
Clinical Profile of Melkersson-Rosenthal Syndrome/Orofacial Granulomatosis: A Review of 51 Patients
Clinical Profile of Melkersson-Rosenthal Syndrome/Orofacial Granulomatosis: A Review of 51 Patients
You might also like
- Oral LPDocument5 pagesOral LPkahkashanahmed065No ratings yet
- MelanomaDocument6 pagesMelanomaagung permanaNo ratings yet
- Nasopalatine Duct Cyst Restro StudyDocument8 pagesNasopalatine Duct Cyst Restro StudyTiara Oktavia SaputriNo ratings yet
- Devasconceloscarvalho 2010Document4 pagesDevasconceloscarvalho 2010Fermín GómezNo ratings yet
- Granulomatous Cheilitis: A of 6 Cases and A Review of The LiteratureDocument7 pagesGranulomatous Cheilitis: A of 6 Cases and A Review of The LiteratureAlfiatuz ZahroNo ratings yet
- Dental Panoramic Radiographic Evaluation in Bisphosphonate-Associated Osteonecrosis of The JawsDocument1 pageDental Panoramic Radiographic Evaluation in Bisphosphonate-Associated Osteonecrosis of The Jawsmateusmoreira2004No ratings yet
- Artigo 1 ParacococcidiodomicoseDocument9 pagesArtigo 1 Paracococcidiodomicoseandre.jaccoud2No ratings yet
- Lack of Association Between Celiac Disease and Dental Enamel HypoplasiaDocument6 pagesLack of Association Between Celiac Disease and Dental Enamel HypoplasiaLjubomirErdoglijaNo ratings yet
- HN 04-2011 Sublingual Gland Tumors PDFDocument6 pagesHN 04-2011 Sublingual Gland Tumors PDFHafiz FatmarNo ratings yet
- Oral Findings of Systemic Lupus Erythematosus - A Grand Round CaseDocument6 pagesOral Findings of Systemic Lupus Erythematosus - A Grand Round CaseArditya Dwi YudistiraNo ratings yet
- Oral Findings of Systemic Lupus Erythematosus-A Grand Round CaseDocument5 pagesOral Findings of Systemic Lupus Erythematosus-A Grand Round CaseIntanNo ratings yet
- Absceso CerebralDocument6 pagesAbsceso Cerebralkreacher3000No ratings yet
- JCDP 21 651Document6 pagesJCDP 21 651Diego GambinNo ratings yet
- Clinical and Pathologic Analyses of Tuberculosis in The Oral Cavity: Report of 11 CasesDocument8 pagesClinical and Pathologic Analyses of Tuberculosis in The Oral Cavity: Report of 11 CasesMaria Lozano Figueroa 5to secNo ratings yet
- 3.tahrir N. Aldelaimi Article Occurrence of Lichen Planus in Diabetes MellitusDocument4 pages3.tahrir N. Aldelaimi Article Occurrence of Lichen Planus in Diabetes MellitusMohammed AbdulhammedNo ratings yet
- Almeida Dear Ruda 2021Document23 pagesAlmeida Dear Ruda 2021pamela queirozNo ratings yet
- Original Article Retrospective Analysis of Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis Over A Period of 10 YearsDocument6 pagesOriginal Article Retrospective Analysis of Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis Over A Period of 10 YearssyalalaaalalaaaNo ratings yet
- Introduction To The Oral and Maxillofacial Pathology Focus Issue On "Preneoplastic Oral Epithelial Lesions"Document11 pagesIntroduction To The Oral and Maxillofacial Pathology Focus Issue On "Preneoplastic Oral Epithelial Lesions"jesus ulises estrada cantuNo ratings yet
- Paranasal Sinuses Malignancies: A 12-Year Review of Clinical CharacteristicsDocument5 pagesParanasal Sinuses Malignancies: A 12-Year Review of Clinical CharacteristicsRidho RifhansyahNo ratings yet
- Melkersson-Rosenthal Syndrome Revisited As A Misdiagnosed DiseaseDocument10 pagesMelkersson-Rosenthal Syndrome Revisited As A Misdiagnosed DiseasePedro NascimentoNo ratings yet
- PAPER (ENG) - The Presentation and Management of Laryngeal Cleft - A 10 Years ExperienceDocument7 pagesPAPER (ENG) - The Presentation and Management of Laryngeal Cleft - A 10 Years ExperienceAldo Hip NaranjoNo ratings yet
- Profile of Tinea Corporis and Tinea Cruris in Dermatovenereology Clinic of Tertiery Hospital: A Retrospective StudyDocument6 pagesProfile of Tinea Corporis and Tinea Cruris in Dermatovenereology Clinic of Tertiery Hospital: A Retrospective StudyRose ParkNo ratings yet
- Alotaiby Et Al, 2015Document7 pagesAlotaiby Et Al, 2015DKNo ratings yet
- 2 Olp and HPEDocument7 pages2 Olp and HPEdrnusratnaziromarNo ratings yet
- Treacher Collins Syndrome: A Systematic Review of Evidence-Based Treatment and RecommendationsDocument14 pagesTreacher Collins Syndrome: A Systematic Review of Evidence-Based Treatment and RecommendationsSai KrupaNo ratings yet
- Mucosal Melanoma of The Head and Neck 32-Year ExperienceDocument5 pagesMucosal Melanoma of The Head and Neck 32-Year ExperienceWahyu JuliandaNo ratings yet
