Download as docx, pdf, or txt
You might also like
- 1701Document6 pages1701Dolly BringasNo ratings yet
- Migraine - More Than A HeadacheDocument11 pagesMigraine - More Than A HeadacheLuma De Fátima Louro AitaNo ratings yet
- Migraine Patient HandoutDocument14 pagesMigraine Patient HandoutthiautamiNo ratings yet
- Final - Thesis Paper 1Document35 pagesFinal - Thesis Paper 1api-481780857No ratings yet
- Human Body QuizDocument9 pagesHuman Body QuizAnoshaNo ratings yet
- Central Nervous System Acting Drugs in Treatment of Migraine HeadacheDocument15 pagesCentral Nervous System Acting Drugs in Treatment of Migraine HeadacheDr. Kaushal Kishor SharmaNo ratings yet
- Common Headache: English Village, Gulan Street, Erbil, Kurdistan Region of IraqDocument6 pagesCommon Headache: English Village, Gulan Street, Erbil, Kurdistan Region of IraqIlyes FerenczNo ratings yet
- The Relationship Between Mind and Brain. Mental Illnesses Have Historically Been Distinguished From Other Medical Illnesses Because They AffectDocument5 pagesThe Relationship Between Mind and Brain. Mental Illnesses Have Historically Been Distinguished From Other Medical Illnesses Because They AffectSylivester PhaustineNo ratings yet
- The Relationship Between Mind and Brain. Mental Illnesses Have Historically Been Distinguished From Other Medical Illnesses Because They AffectDocument5 pagesThe Relationship Between Mind and Brain. Mental Illnesses Have Historically Been Distinguished From Other Medical Illnesses Because They AffectSylivester PhaustineNo ratings yet
- Investigacion Del Sistema NerviosoDocument29 pagesInvestigacion Del Sistema NerviosoheidyNo ratings yet
- 7 - Headache and Facial Pain Lecture - 1Document21 pages7 - Headache and Facial Pain Lecture - 1Ranjit Sharma0% (1)
- Neuro Assignment Himanshi Sumrani 1073 Maclp 3bDocument22 pagesNeuro Assignment Himanshi Sumrani 1073 Maclp 3bhimsumraniNo ratings yet
- Meningitis Ein 3Document42 pagesMeningitis Ein 3Rifqi FuadiNo ratings yet
- MaryamDahooei AyurvedicapproachestomigraineheadacheDocument19 pagesMaryamDahooei AyurvedicapproachestomigraineheadacheVilas BhuwadNo ratings yet
- Nursing 1 - Workshop 6Document9 pagesNursing 1 - Workshop 6GINA NAYIBTH LEON VIDALNo ratings yet
- Neuropsychology NotesDocument26 pagesNeuropsychology NotesLiviaNo ratings yet
- Pathology of SeizuresDocument13 pagesPathology of SeizuresZachary CohenNo ratings yet
- Wala Pa Conclusion ToDocument17 pagesWala Pa Conclusion ToLapitan Jared Anne S.No ratings yet
- Migraine Is A CommonDocument11 pagesMigraine Is A CommonajenkajenkNo ratings yet
- LO 18 Pain Pathways and Pharma MGT OADocument4 pagesLO 18 Pain Pathways and Pharma MGT OAhbgossNo ratings yet
- The Brain Is So Important To Our HealthDocument5 pagesThe Brain Is So Important To Our Healthmichpagsuyuin14No ratings yet
- NPA Intro - Assignment Re-DeditedDocument11 pagesNPA Intro - Assignment Re-DeditedParamesh WaranNo ratings yet
- Research Paper Topics NeurologyDocument5 pagesResearch Paper Topics Neurologyafeawjjwp100% (1)
- CH Dreaming NeurogenesisDocument31 pagesCH Dreaming NeurogenesisrommelsousaNo ratings yet
- On Head AcheDocument27 pagesOn Head Achesarath p rajuNo ratings yet
- Headache: Prepared byDocument46 pagesHeadache: Prepared byBahaa ShaabanNo ratings yet
- Migraine - A Comprehensive GuideDocument29 pagesMigraine - A Comprehensive GuideNatalie Mbonjani100% (1)
