Download as pdf or txt
You might also like
- Surgical Treatment of Tarsal Coalitions in ChildrenDocument10 pagesSurgical Treatment of Tarsal Coalitions in ChildrenNegru TeodorNo ratings yet
- Laprade 2012Document11 pagesLaprade 2012Aaron BNo ratings yet
- 2002 Scarf FundaDocument9 pages2002 Scarf FundaRuth Aydeé SoláNo ratings yet
- Raccourcissement Cubitus - Acta Ortho BelgicaDocument6 pagesRaccourcissement Cubitus - Acta Ortho BelgicaLedouxNo ratings yet
- Elmoumni2012 Long-Term Functional Outcome Following Intramedullary Nailing ofDocument5 pagesElmoumni2012 Long-Term Functional Outcome Following Intramedullary Nailing ofJian Wei LowNo ratings yet
- Triple Arthrodesis in Rheumatoid ArthritisDocument5 pagesTriple Arthrodesis in Rheumatoid ArthritisZahrotul Fitria SuryawanNo ratings yet
- Estudio ComparativoDocument5 pagesEstudio ComparativoDaniel VideaNo ratings yet
- "A To P" Screw Versus Posterolateral Plate For PosteriorDocument6 pages"A To P" Screw Versus Posterolateral Plate For PosteriorErlin EsauNo ratings yet
- Realignment Surgery For Malunited Ankle Fracture: Clinical ArticleDocument5 pagesRealignment Surgery For Malunited Ankle Fracture: Clinical ArticleGio VandaNo ratings yet
- Use of Allograft in Skeletally Immature Patients For Calcaneal Neck Lengthening OsteotomyDocument5 pagesUse of Allograft in Skeletally Immature Patients For Calcaneal Neck Lengthening OsteotomyMonem ShakeerNo ratings yet
- Treatment of Hallux Valgus With An Increased Distal Metatarsal Articular Angle: Evaluation of Double and Triple First Ray OsteotomiesDocument10 pagesTreatment of Hallux Valgus With An Increased Distal Metatarsal Articular Angle: Evaluation of Double and Triple First Ray OsteotomiesmilenabogojevskaNo ratings yet
- Semiconstrained Total Elbow Arthroplasty-1Document6 pagesSemiconstrained Total Elbow Arthroplasty-1Ευαγγελια ΚιμπαρηNo ratings yet
- Foot and Ankle Surgery: A.E.E.P.M. Leeuwesteijn M.D., E. de Visser M.D., PH.D., J.W.K. Louwerens M.D., PH.DDocument6 pagesFoot and Ankle Surgery: A.E.E.P.M. Leeuwesteijn M.D., E. de Visser M.D., PH.D., J.W.K. Louwerens M.D., PH.D杨明No ratings yet
- The Modified Brostr M Gould Procedure - Early Results Usi - 2014 - Foot and AnklDocument5 pagesThe Modified Brostr M Gould Procedure - Early Results Usi - 2014 - Foot and AnklFyodorovich Makarov NikolaiNo ratings yet
- El BatrawypaperDocument7 pagesEl BatrawypaperabdallahalshallNo ratings yet
- Valgus KneeDocument12 pagesValgus KneeFahad MNo ratings yet
- 1 s2.0 S1877056810000708 Main 2Document10 pages1 s2.0 S1877056810000708 Main 2Magdalena MajNo ratings yet
- MainDocument8 pagesMainRamy ElmasryNo ratings yet
- 264 2005 Article 63Document5 pages264 2005 Article 63ruth solaNo ratings yet
- Total Hip Arthroplasty With Trochanteric Ostectomy For Patients With Angular Deformity of The Proximal FemurDocument8 pagesTotal Hip Arthroplasty With Trochanteric Ostectomy For Patients With Angular Deformity of The Proximal Femurdrbane123No ratings yet
- Outcome Assesment of Proximal Fibular Osteotomy in Medial Compartment Knee OsteoarthritisDocument3 pagesOutcome Assesment of Proximal Fibular Osteotomy in Medial Compartment Knee OsteoarthritisPrashant GuptaNo ratings yet
- Brace Treatment For Osteoarthritis of The KneeDocument7 pagesBrace Treatment For Osteoarthritis of The KneeAli MohamedNo ratings yet