- Expression and Distribution of Galectin-1 and Np-63/ Immuno-Histochemical Markers in Potentially Malignant Oral Disorders With and Without DysplasiaDocument7 pagesExpression and Distribution of Galectin-1 and Np-63/ Immuno-Histochemical Markers in Potentially Malignant Oral Disorders With and Without DysplasiaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Efficacy of Steroidal Vs Non-Steroidal Agents in Oral Lichen Planus: A Randomised, Open-Label StudyDocument9 pagesEfficacy of Steroidal Vs Non-Steroidal Agents in Oral Lichen Planus: A Randomised, Open-Label StudyRetno ManggalihNo ratings yet
- Primary Subacute Hematogenous Osteomyelitis in Children: A Clearer Bacteriological EtiologyDocument6 pagesPrimary Subacute Hematogenous Osteomyelitis in Children: A Clearer Bacteriological EtiologymiNo ratings yet
- SclerosingDocument5 pagesSclerosingHakan KüçükerNo ratings yet
- A Clinical and Epidemiological Study On Discoid Lupus ErythematosusDocument7 pagesA Clinical and Epidemiological Study On Discoid Lupus Erythematosusiin sakinah dewiNo ratings yet
- Jurnal PatogenesisDocument6 pagesJurnal PatogenesisErmiati EmhyNo ratings yet
- Artigo 2 - Symptomatic Meckel's Diverticulum in Children - A 12-Year Survey - 2021Document4 pagesArtigo 2 - Symptomatic Meckel's Diverticulum in Children - A 12-Year Survey - 2021Larissa RuthyelyNo ratings yet
- Chromosome 1p36 DeletionsDocument4 pagesChromosome 1p36 Deletionsericwang12No ratings yet
- Referensi Dari Saya No 8Document7 pagesReferensi Dari Saya No 8Kalsum MbNo ratings yet
- Systematic Review of Oral Manifestations Related To HyperparathyroidismDocument27 pagesSystematic Review of Oral Manifestations Related To Hyperparathyroidismanang dwiNo ratings yet
- Research ArticleDocument10 pagesResearch ArticlePratama Imanuel RawungNo ratings yet
- Patogenesis Pleomorphic AdenomaDocument6 pagesPatogenesis Pleomorphic AdenomaYeni PuspitasariNo ratings yet
- Bjorl: Clinical Diagnosis and Histological Analysis of Vocal Nodules and PolypsDocument7 pagesBjorl: Clinical Diagnosis and Histological Analysis of Vocal Nodules and PolypsRia Tupamahu MatatulaNo ratings yet
- 2022 Janas NazeDocument10 pages2022 Janas NazeazizhamoudNo ratings yet
- Enl 7Document4 pagesEnl 7Prizilia SaimimaNo ratings yet
- Maedica 18 645Document6 pagesMaedica 18 645s7ybkjhb44No ratings yet
- Hemangioma InmunohistoquimicaDocument20 pagesHemangioma InmunohistoquimicaSalome ChaconNo ratings yet
- Saini 2016 Calci NoseDocument5 pagesSaini 2016 Calci NoseRym MesfarNo ratings yet
- Ijced 3 (3) 101-109Document9 pagesIjced 3 (3) 101-109GembongSatriaMahardhikaNo ratings yet
- Profile of Tinea Corporis and Tinea Cruris in Dermatovenereology Clinic of Tertiery Hospital: A Retrospective StudyDocument6 pagesProfile of Tinea Corporis and Tinea Cruris in Dermatovenereology Clinic of Tertiery Hospital: A Retrospective StudyMarwiyahNo ratings yet
- Complications of Acute Rhinosinusitis in The Netherlands: F S Hansen, R Hoffmans, C Georgalas and W J FokkensDocument7 pagesComplications of Acute Rhinosinusitis in The Netherlands: F S Hansen, R Hoffmans, C Georgalas and W J Fokkenspanji satryo utomoNo ratings yet
- 664 8537 1 PBDocument5 pages664 8537 1 PBMICHAEL NUGROHONo ratings yet
- Chromosomal Instability, DNA Index, Dysplasia, and SubsiteDocument10 pagesChromosomal Instability, DNA Index, Dysplasia, and SubsiteManar AliNo ratings yet
- Hiperplasia Proceso CoronoidesDocument7 pagesHiperplasia Proceso CoronoidesJuan Carlos MeloNo ratings yet
- Osteosarcoma of The Jaw An Analysis of A Series of 74 Cases (2013)Document8 pagesOsteosarcoma of The Jaw An Analysis of A Series of 74 Cases (2013)sTEVENNo ratings yet
- Sebaceous Carcinoma of The Eyelids: Personal Experience With 60 CasesDocument7 pagesSebaceous Carcinoma of The Eyelids: Personal Experience With 60 CasesJocho NeavesNo ratings yet
- Prevalence and Clinical Features of Pigmented Oral LesionsDocument9 pagesPrevalence and Clinical Features of Pigmented Oral LesionsAlma AlejandraNo ratings yet
- Sjögren's Syndrome: From Pathogenesis To Novel Therapeutic TargetsDocument5 pagesSjögren's Syndrome: From Pathogenesis To Novel Therapeutic TargetsOcha24 TupamahuNo ratings yet
- Costa JOE2013Document5 pagesCosta JOE2013KristineNo ratings yet
- 13 Pediatric Follicular MucinosisDocument7 pages13 Pediatric Follicular MucinosisGi D'AtriNo ratings yet
- Evaluation of Orofacial Manifestations in 50 Thalassemic Patients: A Clinical StudyDocument0 pagesEvaluation of Orofacial Manifestations in 50 Thalassemic Patients: A Clinical StudyMeilinda AmeiNo ratings yet
