Download as pdf or txt
You might also like
- TataAIA PAR Product Bonus History FY23Document4 pagesTataAIA PAR Product Bonus History FY23Arpit ShahNo ratings yet
- SHC Intra Abdominal GuidelinesDocument13 pagesSHC Intra Abdominal GuidelinesNguyễn Mạnh CườngNo ratings yet
- Antibiotic GuidelinesDocument54 pagesAntibiotic GuidelineskhattakpsychoNo ratings yet
- JETIR2211463Document8 pagesJETIR2211463AshuNo ratings yet
- Urinary NTMDocument4 pagesUrinary NTMsaraabolghasemi1No ratings yet
- VAP Guidelines 7.7.04aDocument5 pagesVAP Guidelines 7.7.04aCorina DavidNo ratings yet
- Drug Action Indications and Contraindications Nursing ResponsibilityDocument2 pagesDrug Action Indications and Contraindications Nursing ResponsibilityAcbel RnucoNo ratings yet
- Alert Antibiotic GuideliinesDocument6 pagesAlert Antibiotic GuideliinesEman MohamedNo ratings yet
- MrsaDocument13 pagesMrsaPaula Grace MorfeNo ratings yet
- VK Enteroc FacalisDocument20 pagesVK Enteroc FacalistinhyeuvoiyhocNo ratings yet
- Multi-Drug Resistant Organisms (Mdros) in Healthcare FacilitiesDocument57 pagesMulti-Drug Resistant Organisms (Mdros) in Healthcare Facilitiesasma .sassiNo ratings yet
- CellulitisDocument3 pagesCellulitisshedNo ratings yet
- 30 Glycopeptides Vancomycin and Teicoplanin 2015 Mandell Douglas and BDocument29 pages30 Glycopeptides Vancomycin and Teicoplanin 2015 Mandell Douglas and BHelen DyNo ratings yet
- Antibiotic Regimens For Neonatal Sepsis - UpToDateDocument2 pagesAntibiotic Regimens For Neonatal Sepsis - UpToDateMohd MaghyrehNo ratings yet
- J. - Antimicrob. - Chemother. 2013 Vandecasteele 743 8Document6 pagesJ. - Antimicrob. - Chemother. 2013 Vandecasteele 743 8Natalia MoranNo ratings yet
- Microbiological Effects of Prior Vancomycin Use in Patients With Methicillin-Resistant Staphylococcus Aureus BacteraemiaDocument6 pagesMicrobiological Effects of Prior Vancomycin Use in Patients With Methicillin-Resistant Staphylococcus Aureus Bacteraemiaapi-19597023No ratings yet
- Guideline Wound InfectionDocument5 pagesGuideline Wound Infectioncut fatiaNo ratings yet
- IMG EmpAposterDocument1 pageIMG EmpAposterChiu LeoNo ratings yet
- Alternatives To Vancomycin For The Treatment of Methicillin-Resistant Staphylococcus Aureus InfectionsDocument7 pagesAlternatives To Vancomycin For The Treatment of Methicillin-Resistant Staphylococcus Aureus InfectionsInna MaynizaNo ratings yet
- Antibiotics10 PDFDocument19 pagesAntibiotics10 PDFDharani TharanNo ratings yet
- Antibiotics10 PDFDocument19 pagesAntibiotics10 PDFDharani TharanNo ratings yet
- Role of Antibiotics in Orthopedic InfectionsDocument31 pagesRole of Antibiotics in Orthopedic InfectionsRakesh KumarNo ratings yet
- Cefazolina Más Que VancomicinaDocument7 pagesCefazolina Más Que VancomicinaRicardo UchuyaNo ratings yet
- 2021 Infection Management PosterDocument1 page2021 Infection Management PosterBosco WoodsNo ratings yet
- Antibiotic EssentialsDocument6 pagesAntibiotic EssentialsAna MariaNo ratings yet
- Newyork-Presbyterian Hospital Sites: Columbia University Medical Center Guideline: Medication Use Manual Page 1 of 12Document12 pagesNewyork-Presbyterian Hospital Sites: Columbia University Medical Center Guideline: Medication Use Manual Page 1 of 12Ebey SomanNo ratings yet
- Severe Sepsis and Septic Shock Antibiotic Guide: Community AcquiredDocument6 pagesSevere Sepsis and Septic Shock Antibiotic Guide: Community AcquiredAnonymous G6zDTD2yNo ratings yet
- Assessment of Antibiotic Utilization in Sepsis Order Sets Initiated in The Emergency Department Draft 2Document45 pagesAssessment of Antibiotic Utilization in Sepsis Order Sets Initiated in The Emergency Department Draft 2api-652562554No ratings yet
