Download as pdf or txt
You might also like
- Test Bank For Oral Pharmacology For The Dental Hygienist 2nd Edition 2 e Mea A Weinberg Cheryl Westphal Theile James Burke FineDocument16 pagesTest Bank For Oral Pharmacology For The Dental Hygienist 2nd Edition 2 e Mea A Weinberg Cheryl Westphal Theile James Burke Finexavianhatmgzmz9No ratings yet
- Vol 51 No 2 01 Prevalence Med PDFDocument4 pagesVol 51 No 2 01 Prevalence Med PDFJustin VergaraNo ratings yet
- Oman Pharmacist Licensing Exam McqsDocument186 pagesOman Pharmacist Licensing Exam McqsMuhammad Amin100% (6)
- Lecture-09 Dose-Response RelationshipsDocument10 pagesLecture-09 Dose-Response RelationshipsChian WrightNo ratings yet
- PDF Manikanta J K TDocument60 pagesPDF Manikanta J K TSAURABH SINGHNo ratings yet
- Medication ErrorDocument7 pagesMedication ErrorLenny SucalditoNo ratings yet
- Medication ErrorDocument19 pagesMedication ErrorEvitaIrmayantiNo ratings yet
- WilliamsDocument4 pagesWilliamsRajesh KumarNo ratings yet
- MEdication ErrorsDocument6 pagesMEdication ErrorsBeaCeeNo ratings yet
- Medication Errors: What They Are, How They Happen, and How To Avoid ThemDocument9 pagesMedication Errors: What They Are, How They Happen, and How To Avoid ThemMoisesNo ratings yet
- American Academy of Pediatrics: PEDIATRICS Vol. 102 No. 2 August 1998Document5 pagesAmerican Academy of Pediatrics: PEDIATRICS Vol. 102 No. 2 August 1998Jemimah MejiaNo ratings yet
- Medication Safety: Mita Restinia, M.Farm, AptDocument57 pagesMedication Safety: Mita Restinia, M.Farm, Apt094DNORMINo ratings yet
- Medication Errors: P AperDocument4 pagesMedication Errors: P Aperdesk ayu okaNo ratings yet
- Social Pharmacy: Medication ErrorsDocument62 pagesSocial Pharmacy: Medication ErrorsEmmanuel KingsNo ratings yet
- Medication Errors in The United States and How To Improve Simple Mistakes 1Document7 pagesMedication Errors in The United States and How To Improve Simple Mistakes 1api-681331537No ratings yet
- Medication ErrorsDocument15 pagesMedication ErrorsShubhangi Sanjay KadamNo ratings yet
- Medication Error 2017Document51 pagesMedication Error 2017Christina100% (1)
- Medication SafetyDocument54 pagesMedication SafetyJuwitaASih100% (2)
- Medication ErrorsDocument10 pagesMedication Errorsjuliana bNo ratings yet
- Medication Errors Their Causative and Preventive Factors2.Doc 1Document11 pagesMedication Errors Their Causative and Preventive Factors2.Doc 1Mary MannNo ratings yet
- Figure 1. Indicator Framework of The Medication Error (Nerich Et Al., 2010)Document3 pagesFigure 1. Indicator Framework of The Medication Error (Nerich Et Al., 2010)balqiswulanNo ratings yet
- Medication Errors in Nursing 1Document6 pagesMedication Errors in Nursing 1Komal TanveerNo ratings yet
- The Epidemiology of Medication Errors: The Methodological DifficultiesDocument7 pagesThe Epidemiology of Medication Errors: The Methodological DifficultiesgabyvaleNo ratings yet
- Module 7: Medication Errors and Risk Reduction: Learning OutcomesDocument5 pagesModule 7: Medication Errors and Risk Reduction: Learning OutcomesShaina JavierNo ratings yet
- Med Errors OldDocument1 pageMed Errors OldAnonymous XvwKtnSrMRNo ratings yet
- TareDocument25 pagesTaremelkamu AssefaNo ratings yet
- Medication ErrorsDocument7 pagesMedication ErrorsNelly CheptooNo ratings yet
- The Assignment On Medication Errors in A Hospital & Some Examples of Adverse Reactions and Poisoning IncidencesDocument25 pagesThe Assignment On Medication Errors in A Hospital & Some Examples of Adverse Reactions and Poisoning IncidencesGroup Of Cheaters (ফাতরা)No ratings yet
- Medication Error in TemplateDocument5 pagesMedication Error in Templateapi-283173905No ratings yet
- 395-Main Article-1737-1-10-20210603Document11 pages395-Main Article-1737-1-10-20210603فاتن محمدNo ratings yet