- Ep 3Document10 pagesEp 3Mădălina ŞerbanNo ratings yet
- Jamadermatology Kridin 2021 Oi 210045 1634154542.6481Document9 pagesJamadermatology Kridin 2021 Oi 210045 1634154542.6481Nandha KumarNo ratings yet
- Ejhf 1858Document15 pagesEjhf 1858Bryan NguyenNo ratings yet
- Impact of CoffeeDocument4 pagesImpact of CoffeeBryan NguyenNo ratings yet
- Update On Heart Failure Management and Future Directions: Hong-Mi Choi, Myung-Soo Park, and Jong-Chan YounDocument33 pagesUpdate On Heart Failure Management and Future Directions: Hong-Mi Choi, Myung-Soo Park, and Jong-Chan YounBryan NguyenNo ratings yet
- 1 s2.0 S221317791200008X MainDocument5 pages1 s2.0 S221317791200008X MainBryan NguyenNo ratings yet
- Jacc: Heart Failure CmeDocument20 pagesJacc: Heart Failure CmeBryan NguyenNo ratings yet
- Unplanned Hospital Readmissions After Heartmate Ii ImplantationDocument9 pagesUnplanned Hospital Readmissions After Heartmate Ii ImplantationBryan NguyenNo ratings yet
- Clinical Implications of Abnormal Thyroid Function in Heart FailureDocument2 pagesClinical Implications of Abnormal Thyroid Function in Heart FailureBryan NguyenNo ratings yet
- MELD Exception For Liver Transplantation in Portopulmonary Hypertension: Current Implementation and Future ConsiderationsDocument3 pagesMELD Exception For Liver Transplantation in Portopulmonary Hypertension: Current Implementation and Future ConsiderationsBryan NguyenNo ratings yet
- Practice: Ulcerative Colitis: Diagnosis and ManagementDocument4 pagesPractice: Ulcerative Colitis: Diagnosis and ManagementBryan NguyenNo ratings yet
- A Randomized Controlled Trial of High-Dose Vitamin D in Patients With Heart FailureDocument7 pagesA Randomized Controlled Trial of High-Dose Vitamin D in Patients With Heart FailureBryan NguyenNo ratings yet
- Ciclosporin and Refractory Colitis.5Document6 pagesCiclosporin and Refractory Colitis.5Bryan NguyenNo ratings yet
- Aldosterone Antagonists and Outcomes in Real-World Older Patients With Heart Failure and Preserved Ejection FractionDocument8 pagesAldosterone Antagonists and Outcomes in Real-World Older Patients With Heart Failure and Preserved Ejection FractionBryan NguyenNo ratings yet
- The Future of Cardiovascular BiomedicineDocument16 pagesThe Future of Cardiovascular BiomedicineBryan NguyenNo ratings yet
- Journal Pre-Proof: International Journal of Women's DermatologyDocument18 pagesJournal Pre-Proof: International Journal of Women's DermatologyBryan NguyenNo ratings yet
- Reasons For HCV Non-Treatment in Underserved African Americans: Implications For Treatment With New TherapeuticsDocument9 pagesReasons For HCV Non-Treatment in Underserved African Americans: Implications For Treatment With New TherapeuticsBryan NguyenNo ratings yet
- Feasibility and Cost of A Telemedicine-Based Short-Term Plan For Initial Access in General Dermatology in Andalusia, SpainDocument6 pagesFeasibility and Cost of A Telemedicine-Based Short-Term Plan For Initial Access in General Dermatology in Andalusia, SpainBryan NguyenNo ratings yet
- PsoriDocument12 pagesPsoriBryan NguyenNo ratings yet
- Risk of Atrial Fibrillation According To Cancer Type: A Nationwide Population-Based StudyDocument12 pagesRisk of Atrial Fibrillation According To Cancer Type: A Nationwide Population-Based StudyBryan NguyenNo ratings yet
- A Randomized Study Comparing The Pharmacokinetics of The Potential Biosimilar PF 06438179 GP1111 With Remicade Infliximab in Healthy SubjectsDocument9 pagesA Randomized Study Comparing The Pharmacokinetics of The Potential Biosimilar PF 06438179 GP1111 With Remicade Infliximab in Healthy SubjectsBryan NguyenNo ratings yet
- International Journal of Women's Dermatology: Original ResearchDocument4 pagesInternational Journal of Women's Dermatology: Original ResearchBryan NguyenNo ratings yet
- 1 s2.0 S2352647521000538 MainDocument7 pages1 s2.0 S2352647521000538 MainBryan NguyenNo ratings yet
- Trends of The Main Bibliometric Indicators of Anais 2021 Anais BrasileirosDocument6 pagesTrends of The Main Bibliometric Indicators of Anais 2021 Anais BrasileirosBryan NguyenNo ratings yet
- International Journal of Women's DermatologyDocument3 pagesInternational Journal of Women's DermatologyBryan NguyenNo ratings yet
- The Efficacy and Safety of Sunscreen Use For The Prevention of Skin CancerDocument7 pagesThe Efficacy and Safety of Sunscreen Use For The Prevention of Skin CancerBryan NguyenNo ratings yet
