
Amblyopia - An Update: Review
Amblyopia - An Update: Review
You might also like
- Sir Imran SynopsisDocument13 pagesSir Imran Synopsismethoo143No ratings yet
- Human Anatomy and Physiology For NursesDocument48 pagesHuman Anatomy and Physiology For NursesKelly J Wilson86% (22)
- Biology Investigatory Project On Eye DiseasesDocument18 pagesBiology Investigatory Project On Eye DiseasesBHALAJI KARUNANITHI100% (1)
- BIOLOGY INVESTIGATORY - Docx2.oDocument27 pagesBIOLOGY INVESTIGATORY - Docx2.oK GhatageNo ratings yet
- Looking Beyond Occlusion - A Novel Perspective For Amblyopia TreatmentDocument5 pagesLooking Beyond Occlusion - A Novel Perspective For Amblyopia TreatmentPacoNo ratings yet
- Bio Khushil 12Document23 pagesBio Khushil 12khushilgajpal2007No ratings yet
- Influence of Contact Lenses On The Binocular VisionDocument11 pagesInfluence of Contact Lenses On The Binocular VisionGian Carlo Giusto BurboaNo ratings yet
- Current Management of Childhood Amblyopia: Shin Hae ParkDocument12 pagesCurrent Management of Childhood Amblyopia: Shin Hae ParkSyarifah Thalita NabillaNo ratings yet
- Current Developments in The Management of Amblyopia With The Use of Perceptual Learning TechniquesDocument19 pagesCurrent Developments in The Management of Amblyopia With The Use of Perceptual Learning TechniquesRael RodriguesNo ratings yet
- Understanding Low Functioning Cerebral Visual ImpairmentDocument8 pagesUnderstanding Low Functioning Cerebral Visual ImpairmentShobithaNo ratings yet
- 1 s2.0 S2352396421001535 MainDocument13 pages1 s2.0 S2352396421001535 MainAmy Lalringhluani ChhakchhuakNo ratings yet
- Childhood Amblyopia: Current Management and New Trends: Invited ReviewDocument12 pagesChildhood Amblyopia: Current Management and New Trends: Invited ReviewVrishab KrishnaNo ratings yet
- Murray 2019Document13 pagesMurray 2019ayuputriNo ratings yet
- Investrigatory Project (Term I) : Subject - BIOLOGYDocument20 pagesInvestrigatory Project (Term I) : Subject - BIOLOGYRehan RazaNo ratings yet
- Biology Investigatory ProjectDocument19 pagesBiology Investigatory ProjectGopikrishna united67% (3)
- Name - Krishna Chouhan CLASS - 12th B: Kendriya Vidyalaya No.2 IndoreDocument11 pagesName - Krishna Chouhan CLASS - 12th B: Kendriya Vidyalaya No.2 IndoreKrishna ChouhanNo ratings yet
- Visual Disorders in Children With Cerebral Palsy TDocument11 pagesVisual Disorders in Children With Cerebral Palsy TShobithaNo ratings yet
- Project 220209165249Document32 pagesProject 220209165249Lakshmanan RNo ratings yet
- Cet 5Document4 pagesCet 5jumi26No ratings yet
- Squint: BackgroundDocument8 pagesSquint: BackgroundRebecca WongNo ratings yet
- Cause of Amblyopia in Adult Patients A Cross-Sectional StudyDocument5 pagesCause of Amblyopia in Adult Patients A Cross-Sectional StudyRagni Mishra100% (2)
- Ophthalmic Physiologic Optic - 2019 - McGraw - Optical Treatment of Strabismic AmblyopiaDocument4 pagesOphthalmic Physiologic Optic - 2019 - McGraw - Optical Treatment of Strabismic AmblyopiaNisrina Hamid AlbahreisyNo ratings yet
- Nihms 1622781Document31 pagesNihms 1622781Nisrina Hamid AlbahreisyNo ratings yet
- The Gradual Loss of VisionDocument9 pagesThe Gradual Loss of VisionWALID HOSSAINNo ratings yet
- Biology Investigatory Project: Samiksha Subhashish SarkarDocument35 pagesBiology Investigatory Project: Samiksha Subhashish SarkarSamiksha SarkarNo ratings yet