- Epilepsy - Disease Management-Notes - Compressed-1-25Document25 pagesEpilepsy - Disease Management-Notes - Compressed-1-25Ahsan kamalNo ratings yet
- Neurological DisorderDocument10 pagesNeurological DisordersonyNo ratings yet
- Background: Migraine ClassificationDocument12 pagesBackground: Migraine ClassificationPingkan Maria RuntuweneNo ratings yet
- Headache - Migraine: Dr.S.Pranavendra Nath, Junior Resident, Dept. of Internal Medicine, Kims & RFDocument62 pagesHeadache - Migraine: Dr.S.Pranavendra Nath, Junior Resident, Dept. of Internal Medicine, Kims & RFpurnaNo ratings yet
- Pelzer Et Al 2023 Neurological and Psychiatric Comorbidities of Migraine Concepts and Future PerspectivesDocument15 pagesPelzer Et Al 2023 Neurological and Psychiatric Comorbidities of Migraine Concepts and Future Perspectivespaulo gutierrezNo ratings yet
- Headache: Paul G. Mathew, M.D., and Ivan Garza, M.DDocument13 pagesHeadache: Paul G. Mathew, M.D., and Ivan Garza, M.DElizabeth PedruezaNo ratings yet
- Managing and Preventing Migraine in The Emergency Department A ReviewDocument20 pagesManaging and Preventing Migraine in The Emergency Department A ReviewdedeadamNo ratings yet
- Migraine Headaches - University of Maryland Medical Center PDFDocument22 pagesMigraine Headaches - University of Maryland Medical Center PDFAl Hasyr SarminNo ratings yet
- 21st Century Solutions To DepressionDocument178 pages21st Century Solutions To DepressionGustavo Silva0% (1)
- MigraineDocument3 pagesMigraineFarhan NaseemNo ratings yet
- (Contemporary Clinical Neuroscience) Giuliana Grimaldi, Mario Manto (auth.), Giuliana Grimaldi, Mario Manto (eds.)-Mechanisms and Emerging Therapies in Tremor Disorders-Springer-Verlag New York (2013).pdfDocument490 pages(Contemporary Clinical Neuroscience) Giuliana Grimaldi, Mario Manto (auth.), Giuliana Grimaldi, Mario Manto (eds.)-Mechanisms and Emerging Therapies in Tremor Disorders-Springer-Verlag New York (2013).pdfDanalachi Adrian100% (2)
- Pathophysiology of Headache PDFDocument2 pagesPathophysiology of Headache PDFJoshua Christian TopahNo ratings yet
- Neurotransmitters and How They're Related To Depression - : By: Salma El-HossanDocument6 pagesNeurotransmitters and How They're Related To Depression - : By: Salma El-HossanSalma El-hossanNo ratings yet
- Migraña 1Document5 pagesMigraña 1Charbel Rodrigo Gonzalez SosaNo ratings yet
- Literature Review 1Document7 pagesLiterature Review 1api-549444062No ratings yet
- Migraine Headaches: PubertyDocument14 pagesMigraine Headaches: Pubertyswitgil28No ratings yet
- Epilepsy and Seizures - National Institute of Neurological Disorders and StrokeDocument12 pagesEpilepsy and Seizures - National Institute of Neurological Disorders and StrokevinnythewaliaNo ratings yet
- Workshop 6 - Nursing 1 - Semb 2020Document7 pagesWorkshop 6 - Nursing 1 - Semb 2020GINA NAYIBTH LEON VIDALNo ratings yet
- Headache What Is A Headache?: Tension Headaches Are The Most Common Type of Primary Headache. Up To 90%Document12 pagesHeadache What Is A Headache?: Tension Headaches Are The Most Common Type of Primary Headache. Up To 90%Laurensius Ivan SekaiNo ratings yet
- Aura PathophysiologyDocument10 pagesAura PathophysiologyRenju KuriakoseNo ratings yet
- Intralipid infusion for Myelin Sheath Repair in Multiple Sclerosis and Trigeminal Neuralgia?From EverandIntralipid infusion for Myelin Sheath Repair in Multiple Sclerosis and Trigeminal Neuralgia?No ratings yet
- Perspectives in Abnormal PsychologyDocument37 pagesPerspectives in Abnormal Psychologyzeynub.khan12No ratings yet
