
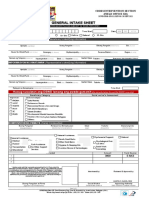
General Intake Sheet I Clientx27s Identifying Information PDF Free
General Intake Sheet I Clientx27s Identifying Information PDF Free
You might also like
- Adult Mswd-ToolDocument3 pagesAdult Mswd-Toolclaverialc10100% (1)
- Manual Op Final Cdo CSWDDocument66 pagesManual Op Final Cdo CSWDRc Tsini Solis100% (4)
- Parental Capability Assssment Report (For Child - )Document5 pagesParental Capability Assssment Report (For Child - )APRIL ANNE BALASON AGSOLID100% (4)
- Orca Share Media1662701335116 6973874860683163750Document1 pageOrca Share Media1662701335116 6973874860683163750Michelle G. BorretaNo ratings yet
- RISB TestDocument7 pagesRISB TestIrsa Zaheer100% (2)
- Assessment Tool For ElderlyDocument4 pagesAssessment Tool For ElderlySheinna DuranNo ratings yet
- TLE Hairdressing Grade 8 - 9Document25 pagesTLE Hairdressing Grade 8 - 9Roswlle50% (2)
- Level of Effectiveness of Family Development Session To The Parent Leader of Pantawid Pamilyang Pilipino Program at SagabDocument24 pagesLevel of Effectiveness of Family Development Session To The Parent Leader of Pantawid Pamilyang Pilipino Program at Sagabjunkassio100% (4)
- Forms Pension ResumptionDocument2 pagesForms Pension ResumptionMei Mei100% (1)
- Colegio de San Francisco Javier: Social CaseworkDocument3 pagesColegio de San Francisco Javier: Social CaseworkSORIA Shinehah EvaNo ratings yet
- Executive Order No. 21-2021 Local Council For The Protection of ChildrenDocument2 pagesExecutive Order No. 21-2021 Local Council For The Protection of ChildrenLyn Tabelisma Ozar100% (2)
- 5 Proposal. EF-PEAFDocument3 pages5 Proposal. EF-PEAFRamil100% (1)
- PWD Budget ProposalDocument2 pagesPWD Budget ProposalMa. Gelina E. Depone0% (2)
- Executive Order 011-11-4ps MacDocument2 pagesExecutive Order 011-11-4ps MacErnest Aton100% (1)
- Lcat Vawc FormDocument1 pageLcat Vawc FormKurt Javier0% (1)
- JJWA Form-1Document4 pagesJJWA Form-1Marieta Alejo50% (2)
- Training For Vaw Desk Officers and Barangay Officers On AntiDocument1 pageTraining For Vaw Desk Officers and Barangay Officers On AntigheljoshNo ratings yet
- Management Performance Appraisal Form: Employee InformationDocument4 pagesManagement Performance Appraisal Form: Employee Informationmahsa choop100% (1)
- Aics Forms For PackchiefsDocument4 pagesAics Forms For PackchiefsMaria Estrellita BolasaNo ratings yet
- Certificate of Participation: Is Given ToDocument1 pageCertificate of Participation: Is Given ToMA. CHONA APOLENo ratings yet
- General Intake Sheet: I. Clients Identifying InformationDocument2 pagesGeneral Intake Sheet: I. Clients Identifying InformationErnest Aton100% (4)
- Youth Leadership and Values Formation CampDocument1 pageYouth Leadership and Values Formation CampKuya KimNo ratings yet
- CBL KALIPI Amended As of June 2023Document14 pagesCBL KALIPI Amended As of June 2023Ana LeahNo ratings yet
- Action Plan Sitio LambacDocument7 pagesAction Plan Sitio LambacNeon True BeldiaNo ratings yet
- Janessa L. YaboDocument41 pagesJanessa L. Yaboterence cagandahanNo ratings yet
- Basic Orientation On ErpatDocument30 pagesBasic Orientation On ErpatManilyn B Cruz100% (1)
- Government Internship Program (Gip) & Immersion Outreach Program (Iop)Document3 pagesGovernment Internship Program (Gip) & Immersion Outreach Program (Iop)Fhaiyne Aresgado LptNo ratings yet
- EDUC. Form Loren FINALDocument2 pagesEDUC. Form Loren FINALJENNIFER FORTU100% (1)
- VAW Desk Assessment Tool For Best Barangay VAW DeskDocument15 pagesVAW Desk Assessment Tool For Best Barangay VAW DeskAndrea Lizares Si100% (2)
