Download as docx, pdf, or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5834)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- Chance Moilwa Book 2 by Emmie Motsamai TheoDocument1,251 pagesChance Moilwa Book 2 by Emmie Motsamai TheomsimangslindiweNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Sally Case Study Handout PDFDocument2 pagesSally Case Study Handout PDFRatus BornNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Its Your Move Participants HANDBOOKDocument24 pagesIts Your Move Participants HANDBOOKRatus BornNo ratings yet
- Student Handbook PN - AUG 2020Document46 pagesStudent Handbook PN - AUG 2020Ratus BornNo ratings yet
- It's Your Move E-Learning Course InstructionsDocument2 pagesIt's Your Move E-Learning Course InstructionsRatus BornNo ratings yet
- It's Your: Functional Assessment AlgorithmDocument1 pageIt's Your: Functional Assessment AlgorithmRatus BornNo ratings yet
- Braden ScaleDocument1 pageBraden ScaleRatus BornNo ratings yet
- A Unique Thermodynamics Course With LaboratoriesDocument24 pagesA Unique Thermodynamics Course With LaboratoriesRatus BornNo ratings yet
- 10 Rights of Medication AdministrationDocument1 page10 Rights of Medication AdministrationRatus BornNo ratings yet
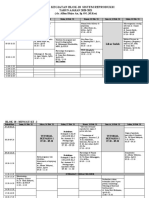
- Jadwal Kegiatan Blok-18 Sistem ReproduksiDocument7 pagesJadwal Kegiatan Blok-18 Sistem Reproduksiicha chanNo ratings yet
- Tocilizumab CovidDocument15 pagesTocilizumab CovidAponte MaríaNo ratings yet
- Anand Dhoka - AB - Numerology ReportDocument82 pagesAnand Dhoka - AB - Numerology ReportTaththasttuNo ratings yet
- Effect of Congenital Heart Disease On Child Growth: Dr. Deia K Khalaf, Dr. Yusra K Al-Rawi and Dr. Laith A Abdul HadiDocument7 pagesEffect of Congenital Heart Disease On Child Growth: Dr. Deia K Khalaf, Dr. Yusra K Al-Rawi and Dr. Laith A Abdul HadimuhammadrikiNo ratings yet
- Potato Diseases: I D E N T I F Y I N GDocument30 pagesPotato Diseases: I D E N T I F Y I N GMaria CiucaNo ratings yet
- Spinal Cord Syndrome Case PresentationDocument53 pagesSpinal Cord Syndrome Case PresentationPermata GBKP Runggun SurabayaNo ratings yet
- Oral Health PromotionDocument11 pagesOral Health PromotionIGN 1SNo ratings yet
- Loresca - Ratio Mtle - HistopathDocument10 pagesLoresca - Ratio Mtle - HistopathKaycee Gretz LorescaNo ratings yet
- Mengapa Biosecurity Menjadi Penting Pada Laboratorium Penyakit Infeksi ?Document10 pagesMengapa Biosecurity Menjadi Penting Pada Laboratorium Penyakit Infeksi ?AndyNo ratings yet
- VARICOSE VEINS .BY DR BasharatDocument94 pagesVARICOSE VEINS .BY DR BasharatMohammad NomanNo ratings yet
- Final Exam MS QuestionsDocument26 pagesFinal Exam MS QuestionsChandler GarrettNo ratings yet
- Raynaud's Disease & Buerger's Disease: Submitted ToDocument11 pagesRaynaud's Disease & Buerger's Disease: Submitted ToKathleen Leana Viray JeanjaquetNo ratings yet
- Isolation and Detection of Staphylococcus Aureus in Foods: Shannen Krishna S. Sena Group 2, Sec. B-1LDocument13 pagesIsolation and Detection of Staphylococcus Aureus in Foods: Shannen Krishna S. Sena Group 2, Sec. B-1LShannen SenaNo ratings yet
- Health Belief Model UpdateDocument15 pagesHealth Belief Model Updatejust nomiNo ratings yet
- HPIM 20 OncologyDocument244 pagesHPIM 20 OncologyapeachNo ratings yet
- Multiple and Mixed Valvular Heart DiseaseDocument13 pagesMultiple and Mixed Valvular Heart DiseaseВенцислав МирчевNo ratings yet
- The Scale of Perceived Occupational StressDocument6 pagesThe Scale of Perceived Occupational StressPranay PandeyNo ratings yet
- Chronic Fatigue Syndrome: Evaluation and TreatmentDocument8 pagesChronic Fatigue Syndrome: Evaluation and TreatmentmeiraimNo ratings yet
- Brain Tumors: Primary BTDocument5 pagesBrain Tumors: Primary BTMohamed Al-zichrawyNo ratings yet
- MPH Program in UP ManilaDocument2 pagesMPH Program in UP ManilaHannah Marquiala PellejoNo ratings yet
- English 18D-NLS Features and WarrantyDocument10 pagesEnglish 18D-NLS Features and Warrantytao_vk6027No ratings yet
- Evidence-Based Practice Project: Diabetes Diet Management: Stephanie Green NUR - 590Document20 pagesEvidence-Based Practice Project: Diabetes Diet Management: Stephanie Green NUR - 590dennis ndegeNo ratings yet
- Tle9agricrop q1 m2 L1 - Undertakinghorticulturalproductionworkasdirected v2Document27 pagesTle9agricrop q1 m2 L1 - Undertakinghorticulturalproductionworkasdirected v2marvic daleonNo ratings yet
- Jurnal Massage For Infantile ColicDocument10 pagesJurnal Massage For Infantile ColicrambuubeNo ratings yet
- Disinfection and Sterilization in Health Care Facilities: What Clinicians Need To KnowDocument8 pagesDisinfection and Sterilization in Health Care Facilities: What Clinicians Need To KnowAyu AndrianiNo ratings yet
- Accreditation No.: 1030-091918-093Document4 pagesAccreditation No.: 1030-091918-093Leo Buquiran AcabalNo ratings yet
- The Physical FitnessDocument37 pagesThe Physical FitnessMIGUELA SP. SANTIAGONo ratings yet
- Hubungan Karakteristik Individu Dan Iklim Kerja Dengan Keluhan Msds Pada Pekerja Perakitan Mini Bus Di PT Mekar Armada Jaya MagelangDocument11 pagesHubungan Karakteristik Individu Dan Iklim Kerja Dengan Keluhan Msds Pada Pekerja Perakitan Mini Bus Di PT Mekar Armada Jaya MagelangDewi SiregarNo ratings yet
- Comparison of The Efficacy and Safety of GlimepiriDocument6 pagesComparison of The Efficacy and Safety of GlimepirinnNo ratings yet