- Guarin, Consuelito Danzelle G. PHARM 1-C 0994 Pathophysiology of Nervous SystemDocument9 pagesGuarin, Consuelito Danzelle G. PHARM 1-C 0994 Pathophysiology of Nervous SystemChelito GuarinNo ratings yet
- 1 Neuropsychiatry of HeadacheDocument6 pages1 Neuropsychiatry of HeadachepriyadikkalaNo ratings yet
- Biology Investigatory Project Class 12thDocument20 pagesBiology Investigatory Project Class 12thsupercelldarshil100% (1)
- Headache NewDocument17 pagesHeadache NewHaris PeaceNo ratings yet
- What Is Trigeminal Neuralgia?Document4 pagesWhat Is Trigeminal Neuralgia?Tiger_2011No ratings yet
- Journal TetanusDocument10 pagesJournal TetanusWinariieeyy NayyNo ratings yet
- Gender and MigraineFrom EverandGender and MigraineAntoinette Maassen van den BrinkNo ratings yet
- Bailey Chase H. Miller Alfredo S. Archilla Chapter 19 Headache and Facial PainDocument15 pagesBailey Chase H. Miller Alfredo S. Archilla Chapter 19 Headache and Facial PainYuniParaditaDjunaidiNo ratings yet
- Headache and Other Craniofacial PainsDocument53 pagesHeadache and Other Craniofacial PainsIon UngureanuNo ratings yet
- P1 Types of HeadacheDocument8 pagesP1 Types of Headachebujor2000ajaNo ratings yet
- Collection of Quotes of Personal Experiences After Antipsychotic Drugs Most Specifically Risperidone and OlanzapineDocument31 pagesCollection of Quotes of Personal Experiences After Antipsychotic Drugs Most Specifically Risperidone and Olanzapinepat789963No ratings yet
- How To Get Started With Writing AssignmentsDocument1 pageHow To Get Started With Writing AssignmentsAngelaNo ratings yet
- Semester CalendarDocument1 pageSemester CalendarAngelaNo ratings yet
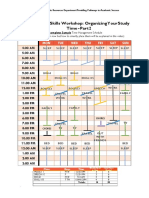
- Study Skills Wkshop - Organizing Your Time 2Document1 pageStudy Skills Wkshop - Organizing Your Time 2AngelaNo ratings yet
- Great Ways To StudyDocument4 pagesGreat Ways To StudyAngelaNo ratings yet
- Cornell Note-Taking SystemDocument1 pageCornell Note-Taking SystemAngelaNo ratings yet
- Cornell Note-Taking MethodDocument2 pagesCornell Note-Taking MethodAngelaNo ratings yet
- Cornell Note-Taking MethodDocument2 pagesCornell Note-Taking MethodAngelaNo ratings yet
- 1e University CornellDocument2 pages1e University CornellAngelaNo ratings yet
- LBP RoutineDocument6 pagesLBP RoutineAngelaNo ratings yet
- 1 Printable NoteDocument1 page1 Printable NoteAngelaNo ratings yet
- Used Car BuyingDocument11 pagesUsed Car BuyingAngelaNo ratings yet
- (Exergame) Wounded Warrior Project Uses TWallDocument1 page(Exergame) Wounded Warrior Project Uses TWallAngelaNo ratings yet
- Fit Over 40 GuideDocument29 pagesFit Over 40 GuideAngelaNo ratings yet
- 2 Googles 8 RulesDocument1 page2 Googles 8 RulesAngelaNo ratings yet
- (Toni) TX MS W Chinese Scalp AcupDocument16 pages(Toni) TX MS W Chinese Scalp AcupAngelaNo ratings yet
- Toni (Zhu Scalp Acup)Document4 pagesToni (Zhu Scalp Acup)AngelaNo ratings yet
- Chinese Scalp Acup (Military Cases)Document4 pagesChinese Scalp Acup (Military Cases)AngelaNo ratings yet
- Scalp AcupunctureDocument11 pagesScalp AcupunctureAngelaNo ratings yet
- Green Smoothie RecipesDocument12 pagesGreen Smoothie RecipesAngelaNo ratings yet
- Christian Wealth BuildingDocument158 pagesChristian Wealth BuildingAngelaNo ratings yet
- 5 Mag PhosDocument8 pages5 Mag PhosAngelaNo ratings yet
- Steve F. Carlisle,: Professional SummaryDocument5 pagesSteve F. Carlisle,: Professional SummaryRickey StokesNo ratings yet