- Binocular Single VisionDocument9 pagesBinocular Single VisionMarcelKorevaarNo ratings yet
- A Case Presentation of CataractDocument16 pagesA Case Presentation of CataractDoneva Lyn Medina100% (1)
- A Window Into Visual Cortex Development and Recovery of Vision - 2015 - VisionDocument3 pagesA Window Into Visual Cortex Development and Recovery of Vision - 2015 - VisionOana BatrinuNo ratings yet
- Ocular Disorders in The NewbornDocument11 pagesOcular Disorders in The NewbornXimena ParedesNo ratings yet
- How Far Is Observation Allowed in Patients With Ectopia Lentis?Document8 pagesHow Far Is Observation Allowed in Patients With Ectopia Lentis?Syeda F AmbreenNo ratings yet
- Abnormal Fixational Eye Movements in Amblyopia: PurposeDocument17 pagesAbnormal Fixational Eye Movements in Amblyopia: PurposeLinda MutiaraNo ratings yet
- Mata - AmblyopiaDocument30 pagesMata - AmblyopiarabinreaganNo ratings yet
- Pedia OphthaDocument29 pagesPedia OphthajeffaguilarNo ratings yet
- ocular deliveryDocument29 pagesocular deliveryKushagra GoyalNo ratings yet
- Fellow Eye Deficits in AmblyopiaDocument11 pagesFellow Eye Deficits in AmblyopiaJavier Ríos OrtegaNo ratings yet
- Age-Related Cataract & GlaucomaDocument26 pagesAge-Related Cataract & Glaucomasweetyeyal2002No ratings yet
- Munim 2022Document4 pagesMunim 2022febyolaNo ratings yet
- Appropriate Terminology For CVI.Document6 pagesAppropriate Terminology For CVI.ShobithaNo ratings yet
- Reviews in Clinical GerontologyDocument18 pagesReviews in Clinical GerontologyRADYA PUTRA PRATAMANo ratings yet
- WPR 2Document5 pagesWPR 2ishika mohanNo ratings yet
- Cortical Visual Impairment: Pediatrics in Review November 2009Document13 pagesCortical Visual Impairment: Pediatrics in Review November 2009Amal AlmutiriNo ratings yet
- Clinical and Experimental Advances in Congenital and Paediatric CataractsDocument16 pagesClinical and Experimental Advances in Congenital and Paediatric CataractsFitri Amelia RizkiNo ratings yet
- TBL 1 - Refractive Error SlidesDocument66 pagesTBL 1 - Refractive Error SlidesAmirah Azman100% (4)
- Refractive Errors: Current Thinking: ArticleDocument7 pagesRefractive Errors: Current Thinking: ArticleJabbarTapiheruNo ratings yet
- Senile Cataract (Age-Related Cataract) - Practice Essentials, Background, PathophysiologyDocument5 pagesSenile Cataract (Age-Related Cataract) - Practice Essentials, Background, PathophysiologyAhmad FahroziNo ratings yet
- Med2 Xing HannahDocument6 pagesMed2 Xing HannahCharlotte YeoNo ratings yet
- Eye Diseases: An Investigatory Project by Shrikanth Pillai XII BDocument11 pagesEye Diseases: An Investigatory Project by Shrikanth Pillai XII BCR7STUDIO 7100% (1)
- Final TouchDocument49 pagesFinal TouchmalathiNo ratings yet
- AmblyopiaDocument10 pagesAmblyopiaNoura RoseNo ratings yet
- Clinical Profile of Accommodative Dysfunction in Different Stages of MyopiaDocument4 pagesClinical Profile of Accommodative Dysfunction in Different Stages of MyopiaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 21-29 Clinical+Characteristics+of+Children+With+Refractive+Amblyopia+at+Cipto+Mangunkusumo+National+Referral+Hospital Rev1Document9 pages21-29 Clinical+Characteristics+of+Children+With+Refractive+Amblyopia+at+Cipto+Mangunkusumo+National+Referral+Hospital Rev1firmianisaNo ratings yet