- CBRP Advocacy ActivitiesDocument2 pagesCBRP Advocacy ActivitiesRohaina SapalNo ratings yet
- Draft Design - Erpat TraainingDocument2 pagesDraft Design - Erpat TraainingMerry Merry100% (1)
- GRCMDocument102 pagesGRCMManilyn B Cruz100% (2)
- Municipality of Kapangan Office of The Municipal Social Welfare and DevelopmentDocument8 pagesMunicipality of Kapangan Office of The Municipal Social Welfare and DevelopmentNill Patrick Ulat DulceNo ratings yet
- Individual Performance Commitment & Review Form: Department of Education Schools Division ofDocument3 pagesIndividual Performance Commitment & Review Form: Department of Education Schools Division ofHansel VillasorNo ratings yet
- 2nd QTR Meeting PYAPDocument3 pages2nd QTR Meeting PYAPAROIN Salvador100% (1)
- Orientation Seminar On Gender and Development With Anti-VAWCDocument40 pagesOrientation Seminar On Gender and Development With Anti-VAWCEdna Mae Cruz100% (2)
- CICL Intake and ReferralDocument12 pagesCICL Intake and ReferralAndro EvangelistaNo ratings yet
- Social Case Study Report: Republic of The Philippines City of TarlacDocument4 pagesSocial Case Study Report: Republic of The Philippines City of TarlacJonathan100% (1)
- Session 4 - Camp Management TeamDocument28 pagesSession 4 - Camp Management TeamCHANIELOU MARTINEZ100% (1)
- Letter For Creation of PositionDocument1 pageLetter For Creation of PositionMark Ronald ArgoteNo ratings yet
- Municipal Social Welfare and Development Office Social Case StudyDocument2 pagesMunicipal Social Welfare and Development Office Social Case StudyHannah Naki MedinaNo ratings yet
- Certificate of Appearance DSWDDocument1 pageCertificate of Appearance DSWDAileen Labastida Barcenas100% (1)
- Persons With Disability Affairs Office Annual Accomplishment ReportDocument2 pagesPersons With Disability Affairs Office Annual Accomplishment ReportJoemar CafrancaNo ratings yet
- Name Relation To Client AGE Civil Status Educ'L Attainment Occupation Monthly IncomeDocument2 pagesName Relation To Client AGE Civil Status Educ'L Attainment Occupation Monthly IncomeKaren LaurinNo ratings yet
- Dafac FormDocument6 pagesDafac FormRobert Dela Cruz LamelaNo ratings yet
- Xycotec Girl Case StudyDocument10 pagesXycotec Girl Case StudyChristian PaulNo ratings yet
- Sustainability Assessment of The Kalipunan NG Liping Pilipina (KALIPI) Program Implementation in Iligan City and Cagayan de Oro CityDocument12 pagesSustainability Assessment of The Kalipunan NG Liping Pilipina (KALIPI) Program Implementation in Iligan City and Cagayan de Oro CityPsychology and Education: A Multidisciplinary JournalNo ratings yet
- Letter of SupplementalDocument4 pagesLetter of SupplementalSample BakeshopNo ratings yet
- CSC PDSDocument5 pagesCSC PDSPingotMagangaNo ratings yet
- (Mm-Dd-Yyyy) (Name of Barangay)Document2 pages(Mm-Dd-Yyyy) (Name of Barangay)RANDY BAOGBOG100% (1)
- 4Ps-MCCT ESSI Guidelines For ExeCom May 25Document26 pages4Ps-MCCT ESSI Guidelines For ExeCom May 25keziah100% (1)
- Social Case Study ReportDocument5 pagesSocial Case Study ReportAngelNo ratings yet
- CLJIP TampilisanDocument20 pagesCLJIP TampilisanJosephine Templa-JamolodNo ratings yet
- Child Study Report DSWDDocument2 pagesChild Study Report DSWDPablo Eschoval100% (3)
- Intake Sheet For Children in Conflict With The Law (Cicl) and Child at Risk (Car)Document2 pagesIntake Sheet For Children in Conflict With The Law (Cicl) and Child at Risk (Car)Ann Jelaine Noveno100% (3)
- Project Brief-CBRP MIOPDocument2 pagesProject Brief-CBRP MIOPJomidy Midtanggal50% (2)
- Republic Act 6972 (Day Care)Document3 pagesRepublic Act 6972 (Day Care)Erly Mae100% (1)