- International Journal of Women's Dermatology: Letters To The EditorDocument2 pagesInternational Journal of Women's Dermatology: Letters To The EditorBryan NguyenNo ratings yet
- Beasley-Meyer2010 Article CharacterizationOfTheUVAProtecDocument9 pagesBeasley-Meyer2010 Article CharacterizationOfTheUVAProtecBryan NguyenNo ratings yet
- Queenie Drug StdyDocument11 pagesQueenie Drug StdyJonas OrbetaNo ratings yet
- Rafassal Caplets, Suppositories, Enemas CompositionDocument6 pagesRafassal Caplets, Suppositories, Enemas Compositionddandan_2No ratings yet
- Social Media As An Incubator of Personality and Behavioral Psychopathology: Symptom and Disorder Authenticity or Psychosomatic Social Contagion?Document5 pagesSocial Media As An Incubator of Personality and Behavioral Psychopathology: Symptom and Disorder Authenticity or Psychosomatic Social Contagion?IndScenNo ratings yet
- BIOLOGY: MODULE 4 Biodiversity, Evolution & Disease Notes PDFDocument10 pagesBIOLOGY: MODULE 4 Biodiversity, Evolution & Disease Notes PDFschool adressNo ratings yet
- MS Radiation & Medical Oncology Course ContentsDocument8 pagesMS Radiation & Medical Oncology Course ContentsAtih_Ul_Haq_5No ratings yet
- Jessica Le - Covid-19Document3 pagesJessica Le - Covid-19api-523306558No ratings yet
- Congenital Anomalies: Dr. Bertha Soegiarto, Sp.ADocument26 pagesCongenital Anomalies: Dr. Bertha Soegiarto, Sp.AChristine VerinaNo ratings yet
- Final Research Paper Effects of Sleep Deprivation On The Academic Performance of Senior High School StudentsDocument130 pagesFinal Research Paper Effects of Sleep Deprivation On The Academic Performance of Senior High School StudentsZyrel OtucanNo ratings yet
- Tugas Bahasa Inggris Makalah Corona - Ima Amalia Juliyantiara - 14201.12.20015 - S1 KeperawatanDocument15 pagesTugas Bahasa Inggris Makalah Corona - Ima Amalia Juliyantiara - 14201.12.20015 - S1 KeperawatanImaliaNo ratings yet
- Bagong DrugsDocument7 pagesBagong DrugsmcensoredNo ratings yet
- Oral HygieneDocument9 pagesOral Hygienesuman guptaNo ratings yet
- Pulmo TBDocument7 pagesPulmo TBglenn poddalahNo ratings yet
- Psychiatry Introductory: Study Guide ToDocument346 pagesPsychiatry Introductory: Study Guide ToMandeep morNo ratings yet
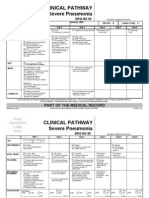
- Clinical Pathways Severe PneumoniaDocument2 pagesClinical Pathways Severe PneumoniaaandakuNo ratings yet
- Nursing Care Plan For Type1 DiabetesDocument1 pageNursing Care Plan For Type1 DiabetesBushra AlkhdourNo ratings yet
- Davainea Proglottina - A Potentially Underestimated PDFDocument3 pagesDavainea Proglottina - A Potentially Underestimated PDFryan100% (1)
- About Herbal Power Peel: Skin Care ProfessionalsDocument7 pagesAbout Herbal Power Peel: Skin Care ProfessionalsAllyna OliverosNo ratings yet
- Pathogenesis of Infectious DiseaseDocument4 pagesPathogenesis of Infectious DiseasejolibeecaldonaNo ratings yet
- Case Diagnosis For RomanDocument4 pagesCase Diagnosis For RomanChris Marie JuntillaNo ratings yet
- Leg UlcerDocument26 pagesLeg UlcerBhuiyan Ma Yousuf100% (1)
- Complete Diagnosis Coding Solution 3rd Edition Safian Test BankDocument27 pagesComplete Diagnosis Coding Solution 3rd Edition Safian Test Banktiffanykelleykjfeydwoxi100% (12)
- Complete Textbook of Phlebotomy 5th Edition by Hoeltke ISBN Solution ManualDocument13 pagesComplete Textbook of Phlebotomy 5th Edition by Hoeltke ISBN Solution Manualsook100% (29)
- Review Article: Thymoma in Myasthenia Gravis: From Diagnosis To TreatmentDocument6 pagesReview Article: Thymoma in Myasthenia Gravis: From Diagnosis To TreatmentHeru SigitNo ratings yet
- 1-Introduction MDDocument38 pages1-Introduction MDRasheena RasheeqNo ratings yet
- Case Study On Endometriosis Treatment With Siddha MedicineDocument5 pagesCase Study On Endometriosis Treatment With Siddha Medicinejuliet rubyNo ratings yet
- Nursing Care Plan (NCP)Document2 pagesNursing Care Plan (NCP)Faisa PulalonNo ratings yet
- Daftar Pustaka: 2018, Badan Penelitian Dan Pengembangan Kesehatan, KementrianDocument9 pagesDaftar Pustaka: 2018, Badan Penelitian Dan Pengembangan Kesehatan, KementrianRan NisNo ratings yet
- Disorders of The Lymphatic System: AnatomyDocument3 pagesDisorders of The Lymphatic System: AnatomyyusufNo ratings yet
- Ischemic ColitisDocument32 pagesIschemic ColitisAlex MarghescuNo ratings yet