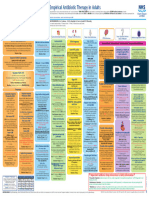
- Guidelines Emporical Antibiotic Therapy in AdultDocument2 pagesGuidelines Emporical Antibiotic Therapy in Adultgulf jobsNo ratings yet
- Guidelines For Treatment of Intra-Abdominal Infections in AdultsDocument10 pagesGuidelines For Treatment of Intra-Abdominal Infections in AdultsPratama InsaniNo ratings yet
- Daptomycin Susceptibility of Methicillin Resistant.21Document2 pagesDaptomycin Susceptibility of Methicillin Resistant.21duongnguyenNo ratings yet
- PENAFIEL M6 April21-2023Document21 pagesPENAFIEL M6 April21-2023Precious Valerie PenafielNo ratings yet
- Antimicrobial Therapy in The Intensive Care UnitDocument14 pagesAntimicrobial Therapy in The Intensive Care UnitNyimas Irina SilvaniNo ratings yet
- Wesleyan: College of Nursing and Allied Medical SciencesDocument2 pagesWesleyan: College of Nursing and Allied Medical SciencesShane Aileen AngelesNo ratings yet
- Basics of AntibioticsDocument42 pagesBasics of AntibioticsAsma BakheitNo ratings yet
- How I Treat M.NucciDocument11 pagesHow I Treat M.NucciRafael SuzukiNo ratings yet
- Skin Soft Tissue Infections 1 - 27 - 2019Document14 pagesSkin Soft Tissue Infections 1 - 27 - 2019Muhammad Azhar ImranNo ratings yet
- Empirical Antibiotic Therapy in Children v7 Exp 31 Dec 2020Document2 pagesEmpirical Antibiotic Therapy in Children v7 Exp 31 Dec 2020Mohamad MostafaNo ratings yet
- Atbs Cocos Pos MDRDocument24 pagesAtbs Cocos Pos MDRvascoNo ratings yet
- Antibiotics, Antifungal, Anti-Infective, Anti-Inflammatory, AntiviralDocument24 pagesAntibiotics, Antifungal, Anti-Infective, Anti-Inflammatory, AntiviralKim AmadoNo ratings yet
- Mscano, Journal Editor, Jidc-012-0978Document7 pagesMscano, Journal Editor, Jidc-012-0978imyours9601No ratings yet
- Rational Use of Antimicrobial AgentsDocument1 pageRational Use of Antimicrobial AgentsJay PatilNo ratings yet
- Drug StudyDocument5 pagesDrug Studyapi-3717941100% (6)
- Antibiotic Therapy For Peritonitis: Treatment Overview, Spontaneous Bacterial Peritonitis, Secondary and Tertiary PeritonitisDocument7 pagesAntibiotic Therapy For Peritonitis: Treatment Overview, Spontaneous Bacterial Peritonitis, Secondary and Tertiary PeritonitisTias SubagioNo ratings yet
- Antibiotic Choices For Treatment of MRSADocument16 pagesAntibiotic Choices For Treatment of MRSAfarmasi_hm100% (2)
- Antibiotic Guidelines For BONE AND JOINT INFECTIONSDocument3 pagesAntibiotic Guidelines For BONE AND JOINT INFECTIONSKhurram NadeemNo ratings yet
- MDROsDocument94 pagesMDROsRAHULNo ratings yet
- Pharma-URO-CYCLIC LIPOEPETIDES (Vancomycin)Document6 pagesPharma-URO-CYCLIC LIPOEPETIDES (Vancomycin)Hussein AlhaddadNo ratings yet
- Clin Infect Dis.-2010-Fishbain-79-84Document6 pagesClin Infect Dis.-2010-Fishbain-79-84Edson MarquesNo ratings yet
- Drug Study Ko BFF Pa-Print Pls Thanks Much Mwa!Document3 pagesDrug Study Ko BFF Pa-Print Pls Thanks Much Mwa!shasheeeeyNo ratings yet
- tmp9D6F TMPDocument3 pagestmp9D6F TMPFrontiersNo ratings yet
- 2.fahad Khaliq.... Febrile Neutro - pptx-1Document38 pages2.fahad Khaliq.... Febrile Neutro - pptx-1dr FAHADKHALIQSIALNo ratings yet
- 2.fahad Khaliq.... Febrile Neutro - pptx-1Document38 pages2.fahad Khaliq.... Febrile Neutro - pptx-1dr FAHADKHALIQSIALNo ratings yet
- Antibiotic Class Summary TableDocument6 pagesAntibiotic Class Summary TableuserherwwweNo ratings yet
- SHC Heme Onc Antimicrobial ProphylaxisDocument4 pagesSHC Heme Onc Antimicrobial ProphylaxisTala MahmoudNo ratings yet
- Pneumonia Drug StudyDocument3 pagesPneumonia Drug Studyatienza02No ratings yet