- Request For TanodDocument2 pagesRequest For TanodNerwin IbarrientosNo ratings yet
- Competency Assessment For Community Empowerment FacilitatorsDocument8 pagesCompetency Assessment For Community Empowerment FacilitatorsRhisia RaborNo ratings yet
- Certificate of EligibilityDocument2 pagesCertificate of EligibilityReina montes100% (1)
- NSRP Form 1Document2 pagesNSRP Form 1Ghie San Jose100% (1)
- The Interactionist Approach: Client Individual or Group System Group, Agency, or OtherDocument27 pagesThe Interactionist Approach: Client Individual or Group System Group, Agency, or OtherRonie Bongolo Dacuba0% (1)
- PMRF RevisedDocument4 pagesPMRF RevisedacsalcedaNo ratings yet
- Concept MapDocument4 pagesConcept MapCasison Mark ArrysonNo ratings yet
- Medial Plantar Flap For Hand ReconstructionDocument7 pagesMedial Plantar Flap For Hand ReconstructionMiguel JohnsonNo ratings yet
- DermatosesDocument12 pagesDermatosesnjoom100% (1)
- An Analysis of How Street Food in India Can Be Made Safe FoodDocument9 pagesAn Analysis of How Street Food in India Can Be Made Safe FoodAnsari faizan ahmedNo ratings yet
- Unit Plan Healthy Relationships 3Document60 pagesUnit Plan Healthy Relationships 3api-269745950No ratings yet
- Vitafoods Europe 2023 Post Show ReportDocument16 pagesVitafoods Europe 2023 Post Show ReportJoan PonsNo ratings yet
- Family Nursing Care Plan ModuleDocument16 pagesFamily Nursing Care Plan ModuleHarlene Joyce ReyNo ratings yet
- Science Investigatory ProjectDocument84 pagesScience Investigatory ProjectRain AmeNo ratings yet
- Neonatal NotesDocument34 pagesNeonatal Notesgridchan100% (2)
- OSCE Cerebellar Examination PDFDocument6 pagesOSCE Cerebellar Examination PDFriczen vilaNo ratings yet
- Document 15 Unseen PassageDocument3 pagesDocument 15 Unseen PassageAntara DuttaNo ratings yet
- Argumentative Essay Report - Mental HealthDocument7 pagesArgumentative Essay Report - Mental HealthJonel James NaritoNo ratings yet
- PE Day 2Document3 pagesPE Day 2Joi Joi JoiNo ratings yet
- UMI Research Proposal One Chapter I-IIIDocument48 pagesUMI Research Proposal One Chapter I-IIIKomakech Simon DemeterNo ratings yet
- Multivitamins in The Prevention of Cardiovasculan Disease in MenDocument10 pagesMultivitamins in The Prevention of Cardiovasculan Disease in MennutrinathyalvesNo ratings yet
- To Save: File - Download As - Microsoft Excel (.XLSX) - Drworkout - FitnessDocument16 pagesTo Save: File - Download As - Microsoft Excel (.XLSX) - Drworkout - FitnessGustavoAguirreValencianaNo ratings yet
- PhilCare-FAQ Coverage PDFDocument1 pagePhilCare-FAQ Coverage PDFNoel EboniaNo ratings yet
- Lesson PlanDocument21 pagesLesson PlanRyrl ShinNo ratings yet
- Daftar Obat Lasa Dan High Alert Yang Diberi LabelDocument3 pagesDaftar Obat Lasa Dan High Alert Yang Diberi LabelNila Permata SariNo ratings yet
- Hospital Equipment. Research ReportDocument6 pagesHospital Equipment. Research ReportYazan Al JabariNo ratings yet
- Dissertation On Stress Management PDFDocument7 pagesDissertation On Stress Management PDFCustomWritingPapersUK100% (1)
- Creatina FosfoquinasaDocument1 pageCreatina Fosfoquinasasusey tepaNo ratings yet
- Bagalkot AhvsDocument5 pagesBagalkot AhvsChandu HosmaniNo ratings yet
- The Skilled Helper Model of HelpingDocument21 pagesThe Skilled Helper Model of HelpingMoana MarieeNo ratings yet
- Case Based 1 - Week 9Document3 pagesCase Based 1 - Week 9DharaNo ratings yet
- Biocheck C2P - PSK Pharma PDFDocument9 pagesBiocheck C2P - PSK Pharma PDFFari ShaikhNo ratings yet