- Non-Invasive Ablation of Cardiac ArrhythmiaDocument2 pagesNon-Invasive Ablation of Cardiac ArrhythmiaPatrick Maguire100% (1)



















































































































Download as pdf or txt
You might also like
- Oral LPDocument5 pagesOral LPkahkashanahmed065No ratings yet
- MelanomaDocument6 pagesMelanomaagung permanaNo ratings yet
- Nasopalatine Duct Cyst Restro StudyDocument8 pagesNasopalatine Duct Cyst Restro StudyTiara Oktavia SaputriNo ratings yet
- Devasconceloscarvalho 2010Document4 pagesDevasconceloscarvalho 2010Fermín GómezNo ratings yet
- Granulomatous Cheilitis: A of 6 Cases and A Review of The LiteratureDocument7 pagesGranulomatous Cheilitis: A of 6 Cases and A Review of The LiteratureAlfiatuz ZahroNo ratings yet
- Dental Panoramic Radiographic Evaluation in Bisphosphonate-Associated Osteonecrosis of The JawsDocument1 pageDental Panoramic Radiographic Evaluation in Bisphosphonate-Associated Osteonecrosis of The Jawsmateusmoreira2004No ratings yet
- Artigo 1 ParacococcidiodomicoseDocument9 pagesArtigo 1 Paracococcidiodomicoseandre.jaccoud2No ratings yet
- Lack of Association Between Celiac Disease and Dental Enamel HypoplasiaDocument6 pagesLack of Association Between Celiac Disease and Dental Enamel HypoplasiaLjubomirErdoglijaNo ratings yet
- HN 04-2011 Sublingual Gland Tumors PDFDocument6 pagesHN 04-2011 Sublingual Gland Tumors PDFHafiz FatmarNo ratings yet
- Oral Findings of Systemic Lupus Erythematosus - A Grand Round CaseDocument6 pagesOral Findings of Systemic Lupus Erythematosus - A Grand Round CaseArditya Dwi YudistiraNo ratings yet
- Oral Findings of Systemic Lupus Erythematosus-A Grand Round CaseDocument5 pagesOral Findings of Systemic Lupus Erythematosus-A Grand Round CaseIntanNo ratings yet
- Absceso CerebralDocument6 pagesAbsceso Cerebralkreacher3000No ratings yet
- JCDP 21 651Document6 pagesJCDP 21 651Diego GambinNo ratings yet
- Clinical and Pathologic Analyses of Tuberculosis in The Oral Cavity: Report of 11 CasesDocument8 pagesClinical and Pathologic Analyses of Tuberculosis in The Oral Cavity: Report of 11 CasesMaria Lozano Figueroa 5to secNo ratings yet
- 3.tahrir N. Aldelaimi Article Occurrence of Lichen Planus in Diabetes MellitusDocument4 pages3.tahrir N. Aldelaimi Article Occurrence of Lichen Planus in Diabetes MellitusMohammed AbdulhammedNo ratings yet
- Almeida Dear Ruda 2021Document23 pagesAlmeida Dear Ruda 2021pamela queirozNo ratings yet
- Original Article Retrospective Analysis of Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis Over A Period of 10 YearsDocument6 pagesOriginal Article Retrospective Analysis of Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis Over A Period of 10 YearssyalalaaalalaaaNo ratings yet
- Introduction To The Oral and Maxillofacial Pathology Focus Issue On "Preneoplastic Oral Epithelial Lesions"Document11 pagesIntroduction To The Oral and Maxillofacial Pathology Focus Issue On "Preneoplastic Oral Epithelial Lesions"jesus ulises estrada cantuNo ratings yet
- Paranasal Sinuses Malignancies: A 12-Year Review of Clinical CharacteristicsDocument5 pagesParanasal Sinuses Malignancies: A 12-Year Review of Clinical CharacteristicsRidho RifhansyahNo ratings yet
- Melkersson-Rosenthal Syndrome Revisited As A Misdiagnosed DiseaseDocument10 pagesMelkersson-Rosenthal Syndrome Revisited As A Misdiagnosed DiseasePedro NascimentoNo ratings yet
- PAPER (ENG) - The Presentation and Management of Laryngeal Cleft - A 10 Years ExperienceDocument7 pagesPAPER (ENG) - The Presentation and Management of Laryngeal Cleft - A 10 Years ExperienceAldo Hip NaranjoNo ratings yet
- Profile of Tinea Corporis and Tinea Cruris in Dermatovenereology Clinic of Tertiery Hospital: A Retrospective StudyDocument6 pagesProfile of Tinea Corporis and Tinea Cruris in Dermatovenereology Clinic of Tertiery Hospital: A Retrospective StudyRose ParkNo ratings yet
- Alotaiby Et Al, 2015Document7 pagesAlotaiby Et Al, 2015DKNo ratings yet
- 2 Olp and HPEDocument7 pages2 Olp and HPEdrnusratnaziromarNo ratings yet
- Treacher Collins Syndrome: A Systematic Review of Evidence-Based Treatment and RecommendationsDocument14 pagesTreacher Collins Syndrome: A Systematic Review of Evidence-Based Treatment and RecommendationsSai KrupaNo ratings yet
- Mucosal Melanoma of The Head and Neck 32-Year ExperienceDocument5 pagesMucosal Melanoma of The Head and Neck 32-Year ExperienceWahyu JuliandaNo ratings yet