- DR Lie Khie Chen - Management of MDR Infection in Sepsis Jade 2016Document33 pagesDR Lie Khie Chen - Management of MDR Infection in Sepsis Jade 2016Astria PermanaNo ratings yet
- Ofelia L. Mendoza - Drug StudyDocument3 pagesOfelia L. Mendoza - Drug StudyMaenard JavierNo ratings yet
- Empiric Antibiotic ListDocument2 pagesEmpiric Antibiotic ListpasswordNo ratings yet
- Nosocomial Infections in The ICU: Learning ObjectivesDocument5 pagesNosocomial Infections in The ICU: Learning ObjectivesJumadil AkbarriansyahNo ratings yet
- Long Term LiabilitiesDocument21 pagesLong Term Liabilitiesnioriatti8924No ratings yet
- What Is Your TypeDocument2 pagesWhat Is Your TypeΛευτέρης ΚαπετανάκηςNo ratings yet
- Skripsi Alvi AkmaliaDocument94 pagesSkripsi Alvi Akmaliakhoiriah nasutionNo ratings yet
- LyricsDocument6 pagesLyricsViernes, John Henilon C. - BSED FilipinoNo ratings yet
- Cylinder Safety Poster (ID 801089) 042019 B2 500x700mmDocument1 pageCylinder Safety Poster (ID 801089) 042019 B2 500x700mmChris TeohNo ratings yet
- Requiem Bloodlines & PowersDocument16 pagesRequiem Bloodlines & PowersLuiz Henrique Matias MarcondesNo ratings yet
- Drexel SL 30-40-50 AC MM F-626-0419Document140 pagesDrexel SL 30-40-50 AC MM F-626-0419Abel GonzalezNo ratings yet
- Parole: Ca 2 - Non-Institutional CorrectionsDocument8 pagesParole: Ca 2 - Non-Institutional CorrectionsWena Mae Cristobal100% (5)
- CASE STUDY CAKE BATIK Proximate AnalysisDocument25 pagesCASE STUDY CAKE BATIK Proximate AnalysisNur Azhani100% (1)
- CVDocument2 pagesCVTaha Akhtar KhanNo ratings yet
- Emergency Preparedness For Severe WeatherDocument2 pagesEmergency Preparedness For Severe WeatherRandy PedrozaNo ratings yet
- Alternatives To Shifting Cultivation-248Document9 pagesAlternatives To Shifting Cultivation-248Chandrashekhar KhobragadeNo ratings yet
- Activity Completion Report: Department of EducationDocument5 pagesActivity Completion Report: Department of EducationTeacher Mitze100% (1)
- Aprelim - Purely CompensationDocument67 pagesAprelim - Purely CompensationAshley VasquezNo ratings yet
- SMACNA Technical Manuals and Standards - Book Price List: SMACNA of San DiegoDocument1 pageSMACNA Technical Manuals and Standards - Book Price List: SMACNA of San DiegoPeanut d. DestroyerNo ratings yet
- Playground and Water Safety GuidelinesDocument50 pagesPlayground and Water Safety GuidelinesNgoc Nhu NguyenNo ratings yet
- RPZ Testing Form 215bDocument2 pagesRPZ Testing Form 215bSam ChoiNo ratings yet
- Coring & Coring Analysis 2Document21 pagesCoring & Coring Analysis 2Reband Azad100% (1)
- SFDA Requirement For DEXADocument9 pagesSFDA Requirement For DEXAEhsan alwafaaNo ratings yet
- 57-Online Rejection Note, Material ReturnDocument3 pages57-Online Rejection Note, Material Returnananth100% (1)
- Case Ih Tractor 1070 Operators Manual 9 2822Document22 pagesCase Ih Tractor 1070 Operators Manual 9 2822zacharygonzalez130703jse100% (140)
- AA Allen - Deliver MeDocument86 pagesAA Allen - Deliver Mecaren ronoNo ratings yet
- Odd 3Document14 pagesOdd 3jeetguptaNo ratings yet
- Catalyst in Refining PetrochemicalsDocument5 pagesCatalyst in Refining PetrochemicalsgshdavidNo ratings yet
- Shida: - EvarDocument107 pagesShida: - Evarpravin mundeNo ratings yet
- EcoDocument7 pagesEcoSushma YonzenNo ratings yet
- Code On Wages 2019 - NotesDocument3 pagesCode On Wages 2019 - NotesAnand ReddyNo ratings yet
- DNA DR In-Class ActivitiesDocument15 pagesDNA DR In-Class ActivitiesCéline Engels100% (1)
- Product Risk Assessment Practices Regulatory AgenciesDocument19 pagesProduct Risk Assessment Practices Regulatory AgenciesAllyssa FernandezNo ratings yet