- Mase Student Planner 6Document25 pagesMase Student Planner 6api-242315971No ratings yet






















































































Download as pdf or txt
You might also like
- Adult Mswd-ToolDocument3 pagesAdult Mswd-Toolclaverialc10100% (1)
- Manual Op Final Cdo CSWDDocument66 pagesManual Op Final Cdo CSWDRc Tsini Solis100% (4)
- Parental Capability Assssment Report (For Child - )Document5 pagesParental Capability Assssment Report (For Child - )APRIL ANNE BALASON AGSOLID100% (4)
- Orca Share Media1662701335116 6973874860683163750Document1 pageOrca Share Media1662701335116 6973874860683163750Michelle G. BorretaNo ratings yet
- RISB TestDocument7 pagesRISB TestIrsa Zaheer100% (2)
- Assessment Tool For ElderlyDocument4 pagesAssessment Tool For ElderlySheinna DuranNo ratings yet
- TLE Hairdressing Grade 8 - 9Document25 pagesTLE Hairdressing Grade 8 - 9Roswlle50% (2)
- Level of Effectiveness of Family Development Session To The Parent Leader of Pantawid Pamilyang Pilipino Program at SagabDocument24 pagesLevel of Effectiveness of Family Development Session To The Parent Leader of Pantawid Pamilyang Pilipino Program at Sagabjunkassio100% (4)
- Forms Pension ResumptionDocument2 pagesForms Pension ResumptionMei Mei100% (1)
- Colegio de San Francisco Javier: Social CaseworkDocument3 pagesColegio de San Francisco Javier: Social CaseworkSORIA Shinehah EvaNo ratings yet
- Executive Order No. 21-2021 Local Council For The Protection of ChildrenDocument2 pagesExecutive Order No. 21-2021 Local Council For The Protection of ChildrenLyn Tabelisma Ozar100% (2)
- 5 Proposal. EF-PEAFDocument3 pages5 Proposal. EF-PEAFRamil100% (1)
- PWD Budget ProposalDocument2 pagesPWD Budget ProposalMa. Gelina E. Depone0% (2)
- Executive Order 011-11-4ps MacDocument2 pagesExecutive Order 011-11-4ps MacErnest Aton100% (1)
- Lcat Vawc FormDocument1 pageLcat Vawc FormKurt Javier0% (1)
- JJWA Form-1Document4 pagesJJWA Form-1Marieta Alejo50% (2)
- Training For Vaw Desk Officers and Barangay Officers On AntiDocument1 pageTraining For Vaw Desk Officers and Barangay Officers On AntigheljoshNo ratings yet
- Management Performance Appraisal Form: Employee InformationDocument4 pagesManagement Performance Appraisal Form: Employee Informationmahsa choop100% (1)
- Aics Forms For PackchiefsDocument4 pagesAics Forms For PackchiefsMaria Estrellita BolasaNo ratings yet
- Certificate of Participation: Is Given ToDocument1 pageCertificate of Participation: Is Given ToMA. CHONA APOLENo ratings yet
- General Intake Sheet: I. Clients Identifying InformationDocument2 pagesGeneral Intake Sheet: I. Clients Identifying InformationErnest Aton100% (4)
- Youth Leadership and Values Formation CampDocument1 pageYouth Leadership and Values Formation CampKuya KimNo ratings yet
- CBL KALIPI Amended As of June 2023Document14 pagesCBL KALIPI Amended As of June 2023Ana LeahNo ratings yet
- Action Plan Sitio LambacDocument7 pagesAction Plan Sitio LambacNeon True BeldiaNo ratings yet
- Janessa L. YaboDocument41 pagesJanessa L. Yaboterence cagandahanNo ratings yet
- Basic Orientation On ErpatDocument30 pagesBasic Orientation On ErpatManilyn B Cruz100% (1)
- Government Internship Program (Gip) & Immersion Outreach Program (Iop)Document3 pagesGovernment Internship Program (Gip) & Immersion Outreach Program (Iop)Fhaiyne Aresgado LptNo ratings yet
- EDUC. Form Loren FINALDocument2 pagesEDUC. Form Loren FINALJENNIFER FORTU100% (1)
- VAW Desk Assessment Tool For Best Barangay VAW DeskDocument15 pagesVAW Desk Assessment Tool For Best Barangay VAW DeskAndrea Lizares Si100% (2)