- Expression and Distribution of Galectin-1 and Np-63/ Immuno-Histochemical Markers in Potentially Malignant Oral Disorders With and Without DysplasiaDocument7 pagesExpression and Distribution of Galectin-1 and Np-63/ Immuno-Histochemical Markers in Potentially Malignant Oral Disorders With and Without DysplasiaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Efficacy of Steroidal Vs Non-Steroidal Agents in Oral Lichen Planus: A Randomised, Open-Label StudyDocument9 pagesEfficacy of Steroidal Vs Non-Steroidal Agents in Oral Lichen Planus: A Randomised, Open-Label StudyRetno ManggalihNo ratings yet
- Primary Subacute Hematogenous Osteomyelitis in Children: A Clearer Bacteriological EtiologyDocument6 pagesPrimary Subacute Hematogenous Osteomyelitis in Children: A Clearer Bacteriological EtiologymiNo ratings yet
- SclerosingDocument5 pagesSclerosingHakan KüçükerNo ratings yet
- A Clinical and Epidemiological Study On Discoid Lupus ErythematosusDocument7 pagesA Clinical and Epidemiological Study On Discoid Lupus Erythematosusiin sakinah dewiNo ratings yet
- Jurnal PatogenesisDocument6 pagesJurnal PatogenesisErmiati EmhyNo ratings yet
- Artigo 2 - Symptomatic Meckel's Diverticulum in Children - A 12-Year Survey - 2021Document4 pagesArtigo 2 - Symptomatic Meckel's Diverticulum in Children - A 12-Year Survey - 2021Larissa RuthyelyNo ratings yet
- Chromosome 1p36 DeletionsDocument4 pagesChromosome 1p36 Deletionsericwang12No ratings yet
- Referensi Dari Saya No 8Document7 pagesReferensi Dari Saya No 8Kalsum MbNo ratings yet
- Systematic Review of Oral Manifestations Related To HyperparathyroidismDocument27 pagesSystematic Review of Oral Manifestations Related To Hyperparathyroidismanang dwiNo ratings yet
- Research ArticleDocument10 pagesResearch ArticlePratama Imanuel RawungNo ratings yet
- Patogenesis Pleomorphic AdenomaDocument6 pagesPatogenesis Pleomorphic AdenomaYeni PuspitasariNo ratings yet
- Bjorl: Clinical Diagnosis and Histological Analysis of Vocal Nodules and PolypsDocument7 pagesBjorl: Clinical Diagnosis and Histological Analysis of Vocal Nodules and PolypsRia Tupamahu MatatulaNo ratings yet
- 2022 Janas NazeDocument10 pages2022 Janas NazeazizhamoudNo ratings yet
- Enl 7Document4 pagesEnl 7Prizilia SaimimaNo ratings yet
- Maedica 18 645Document6 pagesMaedica 18 645s7ybkjhb44No ratings yet
- Hemangioma InmunohistoquimicaDocument20 pagesHemangioma InmunohistoquimicaSalome ChaconNo ratings yet
- Saini 2016 Calci NoseDocument5 pagesSaini 2016 Calci NoseRym MesfarNo ratings yet
- Ijced 3 (3) 101-109Document9 pagesIjced 3 (3) 101-109GembongSatriaMahardhikaNo ratings yet
- Profile of Tinea Corporis and Tinea Cruris in Dermatovenereology Clinic of Tertiery Hospital: A Retrospective StudyDocument6 pagesProfile of Tinea Corporis and Tinea Cruris in Dermatovenereology Clinic of Tertiery Hospital: A Retrospective StudyMarwiyahNo ratings yet
- Complications of Acute Rhinosinusitis in The Netherlands: F S Hansen, R Hoffmans, C Georgalas and W J FokkensDocument7 pagesComplications of Acute Rhinosinusitis in The Netherlands: F S Hansen, R Hoffmans, C Georgalas and W J Fokkenspanji satryo utomoNo ratings yet
- 664 8537 1 PBDocument5 pages664 8537 1 PBMICHAEL NUGROHONo ratings yet
- Chromosomal Instability, DNA Index, Dysplasia, and SubsiteDocument10 pagesChromosomal Instability, DNA Index, Dysplasia, and SubsiteManar AliNo ratings yet
- Hiperplasia Proceso CoronoidesDocument7 pagesHiperplasia Proceso CoronoidesJuan Carlos MeloNo ratings yet
- Osteosarcoma of The Jaw An Analysis of A Series of 74 Cases (2013)Document8 pagesOsteosarcoma of The Jaw An Analysis of A Series of 74 Cases (2013)sTEVENNo ratings yet
- Sebaceous Carcinoma of The Eyelids: Personal Experience With 60 CasesDocument7 pagesSebaceous Carcinoma of The Eyelids: Personal Experience With 60 CasesJocho NeavesNo ratings yet
- Prevalence and Clinical Features of Pigmented Oral LesionsDocument9 pagesPrevalence and Clinical Features of Pigmented Oral LesionsAlma AlejandraNo ratings yet
- Sjögren's Syndrome: From Pathogenesis To Novel Therapeutic TargetsDocument5 pagesSjögren's Syndrome: From Pathogenesis To Novel Therapeutic TargetsOcha24 TupamahuNo ratings yet
- Costa JOE2013Document5 pagesCosta JOE2013KristineNo ratings yet
- 13 Pediatric Follicular MucinosisDocument7 pages13 Pediatric Follicular MucinosisGi D'AtriNo ratings yet
- Evaluation of Orofacial Manifestations in 50 Thalassemic Patients: A Clinical StudyDocument0 pagesEvaluation of Orofacial Manifestations in 50 Thalassemic Patients: A Clinical StudyMeilinda AmeiNo ratings yet