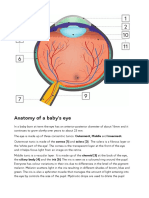
- Anatomy of A Baby's Eye: Outermost, Middle and Innermost. Cornea (1) and Sclera (2) - The Sclera Is A Fibrous Layer orDocument2 pagesAnatomy of A Baby's Eye: Outermost, Middle and Innermost. Cornea (1) and Sclera (2) - The Sclera Is A Fibrous Layer orSandor GyongyverNo ratings yet
- IndianJOphthalmol65101030-3506303 094423Document3 pagesIndianJOphthalmol65101030-3506303 094423Asif Faraz NasirNo ratings yet
- Ref Error ChildrenDocument3 pagesRef Error ChildrenAdriana gonzalezNo ratings yet
- Optical Coherence Tomography Findings of Falciform Retinal Detachment Complicated With Persistent Fetal VasculatureDocument5 pagesOptical Coherence Tomography Findings of Falciform Retinal Detachment Complicated With Persistent Fetal VasculatureAgus SaifudinNo ratings yet
- Cortical Reorganization After Optical Alignment in Strabismic Patients Outside of Critical PeriodDocument13 pagesCortical Reorganization After Optical Alignment in Strabismic Patients Outside of Critical PeriodJonathan GrandasNo ratings yet
- Background: FrequencyDocument10 pagesBackground: FrequencyJenylia HapsariNo ratings yet
- A Rare Presentation of Esotropia in High Myopia in A Young AdultDocument3 pagesA Rare Presentation of Esotropia in High Myopia in A Young AdultTinara HusniaNo ratings yet
- Gilbert y Wu Li, 2012Document7 pagesGilbert y Wu Li, 2012Sara GRNo ratings yet
- Optical Correction of Aphakia in Children: Review ArticleDocument12 pagesOptical Correction of Aphakia in Children: Review Articleaisa mutiaraNo ratings yet
- Barangay Annual Gender and Development (Gad) Plan and BudgetDocument2 pagesBarangay Annual Gender and Development (Gad) Plan and BudgetYham-Lloyd AbordoNo ratings yet
- Accuracy of The Demirjian and Willems MethodsDocument8 pagesAccuracy of The Demirjian and Willems MethodsProfessor T. A. EsanNo ratings yet
- Focus Group Design and Group Dynamics: Lessons From Deaf and Hard of Hearing ParticipantsDocument5 pagesFocus Group Design and Group Dynamics: Lessons From Deaf and Hard of Hearing ParticipantsmeeehNo ratings yet
- 为什么饮食失调很难治疗Document4 pages为什么饮食失调很难治疗Victoria TangNo ratings yet
- The Ainorian CompendiumDocument300 pagesThe Ainorian Compendiumlennoxmurray60100% (3)
- Nejmcp 1903768Document9 pagesNejmcp 1903768EriC. ChaN.No ratings yet
- Price List ABC 28-9-2022Document13 pagesPrice List ABC 28-9-2022NgurahNo ratings yet
- Monitoring and Evaluation FormDocument5 pagesMonitoring and Evaluation Formlesterjessa castroNo ratings yet
- TN BH ABA Provider OrientationDocument34 pagesTN BH ABA Provider OrientationVivian ChenNo ratings yet
- Uma Co., Ltd. Hba1C Diluent: 2-19-6 Yokosuka Matsudo, Chiba, JapanDocument1 pageUma Co., Ltd. Hba1C Diluent: 2-19-6 Yokosuka Matsudo, Chiba, JapanTrần Văn BìnhNo ratings yet
- Yours Uk 12 March 2023Document126 pagesYours Uk 12 March 2023turricanNo ratings yet
- ADEA AADSAS General Instructions BookletDocument53 pagesADEA AADSAS General Instructions Bookletd_yuminNo ratings yet
- Love Letter PDFDocument31 pagesLove Letter PDFAlan Kintanar IIINo ratings yet
- Đề số 1Document4 pagesĐề số 1LanChiVũ0% (1)
- Resumo - SIICUSP - Ingles FinalDocument2 pagesResumo - SIICUSP - Ingles FinalSuel CostaNo ratings yet
- Reconstruction of The EarDocument10 pagesReconstruction of The EarFabian Camelo OtorrinoNo ratings yet