- CBRP Advocacy ActivitiesDocument2 pagesCBRP Advocacy ActivitiesRohaina SapalNo ratings yet
- Draft Design - Erpat TraainingDocument2 pagesDraft Design - Erpat TraainingMerry Merry100% (1)
- GRCMDocument102 pagesGRCMManilyn B Cruz100% (2)
- Municipality of Kapangan Office of The Municipal Social Welfare and DevelopmentDocument8 pagesMunicipality of Kapangan Office of The Municipal Social Welfare and DevelopmentNill Patrick Ulat DulceNo ratings yet
- Individual Performance Commitment & Review Form: Department of Education Schools Division ofDocument3 pagesIndividual Performance Commitment & Review Form: Department of Education Schools Division ofHansel VillasorNo ratings yet
- 2nd QTR Meeting PYAPDocument3 pages2nd QTR Meeting PYAPAROIN Salvador100% (1)
- Orientation Seminar On Gender and Development With Anti-VAWCDocument40 pagesOrientation Seminar On Gender and Development With Anti-VAWCEdna Mae Cruz100% (2)
- CICL Intake and ReferralDocument12 pagesCICL Intake and ReferralAndro EvangelistaNo ratings yet
- Social Case Study Report: Republic of The Philippines City of TarlacDocument4 pagesSocial Case Study Report: Republic of The Philippines City of TarlacJonathan100% (1)
- Session 4 - Camp Management TeamDocument28 pagesSession 4 - Camp Management TeamCHANIELOU MARTINEZ100% (1)
- Letter For Creation of PositionDocument1 pageLetter For Creation of PositionMark Ronald ArgoteNo ratings yet
- Municipal Social Welfare and Development Office Social Case StudyDocument2 pagesMunicipal Social Welfare and Development Office Social Case StudyHannah Naki MedinaNo ratings yet
- Certificate of Appearance DSWDDocument1 pageCertificate of Appearance DSWDAileen Labastida Barcenas100% (1)
- Persons With Disability Affairs Office Annual Accomplishment ReportDocument2 pagesPersons With Disability Affairs Office Annual Accomplishment ReportJoemar CafrancaNo ratings yet
- Name Relation To Client AGE Civil Status Educ'L Attainment Occupation Monthly IncomeDocument2 pagesName Relation To Client AGE Civil Status Educ'L Attainment Occupation Monthly IncomeKaren LaurinNo ratings yet
- Dafac FormDocument6 pagesDafac FormRobert Dela Cruz LamelaNo ratings yet
- Xycotec Girl Case StudyDocument10 pagesXycotec Girl Case StudyChristian PaulNo ratings yet
- Sustainability Assessment of The Kalipunan NG Liping Pilipina (KALIPI) Program Implementation in Iligan City and Cagayan de Oro CityDocument12 pagesSustainability Assessment of The Kalipunan NG Liping Pilipina (KALIPI) Program Implementation in Iligan City and Cagayan de Oro CityPsychology and Education: A Multidisciplinary JournalNo ratings yet
- Letter of SupplementalDocument4 pagesLetter of SupplementalSample BakeshopNo ratings yet
- CSC PDSDocument5 pagesCSC PDSPingotMagangaNo ratings yet
- (Mm-Dd-Yyyy) (Name of Barangay)Document2 pages(Mm-Dd-Yyyy) (Name of Barangay)RANDY BAOGBOG100% (1)
- 4Ps-MCCT ESSI Guidelines For ExeCom May 25Document26 pages4Ps-MCCT ESSI Guidelines For ExeCom May 25keziah100% (1)
- Social Case Study ReportDocument5 pagesSocial Case Study ReportAngelNo ratings yet
- CLJIP TampilisanDocument20 pagesCLJIP TampilisanJosephine Templa-JamolodNo ratings yet
- Child Study Report DSWDDocument2 pagesChild Study Report DSWDPablo Eschoval100% (3)
- Intake Sheet For Children in Conflict With The Law (Cicl) and Child at Risk (Car)Document2 pagesIntake Sheet For Children in Conflict With The Law (Cicl) and Child at Risk (Car)Ann Jelaine Noveno100% (3)
- Project Brief-CBRP MIOPDocument2 pagesProject Brief-CBRP MIOPJomidy Midtanggal50% (2)
- Republic Act 6972 (Day Care)Document3 pagesRepublic Act 6972 (Day Care)Erly Mae100% (1)