- Complications and Outcomes of The Transfibular Approach For Posterolateral Fractures of The Tibial Plateau PDFDocument19 pagesComplications and Outcomes of The Transfibular Approach For Posterolateral Fractures of The Tibial Plateau PDFSergio Tomas Cortés MoralesNo ratings yet
- TKA Scope Arthrolysis Knee Surg Sports Traumatol Arthrosc 2010 Mar 18 (3) 346-351Document6 pagesTKA Scope Arthrolysis Knee Surg Sports Traumatol Arthrosc 2010 Mar 18 (3) 346-351Fayza RihastaraNo ratings yet
- Fai 2011 0818Document4 pagesFai 2011 0818Mohamed GoudaNo ratings yet
- 3 Column AnkleDocument8 pages3 Column AnkleJosé Eduardo Fernandez RodriguezNo ratings yet
- 10 - Long-Term Outcome of Planovalgus Foot Surgical Correction in Children With Cerebral PalsyDocument7 pages10 - Long-Term Outcome of Planovalgus Foot Surgical Correction in Children With Cerebral PalsyJoe MehannaNo ratings yet
- Centre of Femoral HeadDocument4 pagesCentre of Femoral Headprajwal guptaNo ratings yet
- Polesello 2014Document7 pagesPolesello 2014moonwalker2099No ratings yet
- Clinical and Radiological Outcomes of Osteoarth 2019 Orthopaedics TraumatoDocument6 pagesClinical and Radiological Outcomes of Osteoarth 2019 Orthopaedics TraumatodrelvNo ratings yet
- Foot and Ankle SurgeryDocument4 pagesFoot and Ankle SurgeryDavid GonzalezNo ratings yet
- Surgical Outcomes After Traumatic Open Knee Dislocation: Ó Springer-Verlag 2009Document6 pagesSurgical Outcomes After Traumatic Open Knee Dislocation: Ó Springer-Verlag 2009agus sukarnaNo ratings yet
- Bernarddedompsure 2010Document8 pagesBernarddedompsure 2010liearenNo ratings yet
- Endoscopic Resection of Symptomatic Osteochondroma of The Distal FemurDocument4 pagesEndoscopic Resection of Symptomatic Osteochondroma of The Distal FemurAlex CirlanNo ratings yet
- Bryan MorreyDocument5 pagesBryan MorreyokisutartoNo ratings yet
- 1345-Texto Del Artículo-26226-1-10-20211009Document8 pages1345-Texto Del Artículo-26226-1-10-20211009Noe SaavedraNo ratings yet
- Total Hip Arthroplasty Survival in Femoral Head Avascular NecrosisDocument6 pagesTotal Hip Arthroplasty Survival in Femoral Head Avascular NecrosisCleff FlowersNo ratings yet
- 10 1016@j Arthro 2006 07 006Document8 pages10 1016@j Arthro 2006 07 006YoshitaNo ratings yet
- Paper 38Document6 pagesPaper 38Dr Vineet KumarNo ratings yet
- The Advantages of Circular External FixaDocument6 pagesThe Advantages of Circular External FixaPriscilla PriscillaNo ratings yet
- Treatment of Distal Humerus FracturedDocument10 pagesTreatment of Distal Humerus Fracturedauliya ningsihNo ratings yet
- Artrosis Glenohumeral Despues de Artroscopia Bankart Repair A Long-Term Follow-Up of 13 YearsDocument6 pagesArtrosis Glenohumeral Despues de Artroscopia Bankart Repair A Long-Term Follow-Up of 13 Yearsmarcelogascon.oNo ratings yet
- Age-Based Outcomes of Cheilectomy For The Treatment of Hallux RigidusDocument6 pagesAge-Based Outcomes of Cheilectomy For The Treatment of Hallux RigidusmilenabogojevskaNo ratings yet
- Open Ankle Arthrodesis A Retrospective Analysis CDocument6 pagesOpen Ankle Arthrodesis A Retrospective Analysis Ctomas.rabyNo ratings yet
- AAOS Foot Ankle 2018abDocument54 pagesAAOS Foot Ankle 2018abFasa Roshada100% (3)
- Journal Reading: Dr. Firdaus RamliDocument22 pagesJournal Reading: Dr. Firdaus RamliBell SwanNo ratings yet
- Prospective Comparison of Subtalar Arthroereisis With Lateral Column Lengthening For Painful FlatfeetDocument9 pagesProspective Comparison of Subtalar Arthroereisis With Lateral Column Lengthening For Painful FlatfeetKeren SanchezNo ratings yet