- Pe G 12 Melc12 2Document5 pagesPe G 12 Melc12 2Ivy Dianne Pascual100% (5)
- Advanced Nutrition Test 2023 PDFDocument3 pagesAdvanced Nutrition Test 2023 PDFajjaNo ratings yet
- Hazard Analysis and Risk Control Record: Schlumberger-PrivateDocument2 pagesHazard Analysis and Risk Control Record: Schlumberger-Privatehans vatriolisNo ratings yet
- Assignment Individual Section 42Document3 pagesAssignment Individual Section 42Afiqah YusriNo ratings yet
- Heal TH 2019 Research On Drugs Abuse - 2Document140 pagesHeal TH 2019 Research On Drugs Abuse - 2Anti NarkobaNo ratings yet
- Thesis Topics Conservative Dentistry EndodonticsDocument5 pagesThesis Topics Conservative Dentistry Endodonticsaprilfordsavannah100% (2)
- School Violence InInternational ContexDocument257 pagesSchool Violence InInternational ContexLUZ STELLA MOSQUERANo ratings yet
- Study On The Effectiveness of Using Homemade Coconut Milk With Aloe Vera As Hair ConditionerDocument9 pagesStudy On The Effectiveness of Using Homemade Coconut Milk With Aloe Vera As Hair ConditionerFrederick SantosNo ratings yet
- LOA 3rd Quarter TemplateDocument4 pagesLOA 3rd Quarter TemplateJALENE L. MASAGCANo ratings yet
- ASS Event 2-Documentation, Planning and Assessment 2Document13 pagesASS Event 2-Documentation, Planning and Assessment 2Liz LopezNo ratings yet
- Wib Brochure enDocument2 pagesWib Brochure enedsan alinsuagNo ratings yet
- Nutrition: Food Based Dietary GuidelinesDocument19 pagesNutrition: Food Based Dietary GuidelinesAbdi Khalaq Ali HashiNo ratings yet
- Ig2-Mohsin Bashir Report 2Document13 pagesIg2-Mohsin Bashir Report 2Mohsin BashirNo ratings yet

























































































Download as pdf or txt
You might also like
- Sir Imran SynopsisDocument13 pagesSir Imran Synopsismethoo143No ratings yet
- Human Anatomy and Physiology For NursesDocument48 pagesHuman Anatomy and Physiology For NursesKelly J Wilson86% (22)
- Biology Investigatory Project On Eye DiseasesDocument18 pagesBiology Investigatory Project On Eye DiseasesBHALAJI KARUNANITHI100% (1)
- BIOLOGY INVESTIGATORY - Docx2.oDocument27 pagesBIOLOGY INVESTIGATORY - Docx2.oK GhatageNo ratings yet
- Looking Beyond Occlusion - A Novel Perspective For Amblyopia TreatmentDocument5 pagesLooking Beyond Occlusion - A Novel Perspective For Amblyopia TreatmentPacoNo ratings yet
- Bio Khushil 12Document23 pagesBio Khushil 12khushilgajpal2007No ratings yet
- Influence of Contact Lenses On The Binocular VisionDocument11 pagesInfluence of Contact Lenses On The Binocular VisionGian Carlo Giusto BurboaNo ratings yet
- Current Management of Childhood Amblyopia: Shin Hae ParkDocument12 pagesCurrent Management of Childhood Amblyopia: Shin Hae ParkSyarifah Thalita NabillaNo ratings yet
- Current Developments in The Management of Amblyopia With The Use of Perceptual Learning TechniquesDocument19 pagesCurrent Developments in The Management of Amblyopia With The Use of Perceptual Learning TechniquesRael RodriguesNo ratings yet
- Understanding Low Functioning Cerebral Visual ImpairmentDocument8 pagesUnderstanding Low Functioning Cerebral Visual ImpairmentShobithaNo ratings yet
- 1 s2.0 S2352396421001535 MainDocument13 pages1 s2.0 S2352396421001535 MainAmy Lalringhluani ChhakchhuakNo ratings yet