- Request For TanodDocument2 pagesRequest For TanodNerwin IbarrientosNo ratings yet
- Competency Assessment For Community Empowerment FacilitatorsDocument8 pagesCompetency Assessment For Community Empowerment FacilitatorsRhisia RaborNo ratings yet
- Certificate of EligibilityDocument2 pagesCertificate of EligibilityReina montes100% (1)
- NSRP Form 1Document2 pagesNSRP Form 1Ghie San Jose100% (1)
- The Interactionist Approach: Client Individual or Group System Group, Agency, or OtherDocument27 pagesThe Interactionist Approach: Client Individual or Group System Group, Agency, or OtherRonie Bongolo Dacuba0% (1)
- PMRF RevisedDocument4 pagesPMRF RevisedacsalcedaNo ratings yet
- Concept MapDocument4 pagesConcept MapCasison Mark ArrysonNo ratings yet
- Medial Plantar Flap For Hand ReconstructionDocument7 pagesMedial Plantar Flap For Hand ReconstructionMiguel JohnsonNo ratings yet
- DermatosesDocument12 pagesDermatosesnjoom100% (1)
- An Analysis of How Street Food in India Can Be Made Safe FoodDocument9 pagesAn Analysis of How Street Food in India Can Be Made Safe FoodAnsari faizan ahmedNo ratings yet
- Unit Plan Healthy Relationships 3Document60 pagesUnit Plan Healthy Relationships 3api-269745950No ratings yet
- Vitafoods Europe 2023 Post Show ReportDocument16 pagesVitafoods Europe 2023 Post Show ReportJoan PonsNo ratings yet
- Family Nursing Care Plan ModuleDocument16 pagesFamily Nursing Care Plan ModuleHarlene Joyce ReyNo ratings yet
- Science Investigatory ProjectDocument84 pagesScience Investigatory ProjectRain AmeNo ratings yet
- Neonatal NotesDocument34 pagesNeonatal Notesgridchan100% (2)
- OSCE Cerebellar Examination PDFDocument6 pagesOSCE Cerebellar Examination PDFriczen vilaNo ratings yet
- Document 15 Unseen PassageDocument3 pagesDocument 15 Unseen PassageAntara DuttaNo ratings yet
- Argumentative Essay Report - Mental HealthDocument7 pagesArgumentative Essay Report - Mental HealthJonel James NaritoNo ratings yet
- PE Day 2Document3 pagesPE Day 2Joi Joi JoiNo ratings yet
- UMI Research Proposal One Chapter I-IIIDocument48 pagesUMI Research Proposal One Chapter I-IIIKomakech Simon DemeterNo ratings yet
- Multivitamins in The Prevention of Cardiovasculan Disease in MenDocument10 pagesMultivitamins in The Prevention of Cardiovasculan Disease in MennutrinathyalvesNo ratings yet
- To Save: File - Download As - Microsoft Excel (.XLSX) - Drworkout - FitnessDocument16 pagesTo Save: File - Download As - Microsoft Excel (.XLSX) - Drworkout - FitnessGustavoAguirreValencianaNo ratings yet
- PhilCare-FAQ Coverage PDFDocument1 pagePhilCare-FAQ Coverage PDFNoel EboniaNo ratings yet
- Lesson PlanDocument21 pagesLesson PlanRyrl ShinNo ratings yet
- Daftar Obat Lasa Dan High Alert Yang Diberi LabelDocument3 pagesDaftar Obat Lasa Dan High Alert Yang Diberi LabelNila Permata SariNo ratings yet
- Hospital Equipment. Research ReportDocument6 pagesHospital Equipment. Research ReportYazan Al JabariNo ratings yet
- Dissertation On Stress Management PDFDocument7 pagesDissertation On Stress Management PDFCustomWritingPapersUK100% (1)
- Creatina FosfoquinasaDocument1 pageCreatina Fosfoquinasasusey tepaNo ratings yet
- Bagalkot AhvsDocument5 pagesBagalkot AhvsChandu HosmaniNo ratings yet
- The Skilled Helper Model of HelpingDocument21 pagesThe Skilled Helper Model of HelpingMoana MarieeNo ratings yet
- Case Based 1 - Week 9Document3 pagesCase Based 1 - Week 9DharaNo ratings yet
- Biocheck C2P - PSK Pharma PDFDocument9 pagesBiocheck C2P - PSK Pharma PDFFari ShaikhNo ratings yet
- Mase Student Planner 6Document25 pagesMase Student Planner 6api-242315971No ratings yet