- Ep 3Document10 pagesEp 3Mădălina ŞerbanNo ratings yet
- Jamadermatology Kridin 2021 Oi 210045 1634154542.6481Document9 pagesJamadermatology Kridin 2021 Oi 210045 1634154542.6481Nandha KumarNo ratings yet
- Ejhf 1858Document15 pagesEjhf 1858Bryan NguyenNo ratings yet
- Impact of CoffeeDocument4 pagesImpact of CoffeeBryan NguyenNo ratings yet
- Update On Heart Failure Management and Future Directions: Hong-Mi Choi, Myung-Soo Park, and Jong-Chan YounDocument33 pagesUpdate On Heart Failure Management and Future Directions: Hong-Mi Choi, Myung-Soo Park, and Jong-Chan YounBryan NguyenNo ratings yet
- 1 s2.0 S221317791200008X MainDocument5 pages1 s2.0 S221317791200008X MainBryan NguyenNo ratings yet
- Jacc: Heart Failure CmeDocument20 pagesJacc: Heart Failure CmeBryan NguyenNo ratings yet
- Unplanned Hospital Readmissions After Heartmate Ii ImplantationDocument9 pagesUnplanned Hospital Readmissions After Heartmate Ii ImplantationBryan NguyenNo ratings yet
- Clinical Implications of Abnormal Thyroid Function in Heart FailureDocument2 pagesClinical Implications of Abnormal Thyroid Function in Heart FailureBryan NguyenNo ratings yet
- MELD Exception For Liver Transplantation in Portopulmonary Hypertension: Current Implementation and Future ConsiderationsDocument3 pagesMELD Exception For Liver Transplantation in Portopulmonary Hypertension: Current Implementation and Future ConsiderationsBryan NguyenNo ratings yet
- Practice: Ulcerative Colitis: Diagnosis and ManagementDocument4 pagesPractice: Ulcerative Colitis: Diagnosis and ManagementBryan NguyenNo ratings yet
- A Randomized Controlled Trial of High-Dose Vitamin D in Patients With Heart FailureDocument7 pagesA Randomized Controlled Trial of High-Dose Vitamin D in Patients With Heart FailureBryan NguyenNo ratings yet
- Ciclosporin and Refractory Colitis.5Document6 pagesCiclosporin and Refractory Colitis.5Bryan NguyenNo ratings yet
- Aldosterone Antagonists and Outcomes in Real-World Older Patients With Heart Failure and Preserved Ejection FractionDocument8 pagesAldosterone Antagonists and Outcomes in Real-World Older Patients With Heart Failure and Preserved Ejection FractionBryan NguyenNo ratings yet
- The Future of Cardiovascular BiomedicineDocument16 pagesThe Future of Cardiovascular BiomedicineBryan NguyenNo ratings yet
- Journal Pre-Proof: International Journal of Women's DermatologyDocument18 pagesJournal Pre-Proof: International Journal of Women's DermatologyBryan NguyenNo ratings yet
- Reasons For HCV Non-Treatment in Underserved African Americans: Implications For Treatment With New TherapeuticsDocument9 pagesReasons For HCV Non-Treatment in Underserved African Americans: Implications For Treatment With New TherapeuticsBryan NguyenNo ratings yet
- Feasibility and Cost of A Telemedicine-Based Short-Term Plan For Initial Access in General Dermatology in Andalusia, SpainDocument6 pagesFeasibility and Cost of A Telemedicine-Based Short-Term Plan For Initial Access in General Dermatology in Andalusia, SpainBryan NguyenNo ratings yet
- PsoriDocument12 pagesPsoriBryan NguyenNo ratings yet
- Risk of Atrial Fibrillation According To Cancer Type: A Nationwide Population-Based StudyDocument12 pagesRisk of Atrial Fibrillation According To Cancer Type: A Nationwide Population-Based StudyBryan NguyenNo ratings yet
- A Randomized Study Comparing The Pharmacokinetics of The Potential Biosimilar PF 06438179 GP1111 With Remicade Infliximab in Healthy SubjectsDocument9 pagesA Randomized Study Comparing The Pharmacokinetics of The Potential Biosimilar PF 06438179 GP1111 With Remicade Infliximab in Healthy SubjectsBryan NguyenNo ratings yet
- International Journal of Women's Dermatology: Original ResearchDocument4 pagesInternational Journal of Women's Dermatology: Original ResearchBryan NguyenNo ratings yet
- 1 s2.0 S2352647521000538 MainDocument7 pages1 s2.0 S2352647521000538 MainBryan NguyenNo ratings yet
- Trends of The Main Bibliometric Indicators of Anais 2021 Anais BrasileirosDocument6 pagesTrends of The Main Bibliometric Indicators of Anais 2021 Anais BrasileirosBryan NguyenNo ratings yet
- International Journal of Women's DermatologyDocument3 pagesInternational Journal of Women's DermatologyBryan NguyenNo ratings yet
- The Efficacy and Safety of Sunscreen Use For The Prevention of Skin CancerDocument7 pagesThe Efficacy and Safety of Sunscreen Use For The Prevention of Skin CancerBryan NguyenNo ratings yet