- B1 Questions QN001: Form Questions Which Ask For The Underlined WordsDocument2 pagesB1 Questions QN001: Form Questions Which Ask For The Underlined WordsMirjana Paunovic100% (1)
- Penerapan Sistem Haccp Jurusan Gizi Poltekkes Kemenkes MalangDocument3 pagesPenerapan Sistem Haccp Jurusan Gizi Poltekkes Kemenkes MalangGita Martha VIndiartiNo ratings yet
- Three Winding or Tertiary Winding TransformerDocument7 pagesThree Winding or Tertiary Winding TransformergopalakrishnanNo ratings yet
- (Ebook - pdf.NsO) (Martial - Arts) Seven - Habits.of - Highly.successful - Martial.artists (WWW - Northshare.tk)Document6 pages(Ebook - pdf.NsO) (Martial - Arts) Seven - Habits.of - Highly.successful - Martial.artists (WWW - Northshare.tk)riffkiNo ratings yet
- Rhenogran Short Fiber Reinforcement For Rubber A4!04!2017Document6 pagesRhenogran Short Fiber Reinforcement For Rubber A4!04!2017vlabat2017No ratings yet
- Presentation On Solid Waste ManagementDocument14 pagesPresentation On Solid Waste ManagementRajesh HarmukhNo ratings yet
- The Together TeacherDocument4 pagesThe Together TeacherTeachers Without BordersNo ratings yet
- Sample QuestionnaireDocument5 pagesSample QuestionnaireAudi Kyle SaydovenNo ratings yet
- Chem Jeem SeptDocument62 pagesChem Jeem SeptStephen SatwikNo ratings yet
- Approach To Neonatal HyperbilirubinemiaDocument34 pagesApproach To Neonatal HyperbilirubinemiaNilesh HatzadeNo ratings yet
- Shani Taub: Certified Dietary Consultant 732-300-8541, 732-364-7392Document1 pageShani Taub: Certified Dietary Consultant 732-300-8541, 732-364-7392henny bandaNo ratings yet
- Andhashraddha Nirmoolan Samiti Newsletter For September 2011 (VastuShastra Special Issue)Document36 pagesAndhashraddha Nirmoolan Samiti Newsletter For September 2011 (VastuShastra Special Issue)MaharashtraAnisNo ratings yet
- Removable Guardrail SystemsDocument3 pagesRemovable Guardrail SystemsSaiful AnnasNo ratings yet
- 2023.08.08 - Letter To AUSA GravesDocument2 pages2023.08.08 - Letter To AUSA GravesNew York PostNo ratings yet
- NCP Risk For InfectionDocument1 pageNCP Risk For InfectionBianca MaeNo ratings yet
- Dissolution of Calcium Carbonate in Aqueous Solutions of Acetic AcidDocument3 pagesDissolution of Calcium Carbonate in Aqueous Solutions of Acetic AcidMichelle M. SalvadorNo ratings yet
- Stainless Steel CatalogueDocument109 pagesStainless Steel Cataloguelingot123@yahoo.comNo ratings yet
- Excavation and Shoring SH-2012-23eDocument5 pagesExcavation and Shoring SH-2012-23eshamroz khan100% (1)
- Respiratory Pathology IiDocument37 pagesRespiratory Pathology IiPutraNo ratings yet
- Eti Final MPDocument19 pagesEti Final MPAstel DmelloNo ratings yet
- UK DynaSand C0209Document2 pagesUK DynaSand C0209Mee DepoNo ratings yet
- Ridf.Document21 pagesRidf.Syam KrishnanNo ratings yet
- Random TeachingsDocument148 pagesRandom TeachingsabcjohnNo ratings yet
- Compatibility Testing - BloodDocument5 pagesCompatibility Testing - BloodMunish DograNo ratings yet
- Primary Frca Help Plain UpdatedDocument5 pagesPrimary Frca Help Plain UpdatedDavid PappinNo ratings yet
- 720 Pds-Dromus BDocument2 pages720 Pds-Dromus BSAEFUDDIN SAEFUDDINNo ratings yet
- 003 Donkey Table N StickDocument7 pages003 Donkey Table N StickRonnie BrayNo ratings yet
- Hayagreeva - Pudding Prepared Using Split Chik PeasDocument8 pagesHayagreeva - Pudding Prepared Using Split Chik PeasSampathKumarGodavarthiNo ratings yet