- Childhood Amblyopia: Current Management and New Trends: Invited ReviewDocument12 pagesChildhood Amblyopia: Current Management and New Trends: Invited ReviewVrishab KrishnaNo ratings yet
- Murray 2019Document13 pagesMurray 2019ayuputriNo ratings yet
- Investrigatory Project (Term I) : Subject - BIOLOGYDocument20 pagesInvestrigatory Project (Term I) : Subject - BIOLOGYRehan RazaNo ratings yet
- Biology Investigatory ProjectDocument19 pagesBiology Investigatory ProjectGopikrishna united67% (3)
- Name - Krishna Chouhan CLASS - 12th B: Kendriya Vidyalaya No.2 IndoreDocument11 pagesName - Krishna Chouhan CLASS - 12th B: Kendriya Vidyalaya No.2 IndoreKrishna ChouhanNo ratings yet
- Visual Disorders in Children With Cerebral Palsy TDocument11 pagesVisual Disorders in Children With Cerebral Palsy TShobithaNo ratings yet
- Project 220209165249Document32 pagesProject 220209165249Lakshmanan RNo ratings yet
- Cet 5Document4 pagesCet 5jumi26No ratings yet
- Squint: BackgroundDocument8 pagesSquint: BackgroundRebecca WongNo ratings yet
- Cause of Amblyopia in Adult Patients A Cross-Sectional StudyDocument5 pagesCause of Amblyopia in Adult Patients A Cross-Sectional StudyRagni Mishra100% (2)
- Ophthalmic Physiologic Optic - 2019 - McGraw - Optical Treatment of Strabismic AmblyopiaDocument4 pagesOphthalmic Physiologic Optic - 2019 - McGraw - Optical Treatment of Strabismic AmblyopiaNisrina Hamid AlbahreisyNo ratings yet
- Nihms 1622781Document31 pagesNihms 1622781Nisrina Hamid AlbahreisyNo ratings yet
- The Gradual Loss of VisionDocument9 pagesThe Gradual Loss of VisionWALID HOSSAINNo ratings yet
- Biology Investigatory Project: Samiksha Subhashish SarkarDocument35 pagesBiology Investigatory Project: Samiksha Subhashish SarkarSamiksha SarkarNo ratings yet
- Binocular Single VisionDocument9 pagesBinocular Single VisionMarcelKorevaarNo ratings yet
- A Case Presentation of CataractDocument16 pagesA Case Presentation of CataractDoneva Lyn Medina100% (1)
- A Window Into Visual Cortex Development and Recovery of Vision - 2015 - VisionDocument3 pagesA Window Into Visual Cortex Development and Recovery of Vision - 2015 - VisionOana BatrinuNo ratings yet
- Ocular Disorders in The NewbornDocument11 pagesOcular Disorders in The NewbornXimena ParedesNo ratings yet
- How Far Is Observation Allowed in Patients With Ectopia Lentis?Document8 pagesHow Far Is Observation Allowed in Patients With Ectopia Lentis?Syeda F AmbreenNo ratings yet
- Abnormal Fixational Eye Movements in Amblyopia: PurposeDocument17 pagesAbnormal Fixational Eye Movements in Amblyopia: PurposeLinda MutiaraNo ratings yet
- Mata - AmblyopiaDocument30 pagesMata - AmblyopiarabinreaganNo ratings yet
- Pedia OphthaDocument29 pagesPedia OphthajeffaguilarNo ratings yet
- ocular deliveryDocument29 pagesocular deliveryKushagra GoyalNo ratings yet
- Fellow Eye Deficits in AmblyopiaDocument11 pagesFellow Eye Deficits in AmblyopiaJavier Ríos OrtegaNo ratings yet
- Age-Related Cataract & GlaucomaDocument26 pagesAge-Related Cataract & Glaucomasweetyeyal2002No ratings yet
- Munim 2022Document4 pagesMunim 2022febyolaNo ratings yet
- Appropriate Terminology For CVI.Document6 pagesAppropriate Terminology For CVI.ShobithaNo ratings yet
- Reviews in Clinical GerontologyDocument18 pagesReviews in Clinical GerontologyRADYA PUTRA PRATAMANo ratings yet