- International Journal of Women's Dermatology: Letters To The EditorDocument2 pagesInternational Journal of Women's Dermatology: Letters To The EditorBryan NguyenNo ratings yet
- Beasley-Meyer2010 Article CharacterizationOfTheUVAProtecDocument9 pagesBeasley-Meyer2010 Article CharacterizationOfTheUVAProtecBryan NguyenNo ratings yet
- Queenie Drug StdyDocument11 pagesQueenie Drug StdyJonas OrbetaNo ratings yet
- Rafassal Caplets, Suppositories, Enemas CompositionDocument6 pagesRafassal Caplets, Suppositories, Enemas Compositionddandan_2No ratings yet
- Social Media As An Incubator of Personality and Behavioral Psychopathology: Symptom and Disorder Authenticity or Psychosomatic Social Contagion?Document5 pagesSocial Media As An Incubator of Personality and Behavioral Psychopathology: Symptom and Disorder Authenticity or Psychosomatic Social Contagion?IndScenNo ratings yet
- BIOLOGY: MODULE 4 Biodiversity, Evolution & Disease Notes PDFDocument10 pagesBIOLOGY: MODULE 4 Biodiversity, Evolution & Disease Notes PDFschool adressNo ratings yet
- MS Radiation & Medical Oncology Course ContentsDocument8 pagesMS Radiation & Medical Oncology Course ContentsAtih_Ul_Haq_5No ratings yet
- Jessica Le - Covid-19Document3 pagesJessica Le - Covid-19api-523306558No ratings yet
- Congenital Anomalies: Dr. Bertha Soegiarto, Sp.ADocument26 pagesCongenital Anomalies: Dr. Bertha Soegiarto, Sp.AChristine VerinaNo ratings yet
- Final Research Paper Effects of Sleep Deprivation On The Academic Performance of Senior High School StudentsDocument130 pagesFinal Research Paper Effects of Sleep Deprivation On The Academic Performance of Senior High School StudentsZyrel OtucanNo ratings yet
- Tugas Bahasa Inggris Makalah Corona - Ima Amalia Juliyantiara - 14201.12.20015 - S1 KeperawatanDocument15 pagesTugas Bahasa Inggris Makalah Corona - Ima Amalia Juliyantiara - 14201.12.20015 - S1 KeperawatanImaliaNo ratings yet
- Bagong DrugsDocument7 pagesBagong DrugsmcensoredNo ratings yet
- Oral HygieneDocument9 pagesOral Hygienesuman guptaNo ratings yet
- Pulmo TBDocument7 pagesPulmo TBglenn poddalahNo ratings yet
- Psychiatry Introductory: Study Guide ToDocument346 pagesPsychiatry Introductory: Study Guide ToMandeep morNo ratings yet
- Clinical Pathways Severe PneumoniaDocument2 pagesClinical Pathways Severe PneumoniaaandakuNo ratings yet
- Nursing Care Plan For Type1 DiabetesDocument1 pageNursing Care Plan For Type1 DiabetesBushra AlkhdourNo ratings yet
- Davainea Proglottina - A Potentially Underestimated PDFDocument3 pagesDavainea Proglottina - A Potentially Underestimated PDFryan100% (1)
- About Herbal Power Peel: Skin Care ProfessionalsDocument7 pagesAbout Herbal Power Peel: Skin Care ProfessionalsAllyna OliverosNo ratings yet
- Pathogenesis of Infectious DiseaseDocument4 pagesPathogenesis of Infectious DiseasejolibeecaldonaNo ratings yet
- Case Diagnosis For RomanDocument4 pagesCase Diagnosis For RomanChris Marie JuntillaNo ratings yet
- Leg UlcerDocument26 pagesLeg UlcerBhuiyan Ma Yousuf100% (1)
- Complete Diagnosis Coding Solution 3rd Edition Safian Test BankDocument27 pagesComplete Diagnosis Coding Solution 3rd Edition Safian Test Banktiffanykelleykjfeydwoxi100% (12)
- Complete Textbook of Phlebotomy 5th Edition by Hoeltke ISBN Solution ManualDocument13 pagesComplete Textbook of Phlebotomy 5th Edition by Hoeltke ISBN Solution Manualsook100% (29)
- Review Article: Thymoma in Myasthenia Gravis: From Diagnosis To TreatmentDocument6 pagesReview Article: Thymoma in Myasthenia Gravis: From Diagnosis To TreatmentHeru SigitNo ratings yet
- 1-Introduction MDDocument38 pages1-Introduction MDRasheena RasheeqNo ratings yet
- Case Study On Endometriosis Treatment With Siddha MedicineDocument5 pagesCase Study On Endometriosis Treatment With Siddha Medicinejuliet rubyNo ratings yet
- Nursing Care Plan (NCP)Document2 pagesNursing Care Plan (NCP)Faisa PulalonNo ratings yet
- Daftar Pustaka: 2018, Badan Penelitian Dan Pengembangan Kesehatan, KementrianDocument9 pagesDaftar Pustaka: 2018, Badan Penelitian Dan Pengembangan Kesehatan, KementrianRan NisNo ratings yet
- Disorders of The Lymphatic System: AnatomyDocument3 pagesDisorders of The Lymphatic System: AnatomyyusufNo ratings yet
- Ischemic ColitisDocument32 pagesIschemic ColitisAlex MarghescuNo ratings yet
- Non-Invasive Ablation of Cardiac ArrhythmiaDocument2 pagesNon-Invasive Ablation of Cardiac ArrhythmiaPatrick Maguire100% (1)