- Medication Errors PaperDocument6 pagesMedication Errors Paperapi-542442476No ratings yet
- Ebp 1Document4 pagesEbp 1sabitaNo ratings yet
- Medication Error-Hisfarmasi PresentationDocument102 pagesMedication Error-Hisfarmasi PresentationLaura Khristiani MarbunNo ratings yet
- Medication Administration ErrorsDocument16 pagesMedication Administration ErrorspriyaNo ratings yet
- Medication Error PDFDocument61 pagesMedication Error PDFChelsea Ritz MendozaNo ratings yet
- E151 Medicationerrors-QJMDocument10 pagesE151 Medicationerrors-QJMRestu AriyusNo ratings yet
- Safe Administrations of Medications (Draft Chapter)Document74 pagesSafe Administrations of Medications (Draft Chapter)Caleb FellowesNo ratings yet
- Preventing Medication Error Based On Knowledge Management Against Adverse EventDocument9 pagesPreventing Medication Error Based On Knowledge Management Against Adverse EventJurnal Ners UNAIRNo ratings yet
- Common Prescribing ErrorsDocument3 pagesCommon Prescribing ErrorsNadial uzmahNo ratings yet
- ASHP Guidelines On Preventing Medication Errors in HospitalsDocument9 pagesASHP Guidelines On Preventing Medication Errors in HospitalsMedarabiaNo ratings yet
- Course: Patient Safety Solutions Topic:: Some DefinitionsDocument5 pagesCourse: Patient Safety Solutions Topic:: Some DefinitionsKian GonzagaNo ratings yet
- E151 Medicationerrors-QJMDocument10 pagesE151 Medicationerrors-QJMWens BambutNo ratings yet
- What We Need To Know For Patient SafetyDocument9 pagesWhat We Need To Know For Patient SafetyhusainiNo ratings yet
- Medication Errors PaperDocument6 pagesMedication Errors Paperapi-740209346No ratings yet
- Ch. 9Document4 pagesCh. 9Prince K. TaileyNo ratings yet
- Medication Errors 3Document6 pagesMedication Errors 3api-692972467No ratings yet
- The Percentage of Medication Errors Globally, and in Saudi ArabiaDocument7 pagesThe Percentage of Medication Errors Globally, and in Saudi ArabiaLeen alghamdNo ratings yet
- MedicationerrorsDocument11 pagesMedicationerrorsIkhwanir RaisaNo ratings yet
- Background. Registered Nurses (RNS) Have A Role in The Medication Administration ProcessDocument4 pagesBackground. Registered Nurses (RNS) Have A Role in The Medication Administration ProcessEdmarkmoises ValdezNo ratings yet
- 210 1437 1 PB LibreDocument62 pages210 1437 1 PB Librezozorina21No ratings yet
- ComplianceDocument13 pagesCompliancextremist2001No ratings yet
- Reducing Medication Risks of Electronic Medication Systems: Laura A. FinnDocument9 pagesReducing Medication Risks of Electronic Medication Systems: Laura A. FinnASHISH KUMAR YADAVNo ratings yet
- Attributable To The Use of Medications (: Near MissesDocument4 pagesAttributable To The Use of Medications (: Near MissesdudijohNo ratings yet
- Evaluation of Medication Errors in Community Pharmacy Settings: A Retrospective ReportDocument4 pagesEvaluation of Medication Errors in Community Pharmacy Settings: A Retrospective ReportNicoleta CheptanariNo ratings yet
- RRL 8 Part 3Document55 pagesRRL 8 Part 3Joshua Christian Gan0% (1)
- Med Errors FinalDocument7 pagesMed Errors Finalapi-485620816No ratings yet
- Article Wjpps 1469869064Document10 pagesArticle Wjpps 1469869064Lucia SibiiNo ratings yet
- Case StudyDocument10 pagesCase StudyRezwan DihanNo ratings yet
- View of A Review On Adverse Drug Reactions Monitoring AndreportingDocument1 pageView of A Review On Adverse Drug Reactions Monitoring Andreporting9Asfara AzeezNo ratings yet
- Drug Errors: Consequences, Mechanisms, and Avoidance: Key PointsDocument7 pagesDrug Errors: Consequences, Mechanisms, and Avoidance: Key PointsRavikiran SuryanarayanamurthyNo ratings yet
- Abostrofic SytosisDocument17 pagesAbostrofic Sytosisasaad biqaiNo ratings yet