- WPR 2Document5 pagesWPR 2ishika mohanNo ratings yet
- Cortical Visual Impairment: Pediatrics in Review November 2009Document13 pagesCortical Visual Impairment: Pediatrics in Review November 2009Amal AlmutiriNo ratings yet
- Clinical and Experimental Advances in Congenital and Paediatric CataractsDocument16 pagesClinical and Experimental Advances in Congenital and Paediatric CataractsFitri Amelia RizkiNo ratings yet
- TBL 1 - Refractive Error SlidesDocument66 pagesTBL 1 - Refractive Error SlidesAmirah Azman100% (4)
- Refractive Errors: Current Thinking: ArticleDocument7 pagesRefractive Errors: Current Thinking: ArticleJabbarTapiheruNo ratings yet
- Senile Cataract (Age-Related Cataract) - Practice Essentials, Background, PathophysiologyDocument5 pagesSenile Cataract (Age-Related Cataract) - Practice Essentials, Background, PathophysiologyAhmad FahroziNo ratings yet
- Med2 Xing HannahDocument6 pagesMed2 Xing HannahCharlotte YeoNo ratings yet
- Eye Diseases: An Investigatory Project by Shrikanth Pillai XII BDocument11 pagesEye Diseases: An Investigatory Project by Shrikanth Pillai XII BCR7STUDIO 7100% (1)
- Final TouchDocument49 pagesFinal TouchmalathiNo ratings yet
- AmblyopiaDocument10 pagesAmblyopiaNoura RoseNo ratings yet
- Clinical Profile of Accommodative Dysfunction in Different Stages of MyopiaDocument4 pagesClinical Profile of Accommodative Dysfunction in Different Stages of MyopiaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 21-29 Clinical+Characteristics+of+Children+With+Refractive+Amblyopia+at+Cipto+Mangunkusumo+National+Referral+Hospital Rev1Document9 pages21-29 Clinical+Characteristics+of+Children+With+Refractive+Amblyopia+at+Cipto+Mangunkusumo+National+Referral+Hospital Rev1firmianisaNo ratings yet
- Anatomy of A Baby's Eye: Outermost, Middle and Innermost. Cornea (1) and Sclera (2) - The Sclera Is A Fibrous Layer orDocument2 pagesAnatomy of A Baby's Eye: Outermost, Middle and Innermost. Cornea (1) and Sclera (2) - The Sclera Is A Fibrous Layer orSandor GyongyverNo ratings yet
- IndianJOphthalmol65101030-3506303 094423Document3 pagesIndianJOphthalmol65101030-3506303 094423Asif Faraz NasirNo ratings yet
- Ref Error ChildrenDocument3 pagesRef Error ChildrenAdriana gonzalezNo ratings yet
- Optical Coherence Tomography Findings of Falciform Retinal Detachment Complicated With Persistent Fetal VasculatureDocument5 pagesOptical Coherence Tomography Findings of Falciform Retinal Detachment Complicated With Persistent Fetal VasculatureAgus SaifudinNo ratings yet
- Cortical Reorganization After Optical Alignment in Strabismic Patients Outside of Critical PeriodDocument13 pagesCortical Reorganization After Optical Alignment in Strabismic Patients Outside of Critical PeriodJonathan GrandasNo ratings yet
- Background: FrequencyDocument10 pagesBackground: FrequencyJenylia HapsariNo ratings yet
- A Rare Presentation of Esotropia in High Myopia in A Young AdultDocument3 pagesA Rare Presentation of Esotropia in High Myopia in A Young AdultTinara HusniaNo ratings yet
- Gilbert y Wu Li, 2012Document7 pagesGilbert y Wu Li, 2012Sara GRNo ratings yet
- Optical Correction of Aphakia in Children: Review ArticleDocument12 pagesOptical Correction of Aphakia in Children: Review Articleaisa mutiaraNo ratings yet