- Staged Protocol For Initial Management of The Dislocated KneeDocument8 pagesStaged Protocol For Initial Management of The Dislocated KneePerez TerrazasNo ratings yet
- High Tibial Osteotomy For Osteoarthritis of The KneeDocument6 pagesHigh Tibial Osteotomy For Osteoarthritis of The Kneealyek92No ratings yet
- Hip Arthroplasty in Failed Intertrochanteric Fract 103652Document6 pagesHip Arthroplasty in Failed Intertrochanteric Fract 103652seatrrtleNo ratings yet
- Evaluation of The Results From Surgical Treatment of The Terrible Triad of The ElbowDocument8 pagesEvaluation of The Results From Surgical Treatment of The Terrible Triad of The ElbowBruno FellipeNo ratings yet
- Intramedullary Nailing of Distal Metaphyseal.5Document9 pagesIntramedullary Nailing of Distal Metaphyseal.5Joël Clarck EkowongNo ratings yet
- 264 2013 Article 2012Document10 pages264 2013 Article 2012Monika Diaz KristyanindaNo ratings yet
- Ankle Arthrodesis After Severe InfectionDocument5 pagesAnkle Arthrodesis After Severe InfectionSeagate PramonoNo ratings yet
- Functiuonal Out5come After Sugical Tratment of Ankle Fracture Using Baird Jackon ScoreDocument4 pagesFunctiuonal Out5come After Sugical Tratment of Ankle Fracture Using Baird Jackon ScoreAxell C MtzNo ratings yet
- The Journal of Arthroplasty: SciencedirectDocument12 pagesThe Journal of Arthroplasty: SciencedirectAlid AnwarNo ratings yet
- Ankle Stabilization With Arthroscopic Versus Open With Suture Tape Augmentation Techniques X1D XJ. George DeVries PDFDocument5 pagesAnkle Stabilization With Arthroscopic Versus Open With Suture Tape Augmentation Techniques X1D XJ. George DeVries PDFcrpcsxfdkgNo ratings yet
- Nonoperative TreatmentDocument6 pagesNonoperative TreatmentGorkaBuesaNo ratings yet
- Ankle Distraction Arthroplasty A Survivorship RevDocument9 pagesAnkle Distraction Arthroplasty A Survivorship RevmirandaroydsNo ratings yet
- Disorders of the Patellofemoral Joint: Diagnosis and ManagementFrom EverandDisorders of the Patellofemoral Joint: Diagnosis and ManagementNo ratings yet
- Acetabular Fractures in Older Patients: Assessment and ManagementFrom EverandAcetabular Fractures in Older Patients: Assessment and ManagementTheodore T. MansonNo ratings yet
- Mathew 2017Document12 pagesMathew 2017Negru TeodorNo ratings yet
- Posterior Tibial Tendon Dysfunction - What Does The Single Heel Raise Test Mean in AssessmentDocument8 pagesPosterior Tibial Tendon Dysfunction - What Does The Single Heel Raise Test Mean in AssessmentNegru TeodorNo ratings yet
- Double Medial Malleolus A New Physical Findingin TalocalcanealcoalitionDocument6 pagesDouble Medial Malleolus A New Physical Findingin TalocalcanealcoalitionNegru TeodorNo ratings yet
- How To Read A Postoperative Knee Replacement RadiographDocument9 pagesHow To Read A Postoperative Knee Replacement RadiographNegru TeodorNo ratings yet
- Dupuytren Disease and Related PDFDocument418 pagesDupuytren Disease and Related PDFNegru TeodorNo ratings yet
- Axial DeformityDocument58 pagesAxial DeformitynishantsinghbmeNo ratings yet
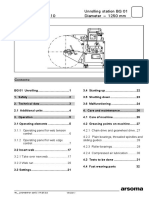
- Unwinding StationDocument34 pagesUnwinding StationDeniMestiWidiantoNo ratings yet
- SF 2940 FormsDocument23 pagesSF 2940 FormsdeekshaNo ratings yet
- AE1222 2021 GROUP E10E WingDesignReportDocument100 pagesAE1222 2021 GROUP E10E WingDesignReportBowmigowNo ratings yet