- Background: Frequency Relationship Medication Errors and Adverse Drug Events Pharmacist's Role in Medication SafetyDocument3 pagesBackground: Frequency Relationship Medication Errors and Adverse Drug Events Pharmacist's Role in Medication SafetyNono PapoNo ratings yet
- Pharmacoepidemiology, Pharmacoeconomics,PharmacovigilanceFrom EverandPharmacoepidemiology, Pharmacoeconomics,PharmacovigilanceRating: 3 out of 5 stars3/5 (1)
- List of WHO GMP Approved Manufacturers in Gujrat IndiaDocument28 pagesList of WHO GMP Approved Manufacturers in Gujrat IndiaRomana ZainNo ratings yet
- Who Trs 908-Annex9Document12 pagesWho Trs 908-Annex9Poorvi KumarNo ratings yet
- Drug Name Magnified Effects With AlcoholDocument1 pageDrug Name Magnified Effects With AlcoholMuhibpi IbrahimNo ratings yet
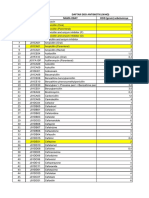
- DAFTAR ATC DDD ANTIBIOTIK WHO 2018 AbcDocument12 pagesDAFTAR ATC DDD ANTIBIOTIK WHO 2018 AbcMahezha DhewaNo ratings yet
- Código Descripción Costo Unita. Existencia Unidades Costo Existencia Precio 1 %utilDocument24 pagesCódigo Descripción Costo Unita. Existencia Unidades Costo Existencia Precio 1 %utilNiky Dos SantosNo ratings yet
- Eye Drops: Drug StudyDocument3 pagesEye Drops: Drug StudyChris PaguioNo ratings yet
- Mrs. Ailun P. Jaugan - BSN - BACTH 2024: PharmacologyDocument39 pagesMrs. Ailun P. Jaugan - BSN - BACTH 2024: Pharmacologytony montanNo ratings yet
- ScriptDocument2 pagesScriptNareshNo ratings yet
- Civic Drive, Filinvest City, Alabang 1781 Muntinlupa, PhilippinesDocument18 pagesCivic Drive, Filinvest City, Alabang 1781 Muntinlupa, Philippinesultimate_2226252No ratings yet
- Solid Dosage Form Part 1Document48 pagesSolid Dosage Form Part 1Claire Marie AlvaranNo ratings yet
- Stability StudiesDocument61 pagesStability StudiesSiddarth PalletiNo ratings yet
- BCS PrácticaDocument17 pagesBCS PrácticaEarvin GonzálezNo ratings yet
- Guideline 339 enDocument638 pagesGuideline 339 enJatin SinghNo ratings yet
- Nama Pasien Umur Waktu Tunggu Diagnosa No & TGL No. BpjsDocument18 pagesNama Pasien Umur Waktu Tunggu Diagnosa No & TGL No. BpjstriNo ratings yet
- Bourgoin Biologics MarketDocument29 pagesBourgoin Biologics Marketkohinoordas2007No ratings yet
- No. Nama Obat VEN Sediaan Harga Satuan JumlahDocument2 pagesNo. Nama Obat VEN Sediaan Harga Satuan Jumlahade rafniNo ratings yet
- Regulatory Toxicology and Pharmacology: Paul Baldrick, PHD Professor, Executive Director, Regulatory StrategyDocument6 pagesRegulatory Toxicology and Pharmacology: Paul Baldrick, PHD Professor, Executive Director, Regulatory StrategyPavanNo ratings yet
- Schedule yDocument11 pagesSchedule ySiva PrasadNo ratings yet
- LevocetirizineDocument3 pagesLevocetirizineAjayChandrakarNo ratings yet
- State Board of PharmacyDocument66 pagesState Board of PharmacyAnonymous hF5zAdvwCC100% (1)
- MarianoqueDocument8 pagesMarianoqueEunise Punzalan OprinNo ratings yet
- Blocked Stock 2100 140223Document22 pagesBlocked Stock 2100 140223Farmasi KenjeranNo ratings yet
- Medical Cannabis For Children Evidence and Recommendations Canadian Paediatric SocietyDocument22 pagesMedical Cannabis For Children Evidence and Recommendations Canadian Paediatric SocietyRegina de AlmeidaNo ratings yet
- MD Pharmacology Thesis TopicsDocument8 pagesMD Pharmacology Thesis Topicshqovwpaeg100% (1)
- DR - Joan Ramon Laporte 7feb2022Document6 pagesDR - Joan Ramon Laporte 7feb2022Heinz HurtigNo ratings yet
- Excipient Risk Assessment: Possible Approaches To Assessing The Risk Associated With Excipient FunctionDocument11 pagesExcipient Risk Assessment: Possible Approaches To Assessing The Risk Associated With Excipient FunctionKolisnykNo ratings yet
- Introduction and History of PharmacovigilanceDocument37 pagesIntroduction and History of PharmacovigilanceAmy Lon33% (3)