNo ratings yet
- Auras Epilépticas: Clasificación, Fisiopatología, Utilidad Práctica, Diagnóstico Diferencial y ControversiasDocument7 pagesAuras Epilépticas: Clasificación, Fisiopatología, Utilidad Práctica, Diagnóstico Diferencial y ControversiasMartinAnteparraNo ratings yet
- Nervous System-2022-23 Asi̇stDocument101 pagesNervous System-2022-23 Asi̇stYiğit GündüzNo ratings yet
- Download textbook Bridging Research And Good Practices Towards Patients Welfare Proceedings Of The 4Th International Conference On Healthcare Ergonomics And Patient Safety Heps Taipei Taiwan 23 26 June 2014 1St Edition ebook all chapter pdfDocument54 pagesDownload textbook Bridging Research And Good Practices Towards Patients Welfare Proceedings Of The 4Th International Conference On Healthcare Ergonomics And Patient Safety Heps Taipei Taiwan 23 26 June 2014 1St Edition ebook all chapter pdfjudy.chappel556100% (18)
- PainDocument23 pagesPainJenjen Cortey100% (3)
- Midbrain, Pons, and Medulla: Anatomy and SyndromesDocument16 pagesMidbrain, Pons, and Medulla: Anatomy and SyndromesJasper CubiasNo ratings yet
- Science Lesson Nervecell-10Document4 pagesScience Lesson Nervecell-10Strawberry MilkeuNo ratings yet
- Case Studies in NeurologyDocument3 pagesCase Studies in NeurologyOnline WriterNo ratings yet
- Full Download Test Bank For Health Psychology 3rd Canadian Edition PDF Full ChapterDocument36 pagesFull Download Test Bank For Health Psychology 3rd Canadian Edition PDF Full Chapterrequinneologic8yzqgt100% (20)