- Barangay Annual Gender and Development (Gad) Plan and BudgetDocument2 pagesBarangay Annual Gender and Development (Gad) Plan and BudgetYham-Lloyd AbordoNo ratings yet
- Accuracy of The Demirjian and Willems MethodsDocument8 pagesAccuracy of The Demirjian and Willems MethodsProfessor T. A. EsanNo ratings yet
- Focus Group Design and Group Dynamics: Lessons From Deaf and Hard of Hearing ParticipantsDocument5 pagesFocus Group Design and Group Dynamics: Lessons From Deaf and Hard of Hearing ParticipantsmeeehNo ratings yet
- 为什么饮食失调很难治疗Document4 pages为什么饮食失调很难治疗Victoria TangNo ratings yet
- The Ainorian CompendiumDocument300 pagesThe Ainorian Compendiumlennoxmurray60100% (3)
- Nejmcp 1903768Document9 pagesNejmcp 1903768EriC. ChaN.No ratings yet
- Price List ABC 28-9-2022Document13 pagesPrice List ABC 28-9-2022NgurahNo ratings yet
- Monitoring and Evaluation FormDocument5 pagesMonitoring and Evaluation Formlesterjessa castroNo ratings yet
- TN BH ABA Provider OrientationDocument34 pagesTN BH ABA Provider OrientationVivian ChenNo ratings yet
- Uma Co., Ltd. Hba1C Diluent: 2-19-6 Yokosuka Matsudo, Chiba, JapanDocument1 pageUma Co., Ltd. Hba1C Diluent: 2-19-6 Yokosuka Matsudo, Chiba, JapanTrần Văn BìnhNo ratings yet
- Yours Uk 12 March 2023Document126 pagesYours Uk 12 March 2023turricanNo ratings yet
- ADEA AADSAS General Instructions BookletDocument53 pagesADEA AADSAS General Instructions Bookletd_yuminNo ratings yet
- Love Letter PDFDocument31 pagesLove Letter PDFAlan Kintanar IIINo ratings yet
- Đề số 1Document4 pagesĐề số 1LanChiVũ0% (1)
- Resumo - SIICUSP - Ingles FinalDocument2 pagesResumo - SIICUSP - Ingles FinalSuel CostaNo ratings yet
- Reconstruction of The EarDocument10 pagesReconstruction of The EarFabian Camelo OtorrinoNo ratings yet
- Pe G 12 Melc12 2Document5 pagesPe G 12 Melc12 2Ivy Dianne Pascual100% (5)
- Advanced Nutrition Test 2023 PDFDocument3 pagesAdvanced Nutrition Test 2023 PDFajjaNo ratings yet
- Hazard Analysis and Risk Control Record: Schlumberger-PrivateDocument2 pagesHazard Analysis and Risk Control Record: Schlumberger-Privatehans vatriolisNo ratings yet
- Assignment Individual Section 42Document3 pagesAssignment Individual Section 42Afiqah YusriNo ratings yet
- Heal TH 2019 Research On Drugs Abuse - 2Document140 pagesHeal TH 2019 Research On Drugs Abuse - 2Anti NarkobaNo ratings yet
- Thesis Topics Conservative Dentistry EndodonticsDocument5 pagesThesis Topics Conservative Dentistry Endodonticsaprilfordsavannah100% (2)
- School Violence InInternational ContexDocument257 pagesSchool Violence InInternational ContexLUZ STELLA MOSQUERANo ratings yet
- Study On The Effectiveness of Using Homemade Coconut Milk With Aloe Vera As Hair ConditionerDocument9 pagesStudy On The Effectiveness of Using Homemade Coconut Milk With Aloe Vera As Hair ConditionerFrederick SantosNo ratings yet
- LOA 3rd Quarter TemplateDocument4 pagesLOA 3rd Quarter TemplateJALENE L. MASAGCANo ratings yet
- ASS Event 2-Documentation, Planning and Assessment 2Document13 pagesASS Event 2-Documentation, Planning and Assessment 2Liz LopezNo ratings yet
- Wib Brochure enDocument2 pagesWib Brochure enedsan alinsuagNo ratings yet
- Nutrition: Food Based Dietary GuidelinesDocument19 pagesNutrition: Food Based Dietary GuidelinesAbdi Khalaq Ali HashiNo ratings yet
- Ig2-Mohsin Bashir Report 2Document13 pagesIg2-Mohsin Bashir Report 2Mohsin BashirNo ratings yet