- User Instructions: Domestic Garage Door OperatorsDocument16 pagesUser Instructions: Domestic Garage Door OperatorsJack Smith100% (1)
- Chapter 1 2 Automated Water Billing System093015Document19 pagesChapter 1 2 Automated Water Billing System093015Nicholson Zapanta100% (1)
- Trinabh Shridhar - Individual Quiz CompletedDocument11 pagesTrinabh Shridhar - Individual Quiz CompletedSneha DhamijaNo ratings yet
- DomesDocument14 pagesDomesKarthikeya SarmaNo ratings yet
- QCVN 09 2017 BXD ENGLISH Unofficial Translation by VGBCDocument20 pagesQCVN 09 2017 BXD ENGLISH Unofficial Translation by VGBCTrần TùngNo ratings yet
- Lab01 Exercise LinuxDocument7 pagesLab01 Exercise LinuxBhupinder SharmaNo ratings yet
- MacroDocument15 pagesMacroanonyme3897No ratings yet
- Lesson 7 Networking DevicesDocument4 pagesLesson 7 Networking DevicesSara Jane CorpuzNo ratings yet
- ArticulatorsDocument73 pagesArticulatorsharshiniNo ratings yet
- Archer (1967) Rayleigh Random Variables PDFDocument36 pagesArcher (1967) Rayleigh Random Variables PDFHector Fabio Gallego EscuderoNo ratings yet
- Lab Report A763319Document7 pagesLab Report A763319David EvansNo ratings yet
- Course Structure and Syllabus UG - R20: Cse - Artificial Intelligence & Data ScienceDocument40 pagesCourse Structure and Syllabus UG - R20: Cse - Artificial Intelligence & Data ScienceSumanth 7899No ratings yet
- Shotpeeningofsteel Specification (Parts-: Indian StandardDocument11 pagesShotpeeningofsteel Specification (Parts-: Indian StandardVivekNo ratings yet
- Delirium in Elderly Patients - Prospective Prevalence Across Hospital Services-2020Document7 pagesDelirium in Elderly Patients - Prospective Prevalence Across Hospital Services-2020Juan ParedesNo ratings yet
- Be Itc MCQ 675263Document18 pagesBe Itc MCQ 675263سيناء الحبيبةNo ratings yet
- Pressure and Friction Drag I: Fluid Flow About Immersed ObjectsDocument11 pagesPressure and Friction Drag I: Fluid Flow About Immersed ObjectsBi BiNo ratings yet
- Worm Rollin PDFDocument6 pagesWorm Rollin PDFanon_517822417No ratings yet
- Compressor: HATLAPA Water-Cooled Piston Compressor W30, W40Document2 pagesCompressor: HATLAPA Water-Cooled Piston Compressor W30, W40Vanas ShahNo ratings yet
- 2021 Grade 12 Science Paper 1 End of Term 1 TestDocument5 pages2021 Grade 12 Science Paper 1 End of Term 1 TestDavies MasumbaNo ratings yet
- Configuring Tomcat To Work With IISDocument3 pagesConfiguring Tomcat To Work With IISWill Wolff-MyrenNo ratings yet
- Running Minio in Minikube GitHubDocument4 pagesRunning Minio in Minikube GitHubJuan Carlos AlvarezNo ratings yet
- 6B Advanced Gas Path (AGP) : Output, Efficiency, and Availability SolutionDocument1 page6B Advanced Gas Path (AGP) : Output, Efficiency, and Availability SolutionMahesh MishraNo ratings yet
- Department of Electrical Engineering (New Campus) : LAB 5: JFET and MOSFET (DC Biasing Review)Document10 pagesDepartment of Electrical Engineering (New Campus) : LAB 5: JFET and MOSFET (DC Biasing Review)syed furqan javedNo ratings yet
- VCF Anhydrous Ammonia (NH3)Document4 pagesVCF Anhydrous Ammonia (NH3)Edgar GuardiaNo ratings yet
- Zaha HadidDocument14 pagesZaha Hadidjanhavi28No ratings yet
- Non IdealDocument29 pagesNon IdealAmin SyazrinNo ratings yet
- Improving The Performance and Bandwidth EfficiencyDocument12 pagesImproving The Performance and Bandwidth EfficiencyalexNo ratings yet